


Doris Hexsel1,2; Indira Valente-Bezerra1,2; Andressa Renon2; Vitor Costa Fabris1
Financial support: This study was partially funded by LMG and Brazilian Center for Studies in Dermatology
Conflict of interest: No Clinical Trials: CAAE 47353221.4.0000.5330 Ethics committee number: 5330 - HMV
How to cite this article: Hexsel D, Bezerra IV, Renon A, Fabris VC. High-intensity focused electromagnetic field treatment for cellulite. Surg Cosmet Dermatol. 2023;15:e20230191.
INTRODUCTION: High-intensity focused electromagnetic field treatment (HIFEM) uses low-frequency electromagnetic waves to induce supramaximal muscle contractions, causing muscle hypertrophy and reducing fat.
OBJECTIVE: To evaluate the effects of a HIFEM treatment for the improvement of cellulite on the buttocks.
METHODS: Thirty patients were divided into two groups that received eight or 12 HIFEM sessions on the buttocks for six weeks. We assessed the improvement in cellulite and the buttocks' global appearance through the Cellulite Severity Scale (CSS), the Global Aesthetic Improvement Scale (GAIS), and a satisfaction questionnaire. Changes in body composition were evaluated through bioimpedance and hip circumference measurements.
RESULTS: Patients from both groups improved the global appearance of their buttocks. Cellulite lesions of some patients improved, but for most patients, the improvement wasn’t great enough to change the grade on the Cellulite Severity Scale. Patient satisfaction was high and adverse events were few, minor, and transitory.
CONCLUSION: The effects of HIFEM on cellulite are subtle, as this treatment modality cannot address the fibrous septa that cause the depressed lesions of cellulite. Nevertheless, HIFEM procedures can improve the buttocks’ global appearance, enhancing the patients’ subjective perception of their cellulite.
Keywords: Cellulite; Aesthetic equipment; Electromagnetic fields
INTRODUÇÃO: O tratamento com campo eletromagnético focado de alta intensidade (HIFEM) usa ondas eletromagnéticas de baixa frequência para induzir contrações musculares, causando hipertrofia muscular e reduzindo a gordura subcutânea.
OBJETIVO: avaliar os efeitos de um tratamento com HIFEM na celulite nos glúteos.
MÉTODOS: trinta mulheres foram recrutadas e randomizadas em 2 grupos que receberam 8 ou 12 sessões de HIFEM na região dos glúteos. A celulite foi avaliada utilizando a Cellulite Severity Scale, a Global Aesthetic Improvement Scale e um questionário de satisfação. Mudanças na composição corporal foram avaliadas com bioimpedância e medidas da circunferência do quadril.
RESULTADOS: a aparência global da região glútea das pacientes melhorou com o tratamento. Houve melhora na celulite de algumas pacientes, mas para a maioria a melhora não foi grande o suficiente para resultar em uma mudança de classificação na Cellulite Severity Scale. A satisfação foi alta e os eventos adversos foram poucos, não-graves e transitórios.
CONCLUSÃO: os efeitos do tratamento com HIFEM na celulite da região glútea são sutis. Contudo, este tratamento é capaz de melhorar globalmente a aparência da região glútea, melhorando a percepção das pacientes sobre a gravidade de sua celulite.
Palavras-chave: Celulite; Equipamentos para estética; Campos eletromagnéticos
Cellulite is a skin condition characterized by depressed and raised lesions on the surface of the skin of the affected areas. Nurnberger and Muller originally described cellulite biomechanics in their paper published in 1978: the depressed lesions result from thick subcutaneous fibrous septa, while the raised areas correspond to the projection of the underlying subcutaneous fat on the skin surface.1 Cellulite affects many women, presenting most frequently on the thighs and buttocks and negatively impacting their quality of life.2,3
High-intensity focused electromagnetic field treatments (HIFEM) use low-frequency electromagnetic waves to induce supramaximal muscle contractions in the targeted areas, causing muscle strengthening and growth and lipolysis, thus reducing the thickness of the subcutaneous fat.4,5 These therapeutic effects act upon different causes of cellulite lesions and improve the overall appearance of the gluteal region.6,7
Given that HIFEM improves muscle tone, reduces subcutaneous fat, and improves the overall aspect of the buttocks, it may be an effective cellulite treatment. This study aims to assess the efficacy and safety of the HIFEM treatment for improving the cellulite of the buttocks.
Study type and location
It was a prospective, single-center, open-label trial. We recruited the participants at a research center in Porto Alegre, Brazil, and they provided written informed consent. This study followed the Good Clinical Practices, Declaration of Helsinki protocols. The local Ethics Committee of Associação Hospitalar Moinhos de Vento approved it.
The main inclusion criteria were patients aged between 18 and 60 years, with moderate cellulite on the buttocks according to the Cellulite Severity Scale (CSS),8 with cellulite grade 2 or lower on each criterion of the same scale, and body mass index (BMI) between 18.5 kg/m2 and 29.9 kg/m2. Exclusion criteria included pregnancy or lactation, the presence of implanted metallic devices (e.g., cardiac pacemaker), active infections or open wounds on the treatment area, having undergone treatment for cellulite or weight loss less than 30 days before the study, or surgical procedure (e.g., liposuction, Subcision®) less than three months before the trial.
Thirty patients were randomized into two treatment groups with 15 patients each. Group 1 received eight treatment sessions (two sessions per week for four weeks) and Group 2 received 12 treatment sessions (two sessions per week for six weeks). All the patients were evaluated at baseline (Visit 1), at week 5 (Visit 2, after receiving eight treatment sessions), and at week 7 (Visit 3, after completing 12 treatment sessions or two weeks after completing eight sessions, depending on the treatment group). We ask patients not to change their usual dietary habits and workout routines for the study to avoid changes in body composition unrelated to the therapy.
The primary outcomes of this study were the reduction of at least one grade on the cellulite of the buttocks, as assessed by the CSS after eight and 12 treatment sessions, and the frequency of adverse events. Secondary outcomes were the percentage of patients improving on the Global Aesthetic Improvement Scale (GAIS), patient satisfaction, and changes in the percentage of lean mass and hip circumference.
We used the T-Sculptor® (LMG, Laser Medical Group, Brazil) equipment for the HIFEM treatment. The therapy targeted the gluteal region, especially the gluteus maximus muscle. Patients received 30-minutes treatment sessions twice a week, at least 48 hours apart. The equipment setting used the manufacturer’s treatment protocol “Combined Training II”, combining hypertrophy training and resistance training. The intensity of the treatment employed in each session was the highest one tolerated by the patient.
We took photographs with a high-definition camera at all visits while the patients stood up straight, without voluntary contraction of the muscles of the gluteal region. The same trained evaluator took the pictures using the same camera settings, at the same place, distance, and lighting.
We assessed the cellulite of each buttock of the patients using the CSS,8 a photonumeric scale that rates the five main cellulite morphological features (depressions number, depressions depth, clinical appearance of evidently raised lesions, flaccidity, and the Nurnberger-Muller cellulite classification scale). Each criterion is rated from 0 to 3, and their total sum classifies the cellulite as mild, moderate, or severe. A consensus between two investigators graded the cellulite by reviewing the high-definition pictures of each patient. The investigators also filled out the GAIS after reviewing the pictures. When filling the GAIS, the researchers focused on the improvement of cellulite. If the buttocks’ global appearance of a patient improved due to better contour and muscle tone, but there were no changes in cellulite, the investigators rated the patient as unchanged. We assessed patients’ body composition (weight, BMI, fat percentage, and lean mass percentage) through bioimpedance. Hip circumference was measured at the largest circumference around the buttocks using a measuring tape. Patients self-reported the adverse events, and the investigators assessed them at each visit. The patients also answered a satisfaction questionnaire at each visit after the beginning of the treatment.
We chose a convenience sample of 30 patients for this study. Parametric data were described as mean ± standard deviation (SD), and non-parametric data were described as the median and interquartile range (IQR). We didn’t conduct statistical hypothesis testing because the population studied was a small non-probability sample.
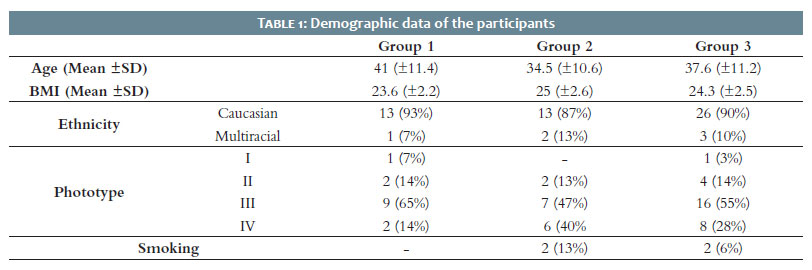
Twenty-nine of thirty patients completed the study. The dropout was one participant who found out she was pregnant the week after she was enrolled, before receiving the treatment. She was excluded from the data analysis. Table 1 shows the demographic data of the participants.
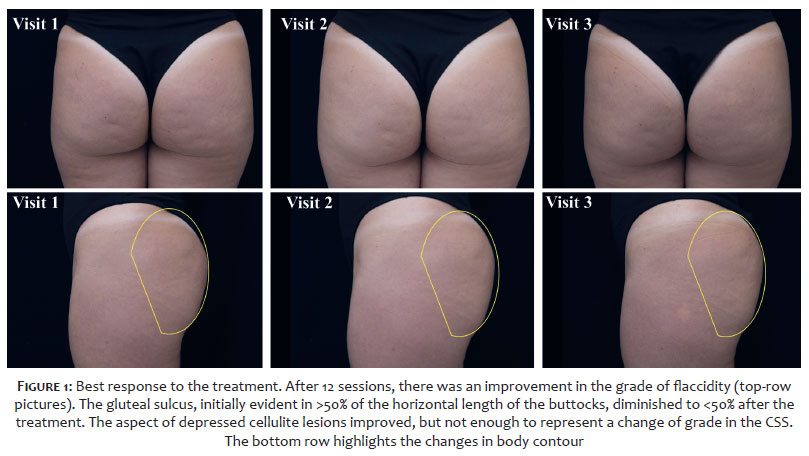
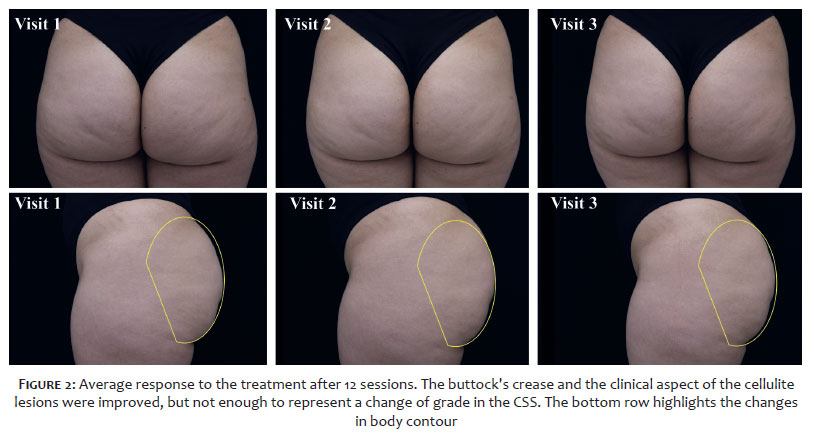
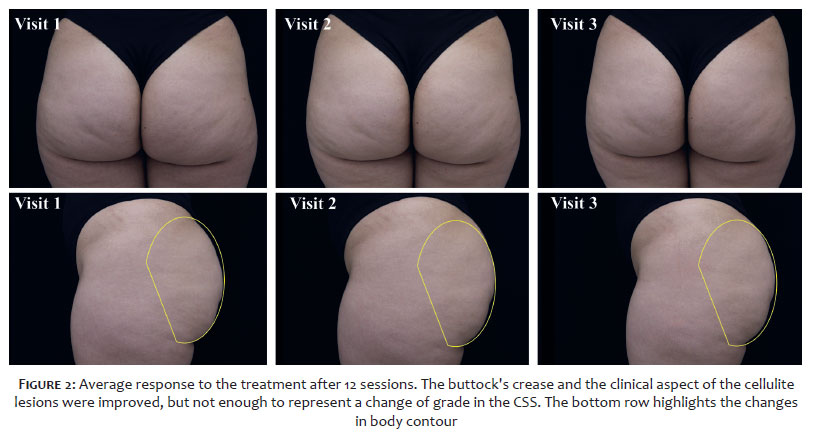
All patients enrolled in the study had moderate cellulite according to the CSS, and by the end of the study, they were all still classified as having moderate cellulite. No patient improved their grades of depressed lesions number, clinical appearance of evidently raised lesions, or Nurnberger-Muller cellulite classification scale. After Visit 3, one patient from group 1 improved their grade of flaccidity or laxity by one point on both buttocks, and another patient in the same group improved the grade of depression depth by one point on both buttocks. One patient in group 2 improved the grades of flaccidity and depression depth by one point on both buttocks. We observed no differences when comparing treatment groups. Figures 1 and 2 represent the best and average response to the treatment in our study, highlighting the improvements in flaccidity and body contour resulting from the HIFEM treatment.
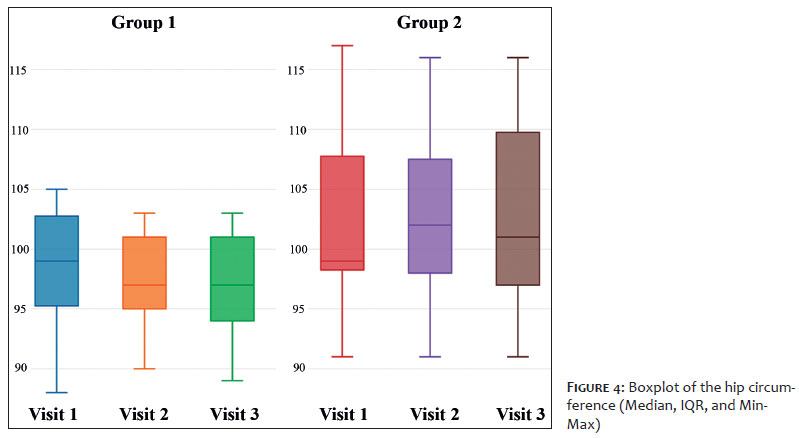
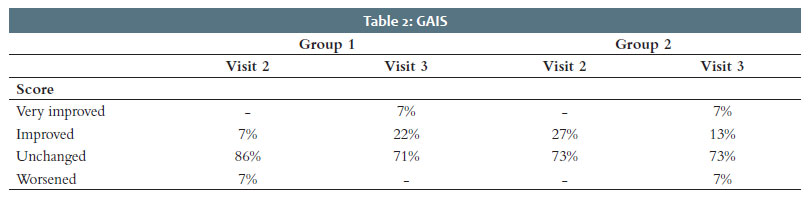
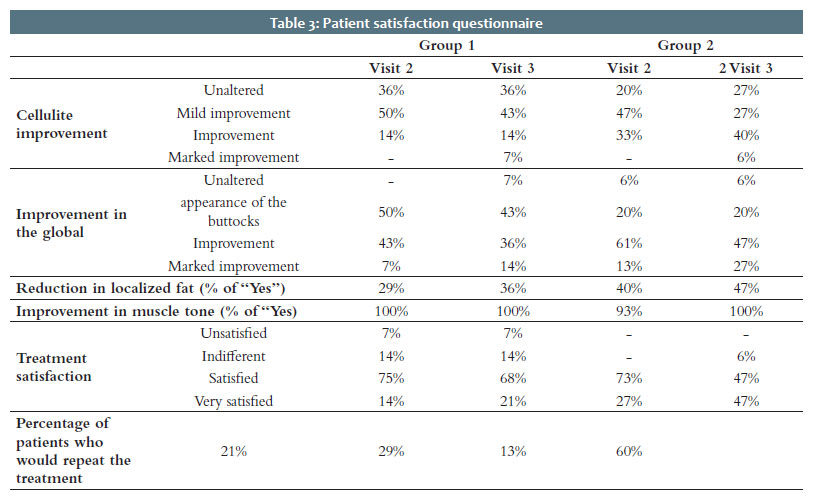
We observed no significant changes in patients’ lean mass and hip circumference percentages (Figures 3 and 4). The patients’ weight also remained stable throughout the study. One outlier from group 1 lost 5.5% of weight after the treatment, and one outlier from group two gained 4.3% of weight. All other participants lost or gained less than 3% of their body weight throughout the study. Before the treatment, the patients’ mean weight was 64.5 kg (±7.9 kg). After eight treatment sessions, the mean weight remained roughly the same: 64.4 kg (±8.0 kg). The mean weight of the group that received 12 treatment sessions changed from 67.9 kg (±7.7 kg) to 67.7 kg (±7.5 kg), also a negligible change. The mean change in weight after eight treatment sessions was -7.1 g (±996 g), and after 12 treatment sessions, it was -200 g (±896g). Given that in all previous comparisons the standard deviation was higher than the change in the mean by a fair margin, we considered the differences in weight in all groups minor and not attributed to treatment effects, as we could establish no positive or negative trends. Table 2 shows the results of the GAIS, and Table 3 presents the results of the satisfaction questionnaire.
The only adverse event reported by the patients was mild pain, which occurred in only two subjects (7%). In both cases, the adverse event was resolved in less than 24 hours.
Subcutaneous fat has paradoxical effects on cellulite. Lipolysis can improve cellulite lesions, especially the raised ones, as they result from the tension forces that the subcutaneous fat applies to the skin. The reduction of subcutaneous fat, on the other hand, has a deflation effect that worsens cellulite by aggravating skin laxity.
The most frequent cellulite lesions are depressions caused by rigid subcutaneous septa that pull the skin down9 and that can be treated by currently available Subcision® techniques.10-12 These rigid subcutaneous septa exert more traction if there is raised tension in subcutaneous space by increased fat, fillers, or muscle mass.
The effects of the HIFEM treatment in increasing muscle mass and decreasing subcutaneous fat by lipolysis, although discrete, are well-documented.4,6,7,13 Theoretically, this therapy can improve cellulite by reducing the thickness of the fat projections that cause the cellulite raised lesions by improving the buttocks’ muscle tone.
Reduced subcutaneous fat may neutralize the lifting effect of the increased muscle mass caused by HIFEM treatments. Both outcomes improve cellulite different lesions that not always coexist in the same patient. In this case, the results are antagonists. The reduction of subcutaneous fat causes some deflation degree, improving the discrete, superficial raised cellulite lesions on the buttocks,2 but at the cost of worsening skin laxity. Increased muscle mass, on the other hand, enhances the volume and causes some lifting of the buttocks, also improving some superficial cellulite lesions and cutaneous laxity. These antagonistic mechanisms explain the subtle treatment effects on cellulite found in this study.
In this study, patients demonstrated and perceived the increased muscle mass more than the lipolytic effect. However, the CSS didn’t have the required sensitivity to detect such small changes in the cellulite appearance. Only a few patients enhanced their CSS scores, and only a small percentage improved in the GAIS assessment (Table 2). The cutaneous fibrous septa, which pull the skin surface down, mainly cause the cellulite depressed lesions.1,2 However, HIFEM treatments do not affect the fibrous septa. Nevertheless, the increased muscle mass and the lipolytic effect could slightly improve cellulite.
It’s noteworthy that the perception of the patients regarding the cellulite on their buttocks was different from the perception of the evaluators. More than 90% of patients from both groups improved buttocks’ global appearance after the treatment. While the evaluators registered a cellulite improvement in less than 30% of the patients, 64% of patients in group 1 and 73% in group 2 reported an improvement in cellulite after the treatment. This discrepancy most likely results from the fact that the HIFEM treatment, even when not directly improving the cellulite lesions, can improve the buttocks’ overall appearance. This progress in the global appearance of the region leads the patient to think that their cellulite has also improved, even when the evaluators don’t report any changes in the cellulite of that area as evaluated by CSS or GAIS. It highlights that the patient’s perception of their cellulite doesn’t depend solely on the objective grade of the cellulite lesions and that treatments that improve the buttocks’ overall appearance also improve the patient’s perception of their cellulite.
Many authors have described the effects of HIFEM on raising muscle tone and mass.6,7,13,14 However, the authors didn’t find a statistically significant difference in the lean mass percentage after the treatment. As the bioimpedance device used in the evaluation grouped the muscles of the gluteal region with all the muscles of the trunk when performing this evaluation, the absolute improvement of lean mass in the buttocks was too small when considering all the muscles in the trunk. However, it’s noteworthy that 100% of the patients reported improvement in muscle tone, and 41% reported a fat reduction. Our results also showed no difference in the median hip circumference, probably because the improvement in the lean mass and the reduction in localized fat balanced each other, leading to no changes in the hip circumference despite the improvement in body contour and muscle tone.
The HIFEM technologies target muscles, improving muscle mass. Some cellulite lesions of the buttocks can improve with increased volume of the buttocks. This therapeutic modality applied to gluteus muscles can improve the buttocks’ global appearance mainly by enhancing buttocks contour, improving the patient’s subjective perception of their cellulite.
1. Nürnberger F, Müller G. So-called cellulite: an invented disease. J Dermatol Surg Oncol. 1978;4(3):221-9.
2. Hexsel D, Valente Bezerra I, Mosena G, Hexsel C. Considerations on zero-degree cellulite. J Cosmet Dermatol. 2022;21(1):134-6.
3. Soares JL, Miot HA, Sanudo A, Bagatin E. Cellulite: poor correlation between instrumental methods and photograph evaluation for severity classification. Int J Cosmet Sci. 2015;37(1):134-40.
4. Goldberg DJ, Enright KM, Goldfarb R, Katz B, Gold M. The role and clinical benefits of high-intensity focused electromagnetic devices for non-invasive lipolysis and beyond: a narrative review and position paper. J Cosmet Dermatol. 2021;20(7):2096-101.
5. Duncan D, Dinev I. Noninvasive induction of muscle fiber hypertrophy and hyperplasia: effects of high-intensity focused electromagnetic field evaluated in an in-vivo porcine model: a pilot study. Aesthet Surg J. 2020;40(5):568-74.
6. Giesse S. A german prospective study of the safety and efficacy of a non-invasive, high-intensity, electromagnetic abdomen and buttock contouring device. J Clin Aesthet Dermatol. 2021;14(1):30-3.
7. Palm M. Magnetic resonance imaging evaluation of changes in gluteal muscles after treatments with the high-intensity focused electromagnetic procedure. Dermatol Surg. 2021;47(3):386-91.
8. Hexsel DM, Dal'forno T, Hexsel CL. A validated photonumeric cellulite severity scale. J Eur Acad Dermatol Venereol. 2009;23(5):523-8.
9. Hexsel DM, Abreu M, Rodrigues TC, Soirefmann M, Prado DZ, Gamboa MM. Side-by-side comparison of areas with and without cellulite depressions using magnetic resonance imaging. Dermatol Surg. 2009;35(10):1471-7.
10. Orentreich DS, Orentreich N. Subcutaneous incisionless (subcision) surgery for the correction of depressed scars and wrinkles. Dermatol Surg. 1995;21(6):543-9.
11. Hexsel DM, Mazzuco R. Subcision: a treatment for cellulite. Int J Dermatol. 2000;39(7):539-44.
12. Kaminer MS, Coleman WP, Weiss RA, Robinson DM, Grossman J. A multicenter pivotal study to evaluate tissue stabilized-guided subcision using the cellfina device for the treatment of cellulite with 3-year follow-up. Dermatol Surg. 2017;43(10):1240-8.
13. Kent DE, Jacob CI. Simultaneous changes in abdominal adipose and muscle tissues following treatments by high-intensity focused electromagnetic (HIFEM) technology-based device: computed tomography evaluation. J Drugs Dermatol. 2019;18(11):1098-102.
14. Katz B, Bard R, Goldfarb R, Shiloh A, Kenolova D. Ultrasound assessment of subcutaneous abdominal fat thickness after treatments with a high-intensity focused electromagnetic field device: a multicenter study. Dermatol Surg. 2019;45(12):1542-8.
Doris Hexsel 0000-0002-0615-9026
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; critical literature review; critical revision of the manuscript.
Indira Valente-Bezerra 0000-0002-4350-9080
Statistical analysis; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; critical revision of the manuscript.
Andressa Renon 0000-0002-9187-3418
Author's Contribution: Data collection, analysis, and interpretation.
Vitor Costa Fabris 0000-0002-3540-2769
Author's Contribution: Statistical analysis; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; critical revision of the manuscript.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}