


Balduino Ferreira de Menezes Neto1; Lucas Vannuchi Magnani1; Aristides Augusto Palhares Neto1; Natália Parenti Bicudo2; Batista de Oliveira Júnior3
Financial support: None
Conflict of interest: None
How to cite this article: Menezes Neto BF, Magnani LV, Palhares Neto AA, Bicudo NP, Oliveira Júnior B. Alternatives for keloid scars treatment: an integrative review. Surg Cosmet Dermatol. 2022;14:e20220127.
Keloid scars affect different populations, compromising patients’ quality of life. The literature presents several treatments. The study aimed to conduct an integrative review of systematic review articles and/or meta-analyses addressing keloid treatment in the PubMed, LILACS, MEDLINE, and Cochrane databases from 2015 to 2021. After identification and following the selection and eligibility criteria, 24 articles were included for qualitative review. We observed that the difficulty in evaluating recurrence affected different keloids treatment modalities, still presenting many failure rates and the need for further studies.
Keywords: Keloid; Scar, hypertrophic; Scar; Clinical procedures; Review; Systematic reviews as topic.
Keloids, named by Alibert in 1806,1 were described as a growth similar to the projections of twigs or crab claws. The English word keloid derives from the Greek khele.
The main characteristics of this benign tumor are its prolonged course of activity, its ability to surpass the limits of the initial lesion, multiple specific genetic and cellular factors (many of them not yet fully elucidated), and unique pathophysiology.2 At the histological level, there is a chronic inflammation of the reticular dermis, with high number of fibroblasts and collagen, especially type I, eosinophilic and hyalinized.
According to the current literature, there is lower growth and development of these tumors after menopause, being more common during pregnancy and puberty.3 Also, genetics, ethnicity, and initial lesion site have been described as factors that favor the appearance of keloids.4
The literature describes several treatment techniques, which can be invasive or non-invasive. Among them, we can highlight alternatives such as compression therapy, silicone gel sheets, and onion extract.5
Pressure therapy for patients with closed wounds that tolerate pressure should be used for at least 23 hours a day, for six to 24 months, using pressure between 24 mmHg and 30 mmHg.5,6 Although it shows good results, this treatment generates high costs, in addition to causing significant discomfort to patients.7
Silicone materials have been indicated as one of the main non-invasive methods, with reported improvement rates of 90%.8 These materials are available as gels or sheets. Silicone sheets should be used from 12 to 24 hours a day, for three to six months, while silicone gels should be applied twice daily.5 However, the literature lacks large studies that prove its effectiveness, in addition to the fact that these materials hardly reach the full resolution of scars.9
Treatment with onion extract, whose main component is quercetin – which has collagen-suppressing, antimicrobial, and anti-inflammatory properties – can also be used to reduce excess scarring.5 Nevertheless, it also lacks prospective and randomized studies.
Regarding treatment, several studies attempt to prove the importance of the association of therapies but with no statistically definitive results.10 However, it’s noteworthy that simple surgical excision, with no adjuvant method, has high recurrence rates, close to 50%, which increases after new attempts, especially in the first four years.11
Although it remains an incurable condition, there are several types of treatments. The most classic is intralesional infiltration of drugs, such as 5-fluorouracil and corticosteroids, and several modalities of adjuvant radiotherapy (RT), such as conventional RT, electron beam RT, and single-dose RT.12
The primary mechanism of action of radiotherapy involves the inhibition of histamine release by mast cells, resulting in a decrease in fibroblast proliferation, in addition to the inhibition of TGF-Beta1, which suppresses collagen production, interfering with the formation of keloids.13
In the 1960s, studies showed that external radiation therapy failed to resolve the lesion when performed alone. Nevertheless, positive results in symptoms alleviation were obtained when the treatment was associated with surgical excision, with worse outcomes in cases of delay in performing radiotherapy after excision, generating higher recurrence rates.14
However, the risk of carcinogenesis associated with adjuvant radiotherapy was still a significant concern. A literature review conducted in 2009 described five cases of this occurrence, although it was not possible to state whether adequate adjacent tissues protection and correct doses were used.15 Thus, the study concluded that the risk of carcinogenesis should not be an impediment to performing the procedure and is essential to emphasize the importance of preventive measures, such as care for the surrounding tissues and protection of the thyroid and mammary glands, especially in children and adolescents.15
A few years later, brachytherapy was developed, which performs internal or interstitial radiotherapy, further reducing these risks.16 With the ability to emit more efficient and focused radiation on the lesion, this technique also requires a lower dose, resulting in reduced local radionecrosis and adverse events on adjacent healthy tissues. Nonetheless, this procedure demands higher hospital expenses due to the use of poorly available and specific materials, in addition to prolonged hospitalizations.15
Electron beam therapy has been widely used in several medical centers, considerably replacing other radiotherapy methods in the keloid treatment.17 A research conducted at the Clinics Hospital of the Medical School of Botucatu (FMB-UNESP) in São Paulo (BR) highlighted its importance. Therefore, this treatment option was maintained in the current routine when approaching these lesions.18,19
Furthermore, the search for new treatments continues20 and comprises the use of angiotensin-converting enzyme (ACE) inhibitors;21,22 intralesional injections of calcium antagonists (such as verapamil);23 intralesional injections of botulinum toxin type A;24,25 electrical stimulation;26 lasers; and cryotherapy,27 among others.
This study aims to present an integrative literature review using only systematic reviews published in the main medical databases in the last five years to understand which treatments have been most applied and developed nowadays.
To conduct an integrative literature review, we used the following electronic databases: PubMed, LILACS, MEDLINE, and Cochrane.
The search period was from 05/10/2021 to 05/23/2021, and we selected only articles published between January 2015 and May 2021.
Search terms and keywords
Databases were searched using the following keywords: “keloid” “and” “treatment”.
Languages were restricted to English and Portuguese, and the search format was adapted to the appropriate syntax of each database.
We selected only systematic reviews and meta-analyses comprising the clinical management of pathological scars, focusing on keloids. Non-human studies and reviews focusing on other pathologies, such as burns and acne, were excluded.
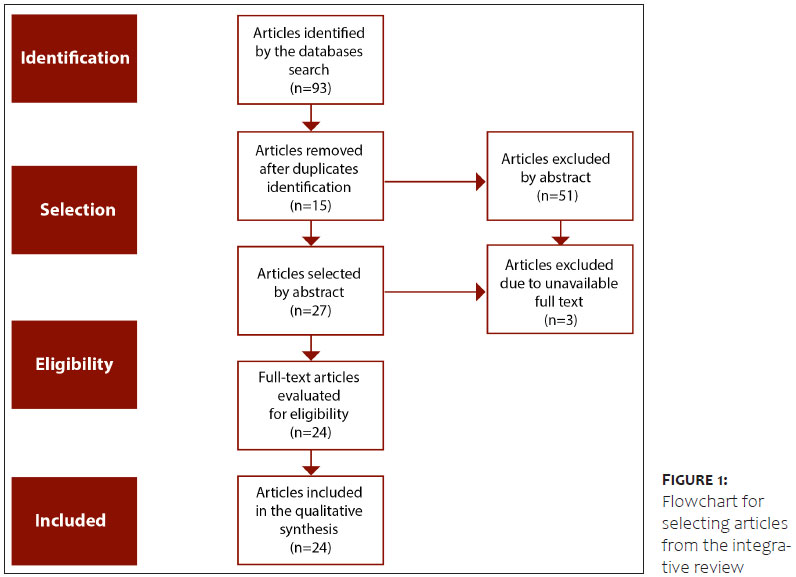
According to the flowchart below (Figure 1) and the Methods section proposal, we searched articles in English and Portuguese between 05/10/2021 and 05/23/2021, using the descriptors “keloid and treatment”, “keloid treatment”, “queloide e tratamento”, focusing only on systematic reviews and/or meta-analyses.
We selected four databases recognized for their visibility, information quality, and access: PubMed, LILACS, MEDLINE, and Cochrane.
In the PubMed database, we used the descriptor “keloid treatment” and filters: results by year from 2015 to 2021 and article type for systematic review and/or meta-analysis. In this initial search, we identified 46 articles. Of them, 26 were excluded: 22 did not focus on keloids, one was not in English, and three articles did not have full text available.
In the MEDLINE database, we found 20 references using the descriptors “keloid treatment systematic review and/or meta-analysis”. Of them, seven articles were excluded because their abstract was incompatible with the keloid treatment topic or because they were not in English or Portuguese. The remaining 13 articles had already been identified in the PubMed database and were excluded due to duplicates.
In the LILACS database, 25 articles were found and only four were kept because the others did not focus on pathological scars, were published before 2015, or were not in Portuguese or English.
The two articles found in the Cochrane database were excluded due to duplicates, as they were already retrieved from the PubMed database.
In the end, 24 systematic reviews and/or meta-analysis articles were selected: four in Portuguese and 20 in English. Two independent researchers (BFMN and AAPN) read all articles in full and divided the different treatment proposals into clinical, surgical, and radiotherapy treatments. The protocol was formulated after a discussion among the two researchers, an independent researcher from Dermatology (JVS) and another independent researcher from Radiotherapy (BOJ).
Among the selected articles, six addressed keloid treatments, four assessed the use of 5-fluorouracil associated or not with corticosteroids, three evaluated radiation therapies, and three analyzed laser technologies. Two investigated the use of verapamil, and two of bleomycin. One review article assessed fat grafting, one analyzed botulinum toxin type A, one investigated imiquimod, and one evaluated corticosteroids alone.
The four articles in Portuguese were not included as systematic reviews but were maintained as they served as references for alternative medications in the discussion of protocol formation.
The literature reports several methods to treat and prevent keloid scars. Because the effective and definitive treatment of this pathological scar is a great challenge, new therapeutic modalities are constantly emerging, in addition to combinations of treatments already used.
First, it is critical to emphasize that this benign tumor treatment begins with prevention. Intraoperative care is essential for all surgical procedures. However, in patients with a predisposition to keloid formation, these precautions are critical. Among them, we can mention the careful manipulation of the tissues, respect for the dissection planes when performing the synthesis, and the preferential use of absorbable sutures in the subcutaneous tissue and fascia,28 thus reducing the tension on the suture lines as much as possible.
Compression therapies affect collagen degradation and fibroblast activity,29 and are especially helpful in ears, as they have their pressure molds, which should not exceed 24 mmHg and 12 hours a day use.30 Silicone plates and tapes also act on collagen and fibroblasts. However, in theory, they use their ability to generate a more hydrated environment for the wound.31 Thus, this group of therapies is only complementary and should not be used alone.
The administration of intralesional corticosteroids is considered one of the most efficient and accessible methods to treat keloids.32 As it is the first line in most services, this therapy suppresses fibroblasts and inflammatory mediators of wounds, generating collagen degradation.33
Triamcinolone acetate (TAC) in concentrations between 5 mg/mL and 40 mg/mL is the main form used, promoting the reduction of keloid volume and showing variable rates of recurrence prevention.34 Skin atrophy, pain during injection, telangiectasias, and skin pigmentation changes are among its main adverse events.35
Intralesional and topical 5-fluorouracil (5-FU) is a pyrimidine antimetabolite that interferes with RNA synthesis and inhibits the thymidylate synthase, thus inhibiting fibroblasts.36 Therefore, the combination of 5-FU+TAC is safer and more effective than these drugs alone.37
Botulinum toxin (BT) type A inhibits the acetylcholine release in motor neurons by antagonizing the ionic calcium action, generating temporary muscle paralysis.38 Nevertheless, there are indications that, in pathological scars, it acts directly on the activity of fibroblasts.39
Topical imiquimod 5% cream can alter the immune response by inducing the release of IFN-alpha, TNF-alpha, and interleukins 1, 6, and 8.40 It presents keloid recurrence in 39% of the cases when associated with surgical excision in applications from six to eight weeks, daily or every three days.41 However, some studies evaluated by this review included patients who only performed tangential excision or shaving, using closure by secondary intention, and not by layers.42 This drug requires a minimum of one-week rest, especially between the second and third weeks of application, as erosion, erythema, and crust formation are frequent in 18% to 89% of patients. Therefore, topical imiquimod cream is an exceptional measure because it is unreliable.
Verapamil, a calcium channel blocker, can be applied intralesionally in doses of 2.5 mg/mL, not exceeding 2 mL per session. Sessions occur at three-week intervals and should be interrupted after the eighth procedure or when the lesion has flattened.43 Although it is less effective than the 5-FU+TAC combination, its use has good clinical safety, generating fewer adverse events.44 This drug increases the procollagenase synthesis, reducing the extracellular matrix production and inhibiting the fibroblast proliferation and the interleukin 6, TGF-Beta,1 and VEGF expression in fibroblasts.45
Pentoxifylline is a drug derived from xanthine, a nonspecific phosphodiesterase inhibitor, which has a vasodilating effect.46
It presents significant rates of recurrence prevention of keloids in patients at high risk when administered orally, in 400 mg doses, three times a day for six months after surgical excision. Furthermore, this drug can be used intralesionally. However, few studies have addressed this possibility.47
Hyaluronidase and hyaluronic acid, drugs with antagonist actions, have been reported to treat keloids intralesionally.48 Nonetheless, both drugs were used in association with corticosteroids, making it difficult to establish the real effects on pathological scars, thus requiring more research aimed at understanding its results on keloids.
Bleomycin can reduce collagen synthesis by decreasing the stimulation of TGF-Beta1.49 Compared to TAC, it was more likely to generate pain, hyperpigmentation, and skin atrophy.50 According to a systematic review, bleomycin seems to be as effective as TAC and its combination with 5-FU.50 This study also observed that this drug produced more pain than the others during applications.
Intralesional cryotherapy with a needle achieved a reduction of up to 51% in the volume of the pathological scar.51
Currently, several treatments use laser due to the significant technological development that allowed the generation of different types of wavelengths. These treatments can be divided into non-ablative and ablative forms and vary between fractional and non-fractional configurations. Ablative forms, such as Er:YAG (waves of 2,940 nm) and CO2 laser (waves of 10,600 nm), are characterized by a longer recovery time and a considerable number of complications. Moreover, the non-ablative options, such as Nd:YAG (waves of 1,054 nm) and pulsed dye-laser (waves between 585 nm and 595 nm), eliminate some of these problems. The fractional lasers can generate microthermal zones, creating unaffected interspersed areas where tissue regenerates.52,53
The pulsed-dye laser has similar effects to those generated by TAC, but its studies presented a short follow-up, in addition to the lack of randomized and multicentric studies.53,54
The most modern and current drugs have the advantage to be applied in a laser-assisted manner, a method known as laser-assisted drug delivery (LADD).55 Researchers are also trying to use this method to treat keloids,56 which is possible since ablative lasers create microscopic spaces that allow drug penetration, such as BT and TAC. However, research still has low evidence, with few participants and a short follow-up period.
Radiation therapy allows the reduction of fibroblast action in keloids in a dose-dependent manner.57 Currently, after the great scientific evolution of the 20th century, it presents in two main forms: external and internal. The electron beam and X-ray are the most common ways of external application, while the most studied internal option is brachytherapy. Although some studies show the superiority of brachytherapy in preventing the recurrence of keloids,58 several meta-analyses have not confirmed this result in a statistically significant way.10
When surgical excision is associated with early radiotherapy, superior results are found.59
Adverse signs and symptoms of corticosteroids are similar to those of radiotherapies, such as desquamation, depigmentation, and erythema. Pain complaints are infrequent.15
The keloid scars treatment continues to be challenging: in addition to the peculiarities imposed by each patient, which vary according to their ethnicity, location, and size of the lesions, there is also the fact that studies can’t present long and consistent follow-ups to assess the emergence relapses.
New prospective studies and knowledge about this pathology and the effects of medications need to be conducted to achieve lasting results with quality for patients.
Balduino Ferreira de Menezes Neto 0000-0001-9379-4441
Study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Lucas Vannuchi Magnani 0000-0002-3176-9205
Preparation and writing of the manuscript; critical revision of the manuscript.
Aristides Augusto Palhares Neto 0000-0002-3484-862X
Approval of the final version of the manuscript; critical literature review; critical revision of the manuscript.
Natália Parenti Bicudo 0000-0001-8674-0349
Critical revision of the manuscript.
Batista de Oliveira Júnior 0000-0003-4768-1686
Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Addison T. On the keloid of Alibert, and on true keloid. Med Chir Trans. 1854;37:27-47.
2. Glass DA. Current understanding of the genetic causes of keloid formation. J Investig Dermatol Symp Proc. 2017;18(2):S50-3.
3. Wolfram D, Tzankov A, Pülzl P, Piza-Katzer H. Hypertrophic scars and keloids--a review of their pathophysiology, risk factors, and therapeutic management. Dermatol Surg. 2009;35(2):171-81.
4. Son D, Harijan A. Overview of surgical scar prevention and management. J Korean Med Sci. 2014;29(6):751-7.
5. Kim SW. Management of keloid scars: noninvasive and invasive treatments. Arch Plast Surg. 2021;48(2):149-157.
6. Gold MH, Berman B, Clementoni MT, Gauglitz GG, Nahai F, Murcia C. Updated international clinical recommendations on scar management: part 1--evaluating the evidence. Dermatol Surg. 2014;40(8):817-24.
7. Anzarut A, Olson J, Singh P, Rowe BH, Tredget EE. The effectiveness of pressure garment therapy for the prevention of abnormal scarring after burn injury: a meta-analysis. J Plast Reconstr Aesthet Surg. 2009;62(1):77-84.
8. Mustoe TA, Cooter RD, Gold MH, Hobbs FD, Ramelet AA, Shakespeare PG, et al; International advisory panel on scar management. International clinical recommendations on scar management. Plast Reconstr Surg. 2002;110(2):560-71.
9. Butler PD, Longaker MT, Yang GP. Current progress in keloid research and treatment. J Am Coll Surg. 2008;206(4):731-41.
10. Shin JY, Lee JW, Roh SG, Lee NH, Yang KM. A comparison of the effectiveness of triamcinolone and radiation therapy for ear keloids after surgical excision: a systematic review and meta-analysis. Plast Reconstr Surg. 2016;137(6):1718-25.
11. Ogawa R. The most current algorithms for the treatment and prevention of hypertrophic scars and keloids. Plast Reconstr Surg. 2010;125(2):557-68.
12. Kim JH, Koo JM, Park TH. Optimizing radiotherapy for keloids: a meta-analysis systematic review comparing recurrence rates between different radiation modalities. Ann Plast Surg. 2018;80(1):91-2.
13. Lee SY, Park J. Postoperative electron beam radiotherapy for keloids: treatment outcome and factors associated with occurrence and recurrence. Ann Dermatol. 2015;27(1):53-8.
14. Van den Brenk HA, Minty CC. Radiation in the management of keloids and hypertrophic scars. Br J Surg. 1960;47:595-605.
15. Ogawa R, Yoshitatsu S, Yoshida K, Miyashita T. Is radiation therapy for keloids acceptable? The risk of radiation-induced carcinogenesis. Plast Reconstr Surg. 2009;124(4):1196-1201.
16. Nicoletis C, Chassagne D. L'irradiation interstitielle par l'iridium 192 dans la prévention des récidives après excision chirurgicale des cicatrices chéloïdiennes [Interstitial irradiation by iridium 192 in the prevention of recurrence after surgical excision of keloid cicatrices]. Ann Chir Plast. 1967;12(3):237-42.
17. Maarouf M, Schleicher U, Schmachtenberg A, Ammon J. Radiotherapy in the management of keloids. Clinical experience with electron beam irradiation and comparison with X-ray therapy. Strahlenther Onkol. 2002;178(6):330-5.
18. Júnior B, Lastória J, Pereira H, Silveira L, Oliveira L, Stolf H. Estudo comparativo entre o tratamento radioterápico com elétrons e betaterapia, após cirurgia de queloides. Surg Cosmet Dermatol. 2009;1(2):53-7.
19. Oliveira Junior B, Schellini SA, Lastória JC, Carvalho LR, Stolf HO, Oliveira ALP. Tratamento de queloides usando radioterapia pósoperatória com elétrons: estudo comparativo e randomizado com dois esquemas. Surg Cosmet Dermatol. 2013;5(1):16–26.
20. Memariani H, Memariani M, Moravvej H, Shahidi-Dadras M. Emerging and novel therapies for keloids: a compendious review. Sultan Qaboos Univ Med J. 2021;21(1):e22-e33.
21. Ogawa R, Arima J, Ono S, Hyakusoku H. Case report total management of a severe case of systemic keloids associated with high blood pressure (Hypertension): clinical symptoms of keloids may be aggravated by hypertension. Eplasty. 2013;13:e25.
22. Iannello S, Milazzo P, Bordonaro F, Belfiore F. Low-dose enalapril in the treatment of surgical cutaneous hypertrophic scar and keloid--two case reports and literature review. Med Gen Med. 2006;8(4):60.
23. Margaret Shanthi FX, Ernest K, Dhanraj P. Comparison of intralesional verapamil with intralesional triamcinolone in the treatment of hypertrophic scars and keloids. Indian J Dermatol Venereol Leprol. 2008;74(4):343-8.
24. Zhibo X, Miaobo Z. Intralesional botulinum toxin type A injection as a new treatment measure for keloids. Plast Reconstr Surg. 2009;124(5):275e-7e.
25. Shaarawy E, Hegazy RA, Abdel Hay RM. Intralesional botulinum toxin type A equally effective and better tolerated than intralesional steroid in the treatment of keloids: a randomized controlled trial. J Cosmet Dermatol. 2015;14(2):161-6.
26. Ud-Din S, Bayat A. Electrical stimulation and cutaneous wound healing: a review of clinical evidence. Healthcare (Basel). 2014;2(4):445-67.
27. Oliveira GV, Metsavaht LD, Kadunc BV, Jedwab SKK, Bressan MS, Stolf HO, et al. Treatment of keloids and hypertrophic scars. Position statement of the Brazilian expert group GREMCIQ. J Eur Acad Dermatol Venereol. 2021;35(11):2128-42.
28. Corrêa PM, Passos CEF, Souza EM, Batista GAS, Jacintho JDO, Oliveira LB, et al. Treatment of keloids: a literature review. Rev Bras Cir Plást (RBCP). 2019;34(3):391–8.
29. Berman B, Maderal A, Raphael B. Keloids and hypertrophic scars: pathophysiology, classification, and treatment. Dermatol Surg. 2017;43(Suppl 1):S3-S18.
30. Chrisostomidis C, Konofaos P, Chrisostomidis G, Vasilopoulou A, Dimitroulis D, Frangoulis M, et al. Management of external ear keloids using form-pressure therapy. Clin Exp Dermatol. 2008;33(3):273-5.
31. Suetake T, Sasai S, Zhen YX, Ohi T, Tagami H. Functional analyses of the stratum corneum in scars. Sequential studies after injury and comparison among keloids, hypertrophic scars, and atrophic scars. Arch Dermatol. 1996;132(12):1453-8.
32. Betarbet U, Blalock TW. Keloids: a review of etiology, prevention, and treatment. J Clin Aesthet Dermatol. 2020;13(2):33-43.
33. Epstein E. Triamcinolone and keloids. West J Med. 1980;133(3):257-8.
34. Wong TS, Li JZ, Chen S, Chan JY, Gao W. The efficacy of triamcinolone acetonide in keloid treatment: a systematic review and meta-analysis. Front Med (Lausanne). 2016;3:71.
35. Heppt MV, Breuninger H, Reinholz M, Feller-Heppt G, Ruzicka T, Gauglitz GG. Current strategies in the treatment of scars and keloids. Facial Plast Surg. 2015;31(4):386-95.
36. Wang XQ, Liu YK, Qing C, Lu SL. A review of the effectiveness of antimitotic drug injections for hypertrophic scars and keloids. Ann Plast Surg. 2009;63(6):688-92.
37. Jiang ZY, Liao XC, Liu MZ, Fu ZH, Min DH, Yu XT, et al. Efficacy and safety of intralesional triamcinolone versus combination of triamcinolone with 5-Fluorouracil in the treatment of keloids and hypertrophic scars: a systematic review and meta-analysis. Aesthetic Plast Surg. 2020;44(5):1859-68.
38. Fanous A, Bezdjian A, Caglar D, Mlynarek A, Fanous N, Lenhart SF, et al. Treatment of keloid scars with botulinum toxin type A versus triamcinolone in an athymic nude mouse model. Plast Reconstr Surg. 2019;143(3):760-7.
39. Jagdeo J, Carruthers A, Smith KC. New frontiers and clinical applications for botulinum neuromodulators. Dermatol Surg. 2015;41(Suppl 1):S17-8.
40. Berman B. Imiquimod: a new immune response modifier for the treatment of external genital warts and other diseases in dermatology. Int J Dermatol. 2002;41(Suppl 1):7-11.
41. Klotz T, Munn Z, Aromataris EC, Greenwood JE. Imiquimod to prevent keloid recurrence postexcision: a systematic review and meta-analysis. Wound Repair Regen. 2020;28(1):145-56.
42. Berman B, Harrison-Balestra C, Perez OA, Viera M, Villa A, Zell D, et al. Treatment of keloid scars post-shave excision with imiquimod 5% cream: a prospective, double-blind, placebo-controlled pilot study. J Drugs Dermatol. 2009;8(5):455-8.
43. Aggarwal A, Ravikumar BC, Vinay KN, Raghukumar S, Yashovardhana DP. A comparative study of various modalities in the treatment of keloids. Int J Dermatol. 2018;57(10):1192-1200.
44. Li Z, Jin Z. Comparative effect and safety of verapamil in keloid and hypertrophic scar treatment: a meta-analysis. Ther Clin Risk Manag. 2016;12:1635-41.
45. Boggio RF, Freitas VM, Cassiola FM, Urabayashi M, Machado-Santelli GM. Effect of a calcium-channel blocker (verapamil) on the morphology, cytoskeleton and collagenase activity of human skin fibroblasts. Burns. 2011;37(4):616-25.
46. Tan A, Martinez Luna O, Glass DA. Pentoxifylline for the prevention of postsurgical keloid recurrence. Dermatol Surg. 2020;46(10):1353-6.
47. Serag-Eldin YMA, Mahmoud WH, Gamea MM, Hegab DS. Intralesional pentoxifylline, triamcinolone acetonide, and their combination for treatment of keloid scars. J Cosmet Dermatol. 2021;20(10):3330-40.
48. Limmer EE, Glass DA. A review of current keloid management: mainstay monotherapies and emerging approaches. Dermatol Ther (Heidelb). 2020;10(5):931-48.
49. Arno AI, Gauglitz GG, Barret JP, Jeschke MG. Up-to-date approach to manage keloids and hypertrophic scars: a useful guide. Burns. 2014;40(7):1255-66.
50. Kim WI, Kim S, Cho SW, Cho MK. The efficacy of bleomycin for treating keloid and hypertrophic scar: a systematic review and meta-analysis. J Cosmet Dermatol. 2020;19(12):3357-66.
51. Zouboulis VA, Zouboulis CC. A novel experimental model for studying efficacy of cryosurgery in keloids. J Eur Acad Dermatol Venereol. 2020;34(8):1851-4.
52. Walsh J, Morelli J, Parrish JA. Laser-tissue interactions and their clinical applications. Curr Probl Dermatol. 1986;15:94-110.
53. Forbat E, Ali FR, Al-Niaimi F. Treatment of keloid scars using light-, laser- and energy-based devices: a contemporary review of the literature. Lasers Med Sci. 2017;32(9):2145-54.
54. Park JH, Chun JY, Lee JH. Laser-assisted topical corticosteroid delivery for the treatment of keloids. Lasers Med Sci. 2017;32(3):601-8.
55. Zaleski-Larsen LA, Fabi SG. Laser-assisted drug delivery. Dermatol Surg. 2016;42(8):919–31.
56. Truong K, Prasidha I, Wain T. A systematic review of randomised controlled trials investigating laser assisted drug delivery for the treatment of keloid and hypertrophic scars. Lasers Med Sci. 2022;37(1):47-59.
57. Ji J, Tian Y, Zhu YQ, Zhang LY, Ji SJ, Huan J, et al. Ionizing irradiation inhibits keloid fibroblast cell proliferation and induces premature cellular senescence. J Dermatol. 2015;42(1):56-63.
58. Mankowski P, Kanevsky J, Tomlinson J, Dyachenko A, Luc M. Optimizing radiotherapy for keloids: a meta-analysis systematic review comparing recurrence rates between different radiation modalities. Ann Plast Surg. 2017;78(4):403-11.
59. Siotos C, Uzosike AC, Hong H, Seal SM, Rosson GD, Cooney CM, et al. Keloid excision and adjuvant treatments: a network meta-analysis. Ann Plast Surg. 2019;83(2):154-62.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}