


Luana Amaral de Moura; Lucia Martins Diniz; Emilly Neves Souza; Alexandre Calegari Oliosi; Marcela Scárdua Sabbagh de-Azevedo
Financial support: None
Conflict of interest: None
How to cite this article: Moura LA, Diniz LM, Souza EN, Oliosi AC, Azevedo MSS. Eccrine syringofibroadenoma in a patient with quadriplegia following transverse myelitis. Surg Cosmet Dermatol. 2022;14:e20220164.
Eccrine syringofibroadenoma (EFAS) is a rare benign tumor that originates from the eccrine sweat glands. It has a predilection for the extremities of elderly individuals and may arise in association with various acquired or hereditary diseases and neoplastic skin disorders. We report the case of a 48-year-old man who had been quadriplegic due to transverse myelitis for 30 years, with a rapidly progressive plantar tumor that was difficult to diagnose.
Keywords: Poroma; Neoplasms; Eccrine glands.
Eccrine syringofibroadenoma (ESFA) is a rare benign adnexal tumor that originates from the acrosyringium portion of the eccrine sweat glands.1,2 It usually presents as a solitary hyperkeratotic nodular lesion, of variable size, with a predilection for the extremities of elderly individuals.3,4 We report a case of a 48-year-old man with a rapidly growing plantar tumor that was difficult to diagnose clinically and histopathologically.
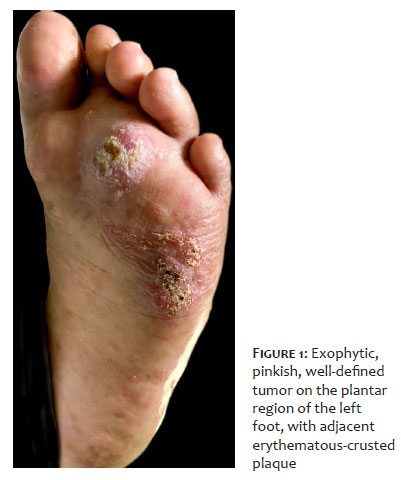
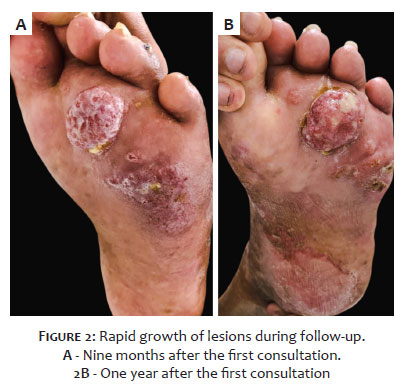
A 48-year-old man, quadriplegic for 30 years due to transverse myelitis and with a right nephrectomy, reported an erythematous macular lesion on the plantar region of the left foot, which had appeared four months ago and evolved into a tumor, in addition to unexplained weight loss and weakness. He denied trauma. On examination, he presented the Leser-Trélat sign, lower limbs edema, and an exophytic, pink, well-defined tumor on the plantar region of the left foot, with an adjacent erythematous-crusted plaque (Figure 1). The anatomopathological examination of the biopsy performed at another Service suggested spongiotic dermatitis. During follow-up, the patient evolved with the rapid growth of the lesions (Figure 2). Two new incisional biopsies were performed, whose histological analyzes were compatible with stasis dermatitis. Cultures were negative. Nuclear magnetic resonance showed a solid expansive formation measuring 3.2 x 1.2 x 3.0 cm, restricted to the cutaneous plane, nonspecific. After approximately one year, a new histopathological examination revealed infiltration of eosinophils and plasmocytes, chronic localized lymphedema, and an area of atypical lymphoid cells. Immunohistochemical analysis (Figure 3) was positive for p63 protein, EMA (epithelial membrane antigen), and CEA (carcinoembryonic antigen) in ducts, findings consistent with eccrine syringofibroadenoma. The patient is awaiting an exeresis of the lesion with the Plastic Surgery team. The investigation of occult neoplasms was negative until the time of submission of this report.
First described by Mascaró in 1963, ESFA is a benign adnexal proliferation of duct-forming epithelial cells with eccrine differentiation and a certain histological affinity with mammary fibroadenoma.5 It has a predilection for the extremities, can be single or multiple, and arise in association with various acquired or hereditary diseases and neoplastic skin conditions.1,5
The current classification encompasses five subtypes: (1) solitary; (2) multiple associated with ectodermal dysplasia; (3) multiples without skin findings (eccrine syringofibroadenomatosis); (4) unilateral linear (nevoid); and (5) reactive associated with inflammatory or neoplastic dermatoses, as in our report.4,5
Reactive ESFA appears to be secondary to a repair and remodeling process induced after tissue damage, leading to injury-reactive hyperplasia.3 Its association with multiple entities has been described, such as diabetes mellitus, lichen planus, squamous cell carcinoma, leprosy, and polyneuropathies.1 Considering the significant chronic lymphedema presented by the reported patient, we believe that the etiopathogenesis of ESFA is directly related to this situation.
Despite the diverse clinical presentations, the histopathological features comprise anastomosing cords of cuboidal epithelial cells surrounded by fibrovascular stroma with plasmocytes and ductal structures. Immunohistochemical analysis can help the diagnosis, with positivity for EMA and CEA, showing the lumen of the acrosyringium in the epithelial cords of the lesion.1,3,4
Treatment is controversial and may involve excision, radiotherapy, laser, etretinate, and topical corticosteroids.3,5
The present report emphasizes the importance of ESFA as a differential diagnosis of tumor lesions in the extremities and demonstrates a case of ESFA reactive to chronic lower extremity lymphedema in a quadriplegic patient.
Luana Amaral de Moura 0000-0002-3697-0186
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Lucia Martins Diniz 0000-0001-8107-8878
Approval of the final version of the manuscript; preparation and writing of the manuscript; active participation in research orientation; critical revision of the manuscript.
Emilly Neves Souza 0000-0003-1151-8537
Approval of the final version of the manuscript; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Alexandre Calegari Oliosi 0000-0001-6191-631X
Approval of the final version of the manuscript; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Marcela Scárdua Sabbagh de-Azevedo 0000-0002-1664-3217
Approval of the final version of the manuscript; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
1. Khan HA, Kumarasinghe P, Wood B. Late-onset eccrine syringofibroadenoma of the feet in a patient with hypohidrotic ectodermal dysplasia. Australas J Dermatol. 2021;62(3):383-5.
2. Tedbirt B, Carvalho P, Boulard C, Tetart F, Deschamps-Huvier A, Chenal P, et al. Reactive eccrine syringofibroadenomatosis associated with venous leg ulcers: a case report and literature review. Int J Low Extrem Wounds. 2020;20:1534734620966900.
3. Cunha Filho RRD, Quioca LJ, Rastelli GJC, Neto JF. Reactive eccrine syringofibroadenoma triggered by thermal damage: case report. An Bras Dermatol. 2021;96(2):255-6.
4. Temnithikul B, Jerasutus S, Sudtikoonaseth P, Voravutinon N, Kootiratrakarn T, Kattipathananpong P. Eccrine syringofibroadenoma (ESFA): a report of two cases. Dermatol Pract Concept. 2016;6(1):5-8.
5. Pagliuca F, Moscarella E, Argenziano G, Ronchi A, Franco R. Longstanding eccrine syringofibroadenoma with evidence of carcinomatous transformation. Am J Dermatopathol. 2020;42(10):780-2.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}