


Talira Caserta Gon1; Trícia Caserta Gon2; Airton dos Santos Gon3
Financial support: None
Conflict of interest: None
How to cite this article: Gon TC, Gon TC, Gon AS. Successful treatment of chromoblastomycosis using cryosurgery in association with low-dose itraconazole. Surg Cosmet Dermatol. 2023;15:e20220154.
Chromoblastomycosis is a chronic granulomatous infection caused by dematiaceous fungi with varied clinical presentations, which may represent a therapeutic challenge. In this report, we present a case of chromoblastomycosis in a localized form, with a long evolution, in an elderly patient, resistant to previous drug therapies, successfully treated by the association of a physical method with systemic pharmacological treatment, which allowed the use of a reduced dose of the drug.
Keywords: Chromoblastomycosis; Cryosurgery; Itraconazole
Chromoblastomycosis is a chronic granulomatous infection that affects the skin and subcutaneous tissue, caused by dematiaceous fungi (brown pigment-producing). In endemic areas, the prevalent species are Fonsecaea pedrosoi and Cladophialophora carrionii.1 The lesions appear as slow-growing verrucous plaques, with the possibility of atrophy or formation of nodules and tumors. It can be considered an occupational disease, frequently occurring in rural workers. Most lesions occur on exposed areas, as the fungus is usually inoculated by trauma.2,3
In many cases, chromoblastomycosis treatment still represents a challenge due to the chronic and recurrent nature of the lesions, whether in the localized or extensive forms of the disease. Several reports have demonstrated the usefulness of associating pharmacological treatments with physical procedures to obtain better results.1
We report the successful treatment of a case of long-standing chromoblastomycosis using cryosurgery and low-dose itraconazole.
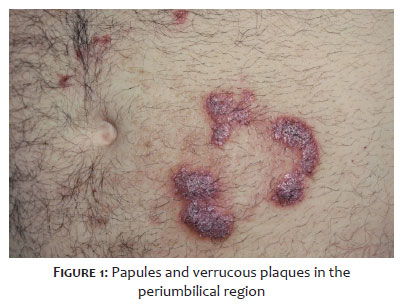
A 71-year-old man presented pruritic lesions on his abdomen for 20 years with no improvement after several treatment attempts with topical agents and systemic antifungals. When the lesions appeared, the patient lived and worked in a rural area, where he reported, as a routine activity, the habit of carrying firewood in contact with the abdomen without any protection. Upon dermatological examination, the patient presented papules and verrucous plaques, well delimited, in the periumbilical region, more to the left, in a corymbiform arrangement (Figure 1). Histopathological examination defined the diagnosis of chromoblastomycosis, showing a chronic granulomatous reaction and epithelial hyperplasia, with the presence of brownish refractive fungi. Tissue culture isolation obtained by biopsy of the fungus Fonsecaea pedrosoi confirmed the diagnosis. The patient underwent two cycles of application of liquid nitrogen in an open spray. Due to the extension, the lesions were divided by areas and treated sequentially until reaching freezing and halo formation (60 seconds). The second cycle was performed after the complete thawing of the lesions (10 minutes). Itraconazole, at a dose of 100 mg per day orally, was prescribed for continuous use until return. After 45 days, the patient showed significant improvement and partial regression of the lesions (Figure 2). He underwent a second cryosurgery session, and itraconazole was maintained at the same dosage. At 90 days, he presented complete regression of the lesions, and treatment was suspended (Figure 3). Follow-up was conducted for five years, with no recurrence of the condition (Figure 4).
Patients with long-standing chromoblastomycosis, both in localized and extensive forms, require prolonged treatment with high-dose systemic antifungals, sometimes associated with physical methods.4
In a recent systematic review on the in vitro action of oral antifungal drugs available for chromoblastomycosis treatment, based on the minimum inhibitory concentration, the most effective drugs were, in descending order, posaconazole, terbinafine, itraconazole, and voriconazole.5 However, in clinical practice, itraconazole can be considered the standard drug among the antifungals used. Its use has been recognized for a long time through reports of clinical and biological cures in about 40% of patients when applied for prolonged periods at dosages ranging from 200 mg to 400 mg per day.6 During treatment with itraconazole, more significant tissue responses were recorded in the dermis, observing a reduction in the thickness of the epidermis, a partial or total decrease in the granulomatous infiltrate, an increase in fibrosis, and quantitative/morphological alterations.7
Cryosurgery with liquid nitrogen has been described as an effective method to treat chromoblastomycosis for several decades.8-10 Although it is accepted as an effective treatment modality, the mechanism that leads to the cure of the disease is still unknown. Exposure of cultures of the causative microorganisms to temperatures as low as -196°C did not cause the agents to die.11 These results demonstrate that cold alone cannot be responsible for their destruction. It is believed that late biological phenomena, such as necrosis with tissue destruction and alterations in the host’s immune response, are responsible for eradicating fungi in the lesions.12,13
A strategy to increase cure rates and reduce recurrences is the association between different drugs, such as itraconazole and terbinafine, and combining physical methods with oral antifungals. Among these, the association between an oral antifungal and cryosurgery with liquid nitrogen has been one of the most described methods.14-16 However, oral antifungals, in high doses and for prolonged periods, have their use limited by the high cost and the risks of major adverse events.
In this patient, performing surgery to remove the lesions was considered impractical due to the location and extent of the lesions. Because of the size of the resulting surgical defect, primary closure by approximation of the edges was unlikely, which would imply the need to use more complex techniques such as grafts or flaps. Another aspect considered, in the case of an elderly patient, was to avoid using drugs with potential adverse events in high doses and for a prolonged period.
Thus, the therapeutic approach adopted was to combine cryosurgery with liquid nitrogen, in a non-aggressive way, with oral antifungal, in a lower dosage than that recommended in the literature. This strategy proved to be effective, reducing costs and potential adverse events, providing clinical cures, and, consequently, a better quality of life for the patient.
Talira Caserta Gon 0000-0002-1567-680X
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Trícia Caserta Gon 0000-0003-4169-1840
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Airton dos Santos Gon 0000-0003-1219-5581
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Brito AC, Bittencourt MJS. Chromoblastomycosis: an etiological, epidemiological, clinical, diagnostic, and treatment update. An Bras Dermatol. 2018;93(4):495-506.
2. Kurien G, Sugumar K, Chandran V. Chromoblastomycosis. [Updated 2022 Feb 6]. In: StatPearls [Internet]. Treasure Island (FL) [Cited 2022 Jan.]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470253/
3. Correia RTM, Valente NYS, Criado PR, Martins JEC. Cromoblastomicose: relato de 27 casos e revisão da literatura. An Bras Dermatol. 2010;85(4):448-54.
4. Queiroz-Telles F. Chromoblastomycosis: a neglected tropical disease. Rev Inst Med Trop. 2015;57(suppl 19):46-50.
5. Hellwig AHS, Heidrich D, Zanette RA, Scroferneker ML. In vitro susceptibility of chromoblastomycosis agents to antifungal drugs: a systematic review. J Glob Antimicrob Resist. 2019;16:108-14.
6. Queiroz-Telles F, Purim KF, Fillus JN, Bordignon GF, Lameira RP, Van Cutsem J, et al. Itraconazole in the treatment of chromoblastomycosis due to Fonsecaea pedrosoi. Int J Dermatol. 1992;31(11):805-12.
7. Purim KSM, Peretti MC, Fillus JN, Olandoski M. Chromoblastomycosis: tissue modifications during itraconazole treatment. An Bras Dermatol. 2017;92(4):478-83.
8. Sittart JAS, Valente NY. Tratamento da cromomicose pelo nitrogênio liquido [Treatment of chromomycosis with liquid nitrogen]. Med Cutan Ibero Lat Am. 1986;14(4):227-32.
9. Pimentel ER, Castro LG, Cucé LC, Sampaio SA. Treatment of chromomycosis by cryosurgery with liquid nitrogen: a report on eleven cases. J Dermatol Surg Oncol. 1989;15(1):72-7.
10. Castro LG, Pimentel ER, Lacaz CS. Treatment of chromomycosis by cryosurgery with liquid nitrogen: 15 years' experience. Int J Dermatol. 2003;42(5):408-12.
11. Castro LGM. Mecanismo de cura da cromomicose pela criocirurgia com nitrogênio líquido: estudos in vitro sobre a resistência dos fungos causadores da doença ao frio. An Bras Dermatol. 1989;64(6):297-300.
12. Castro LGM, Salebian A, Lacaz CS. Células fúngicas permanecem viáveis por até doze dias em lesões de cromomicose tratadas pela criocirurgia com nitrogênio líquido. An Bras Dermatol. 2003;78(3):279-82.
13. Moraes AM, Velho PENF, Magalhães RF. Criocirurgia com nitrogênio líquido e as dermatoses infecciosas. An Bras Dermatol. 2008;83(4):285-98.
14. Elkhachine Y, Elbenaye J, Er-Rami M, Sakkah A, Jakar A, Elhaouri M. Chromomycose cutanée étendue: efficacité de l’association terbinafine et cryothérapie [Extensive cutaneous chromomycosis: Efficacy of combined terbinafine and cryotherapy]. Ann Dermatol Venereol. 2018;145(8-9):512-5.
15. Kullavanijaya P, Rojanavanich V. Successful treatment of chromoblastomycosis due to Fonsecaea pedrosoi by the combination of itraconazole and cryotherapy. Int J Dermatol. 1995;34(11):804-7.
16. Ranawaka RR, Amarasinghe N, Hewage D. Chromoblastomycosis: combined treatment with pulsed itraconazole therapy and liquid nitrogen cryotherapy. Int J Dermatol. 200;48(4):397-400.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}