


Vivian de Carvalho Amaral
Financial support: None
Conflict of interest: None
How to cite this article: Amaral VC. PDO threads, calcium hydroxyapatite, and l-polylactic acid for vulvar flaccidity - indications, technique, and results. Surg Cosmet Dermatol. 2023;15:e20230192.
The labia majora become saggy with aging. Although filling with hyaluronic acid provides significant rejuvenation, it can also lead to the formation of true vulvar testicles if poorly indicated, especially in excessively flaccid vulvas, which do not support any further volumization. In these cases of excessive flaccidity, we believe that collagen biostimulators would be the best initial treatment, as their injection would lead to the replacement of dermal collagen and improvement in laxity, without a significant increase in volume. We have been using calcium hydroxyapatite, l-polylactic acid, and PDO threads since 2019, with good results.
Keywords: Vulva; Collagen; Genitalia, Female; Rejuvenation
The external female genitalia loses elasticity and volume with age,1,2 causing the labia majora (LM) to become flaccid and pendulous. Although volumetric replacement of the LM with hyaluronic acid (HA) can provide significant rejuvenation,1, 2, 3, 4 when poorly indicated, it can also form vulvar testicles.5 We believe that such aesthetic failure occurs due to large volumes of high molecular weight products or when the injection is poorly indicated and performed in excessively flaccid vulvas that cannot support additional volume.
In cases of excessive flaccidity, we believe that collagen biostimulators (CB) would be the best initial treatment, as their injection would lead to the replacement of dermal collagen, improving flaccidity without excessive increase in volume. For this purpose, since 2019, we have been using the injection of calcium hydroxyapatite (CaHA), l-polylactic acid (PLLA), and PDO threads (PDO), with good results.
Since 2019, we selected 21 women between 30 and 60 years with vulvar flaccidity and bulky and/or hanging labia majora (LM) for collagen biostimulators (CB) injection.
The choice of treatment was based on the criteria below:
- Bulky LM, which should not have received any additional volume, received PDO;
- LM that needed initial volumization, received CaHA;
- PLLA was the product of choice to treat the entire genital area, involving LM and mons pubis.
We inserted the three products into the superficial subcutaneous tissue.
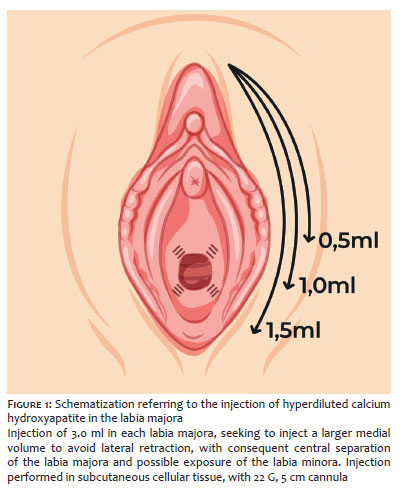
CaHA and PLLA injections were performed using the fan technique, by retroinjection, with a 22 G, 5 cm cannula.
We used a syringe with carboxymethylcellulose gel 70% and CaHA 30% for CaHA injection, diluted in the saline solution until reaching four times the initial volume of the syringe. Half the final volume obtained was injected into each LM (about 3.0 ml per side) (Figure 1).
We used 150 mg or 210 mg bottles for PLLA injections, initially diluted in 16 ml and 24 ml of distilled water, respectively, plus 4 ml of lidocaine1%. A PLLA concentration of 7.5 mg/ml was reached in both dilutions: 5 ml was injected in each LM and 10 ml in the mons pubis (Figure 2).
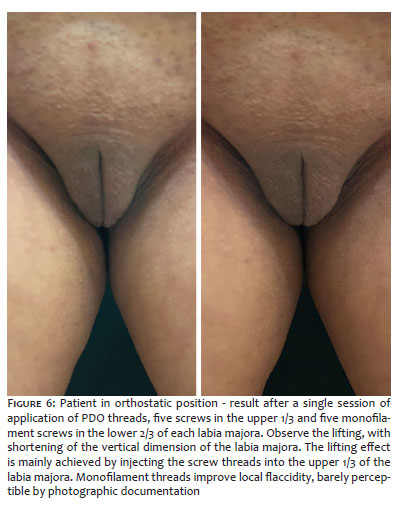
For PDO insertion, we used five threads on screws (29 G, 52 mm) in the upper 1/3 and five monofilament threads (30 G, 50 mm) in the lower 2/3 of each LM, totaling ten threads per side (Figure 3).
Patients who received PDO were only re-approached four months after the initial procedure, if necessary. In the case of CaHA or PLLA treatment, one to two sessions were performed, with a minimum interval of 30 days.
All treated patients were satisfied with their results after 90 days (Figures 4, 5, and 6). However, we observed greater initial satisfaction among patients who received CaHA.
As complications, we noted the formation of a palpable nodule, not visible, with CaHA, and an infection treated with oral antibiotic therapy with PDO, without the need to remove the threads. Patients injected with PLLA had no major complications. Intercurrences, such as small bruises, edema, and local discomfort, were common to all procedures and resolved spontaneously within seven days.
Collagen biostimulators (CBs) act by increasing the production of dermal collagen by fibroblasts.
Inserting PDO threads results in neocollagenesis, proportional to the number of threads injected,6 neovascularization, fat reduction, and higher tissue contracture.7 Based on this information, we followed the injection criteria:
• Due to the effect of fat compaction, we chose the most voluminous LM for PDO insertion;
• We never inject less than ten threads in each LM, for effective neocollagenesis;
• For a greater lifting effect, we used screw threads, which deliver a higher concentration of polydioxanone, with consequent higher tissue retraction in the upper 1/3;
• We did not use screw wires inferiorly, as they could bring about discreet volumization, which is undesirable in this location;
• We did not associate HA local injection before six months, under the risk of hydrophilic degradation of PDO.8
Hyperdiluted CaHA stimulates neocollagenesis with safety,9, 10, 11 efficacy, and long duration.12 Due to the presence of the carboxymethylcellulose gel vehicle, the treatment can be used as an adjuvant to volume increase.13 The most reported complications are nodules, which disappear without intervention in most cases.13 Its occurrence increases in areas of thinner skin and very superficial injections of less diluted CaHA.14 Based on this information, we follow the criteria for injecting CaHA:
• We opted for CaHA for LM that already needed some initial volumization, with intense skin flaccidity and prominent grooves in the area;
• We hyperdiluted the CaHA to 400% and kept the injection in the cutaneous portion of the LM, away from the mucosa, to avoid the formation of nodules;
• We vigorously massage the area after the injection and guide home massage for five minutes five times a day for five days;
• In general, only one session was performed, followed, after 60 days, by actual volumization with HA.
PLLA is considered a biocompatible and biodegradable polymer, effective, safe, with lasting effects and a high level of satisfaction among patients.15, 16, 17 PLLA injections induce the neoformation of type 1 and type 3 collagen, TGF-β1, TGF-β2, and TGF-β3, histologically perceptible as early as two weeks after injection and with a decrease in 12 weeks,18 but with clinically visible therapeutic effects for up to two years.19 The efficacy and safety of PLLA are influenced by the correct product reconstitution, dilution, and administration. Unwanted adverse events such as papules and nodules can result from incorrect product reconstitution, uneven distribution, superficial injection, or lack of post-treatment massage.20 Based on this information, we follow the criteria for PLLA injection:
• We followed the recommendation described in the medical literature for an injection of approximately 3mg/cm21, which allowed us to treat larger areas that included not only the LM but also the mons pubis;
• We avoided injecting patients with excessive volume in the mons pubis;
• We stopped the injection when 3/4 of the cannula was visible to avoid superficialization of the product and the appearance of papules and nodules 21;
• We performed the immediate reconstitution of the PLLA without major complications 22;
• We conducted, on average, two sessions with intervals of 30 days;
• We proceeded with the local massage as described for CaHA.
Although the use of collagen biostimulators (CBs) in non-genital areas is well established, the literature on such substances in vulvar rejuvenation is still scarce.23 However, the intense search for genital beautification procedures, associated with the good results obtained with the injection of CBs in other body areas has encouraged its use in the vulvar region.
We consider the treatments described to be safe and effective. The patients were instructed regarding the delayed effects of non-volumizing injections, which was crucial for achieving the expectations of the results. The most common adverse events of the three procedures were injection-related and included bruising, swelling, and mild discomfort. The encouraging results obtained should inspire further studies.
Vivian de Carvalho Amaral 0000-0002-5379-652X
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Zerbinati N, Haddad RG, Bader A, Rauso R, D'Este E, Cipolla G, et al. A new hyaluronic acid polymer in the augmentation and restoration of labia majora. J Biol Regul Homeost Agents. 2017;31(Suppl. 2):153-61.
2. 'Jabbour S, Kechichian E, Hersant B, Levan P, El Hachem L, Noel W, et al. Labia majora augmentation: a systematic review of the literature. Aesthet Surg J. 2017;37(10):1157-64.
3. Hexsel D, Dal Forno T, Caspary P, Hexsel CL. Soft-tissue augmentation with hyaluronic acid filler for labia majora and mons pubis. Dermatol Surg. 2016;42(7):911-4.
4. Fasola E, Gazzola R. Labia majora augmentation with hyaluronic acid filler: technique and results. Aesthet Surg J. 2016;36(10):1155-63.
5. Su C-F, Tsai H-J. Mimicking bilateral vulvar testicles after labia majora augmentation with hyaluronic acid. Ann Plast Reconstr Surg. 2019;3(5):1044.
6. Shin JJ, Park TJ, Kim BY, Kim CM, Suh DH, Lee SJ, et al. Comparative effects of various absorbable threads in a rat model. J Cosmet Laser Ther. 2019;21(3):158-62.
7. Yoon JH, Kim SS, Oh SM, Kim BC, Jung W. Tissue changes over time after polydioxanone thread insertion: an animal study with pigs. J Cosmet Dermatol. 2019;18(3):885-91.
8. Suárez-Vega DV, Velazco de Maldonado GJ, Ortíz RL, García-Guevara VJ, Miller-Kobisher B. In Vitro degradation of polydioxanone lifting threads in hyaluronic acid. J Cutan Aesthet Surg. 2019;12(2):145-8.
9. Fakih-Gomez N, Kadouch J. Combining calcium hydroxylapatite and hyaluronic acid fillers for aesthetic indications: efficacy of an innovative hybrid filler. Aesthetic Plast Surg. 2022;46(1):373-81.
10. Rovatti PP, Pellacani G, Guida S. Hyperdiluted calcium hydroxylapatite 1: 2 for mid and lower facial skin rejuvenation: efficacy and safety. Dermatol Surg. 2020;46(12):e112-e7.
11. Guida S, Longhitano S, Shaniko K, Galadari H, Chester J, Ciardo S, et al. Hyperdiluted calcium hydroxylapatite for skin laxity and cellulite of the skin above the knee: a pilot study. Dermatol Ther. 2020;33(6):e14076.
12. Wollina U, Goldman A. Long lasting facial rejuvenation by repeated placement of calcium hydroxylapatite in elderly women. Dermatol Ther. 2020;33(6):e14183.
13. Goldie K, Peeters W, Alghoul M, Butterwick K, Casabona G, Chao YYY, et al. Global consensus guidelines for the injection of diluted and hyperdiluted calcium hydroxylapatite for skin tightening. Dermatol Surg. 2018;44(Suppl 1):S32-S41.
14. Guida S, Longhitano S, Spadafora M, Lazzarotto A, Farnetani F, Zerbinati N, et al. Hyperdiluted calcium hydroxylapatite for the treatment of skin laxity of the neck. Dermatol Ther. 2021;34(5):e15090.
15. Jabbar A, Arruda S, Sadick N. Off face usage of Poly-L-Lactic acid for body rejuvenation. J Drugs Dermatol. 2017;16(5):489-94.
16. Ray S, Adelnia H, Ta HT. Collagen and the effect of poly-l-lactic acid based materials on its synthesis. Biomater Sci. 2021;9(17):5714-31.
17. Alessio R, Rzany B, Eve L, Grangier Y, Herranz P, Olivier-Masveyraud F, et al. European expert recommendations on the use of injectable poly-L-lactic acid for facial rejuvenation. J Drugs Dermatol. 2014;13(9):1057-66.
18. Kim CM, Kim BY, Hye Suh D, Lee SJ, Moon HR, Ryu HJ. The efficacy of powdered polydioxanone in terms of collagen production compared with poly-L-lactic acid in a murine model. J Cosmet Dermatol. 2019;18(6):1893-8.
19. Trinh LN, Gupta A. Non-hyaluronic acid fillers for midface augmentation: a systematic review. Facial Plast Surg. 2021;37(4):536-42.
20. Narins RS. Minimizing adverse events associated with poly-L-lactic acid injection. Dermatol Surg. 2008;34(Suppl 1):S100-4.
21. Haddad A, Bogdana VK, Guarnieri C, Noviello JS, Cunha MG, Parada MB. Conceitos atuais no uso do ácido poli-l-láctico para rejuvenescimento facial: revisão e aspectos práticos. Surg Cosmet Dermatol. 2017;9(1):61-71.
22. Bravo BSF, Carvalho RM. Safety in immediate reconstitution of poly-l-lactic acid for facial biostimulation treatment. J Cosmet Dermatol. 2021;20(5):1435-8.
23. Loghem. Use of calcium hydroxylapatite for augmentation of the labia majora and mons pubis. Sci J Clin Res Dermatol. 2017;2(1):10-3.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}