


Larissa Daniele Machado Góes1; José Genival Alves de Macedo Júnior2; Manoel Benjamim de Almeida Barbosa3; Tayenne da Silva Gomes4; Lisandro Ferreira Lopes4
Submitted on: 20/02/2022
Approved on: 12/05/2022
Financial support: None
Conflict of interest: None
How to cite this article: Góes LDM, Macedo Júnior JGA, Barbosa MBA, Gomes TS, Lopes LF. Rosettes in cutaneous angiosarcoma: a new dermoscopic clue. Surg Cosmet Dermatol. 2022;14:e20220136
Cutaneous angiosarcoma is a rare cancer with a poor prognosis that affects mainly elderly men. It is related to chronic exposure to sunlight, chronic lymphedema, and procedures using radiation. We report a case of a 62-year-old man with a progressively growing violaceous tumor in the left temporal region. Dermoscopy showed erythematous areas of different shades, pseudo-follicular openings structures, and rosettes. The biopsy and the immunohistochemical study confirmed the diagnosis of cutaneous angiosarcoma. The patient is currently undergoing chemotherapy treatment in the oncology service with significant improvement of the lesion.
Keywords: Dermoscopy; Hemangiosarcoma; Skin neoplasms
Cutaneous angiosarcoma (CA) is a rare aggressive malignant vascular tumor with a poor prognosis, representing about 1.6% of soft tissue sarcomas.1 According to its origin, it can be classified into cutaneous angiosarcoma associated with chronic lymphedema (Stewart-Treves syndrome), radiation-induced cutaneous angiosarcoma, and cutaneous angiosarcoma of the head and neck.2 Cutaneous angiosarcoma can develop in various body regions, such as the breast, face, scalp, and limbs.3 However, more than half of all cases occur in the head and neck, especially on the scalp.2 The disease more frequently affects men over 60 years old, corresponding to about 85% of cases.4
Research indicates that the exacerbated expression of receptor tyrosine kinase and angiogenic growth factors are responsible for the deregulation of angiogenesis in cutaneous angiosarcoma.5 As for the location, primary cutaneous angiosarcoma occurs preferentially in photo-exposed skin6 while secondary cutaneous angiosarcoma usually occurs in areas that have previously undergone radiotherapy or with the presence of chronic lymphedema. Other studies associate cutaneous angiosarcoma with xeroderma pigmentosum, immunosuppression, and hemodialysis, due to its relationship with neovasculogenesis.6
Early lesions present as ill-defined violaceous to bluish areas with hardened borders. 7 At this stage, the disease must be differentiated from hematoma, rosacea, lupus erythematosus, and infections such as erysipelas and cellulitis. 7
The evaluation of vascular structures of skin lesions is applied to various fields, from tumor, inflammatory, and scalp lesions to the evaluation of nail fold capillaries in connective tissue diseases. 8 However, the assessment of color variations of lesions has been neglected. 9
The dermoscopic findings of angiosarcoma are scarce, being described mainly in case reports. It presents varied shades of erythema, from pink-purple areas with a white or skin-colored central zone to a peripheral violaceous tone;9 a reddish homogeneous area with white lines;10 vapor-like regions with a white or skin-colored central area and a violaceous periphery;11 a pink to violaceous erythema with white peri-follicular zones; a homogeneous violaceous to the black area covered by a whitish veil; or a diffuse violaceous erythema with follicular plugs.12
Rosette is a dermoscopic sign visible under polarized light, characterized by four white dots arranged like a 4-leaf clover.13 These structures can be found in melanocytic and nonmelanocytic lesions, and are not pathognomonic of any dermatosis.14,13 A series of 6,108 ex vivo dermatoscopies found rosettes in a variety of conditions such as scars (6.4%), dermatofibroma (6%), molluscum contagiosum (5.9%), squamous cell carcinoma (4.0%), basal cell carcinoma (1.7%), melanoma (1.4%), and nevi (0.7%).14 A recent description in the Brazilian literature identified rosettes in T-cell pseudolymphoma.15
The therapeutic modalities used to treat cutaneous angiosarcoma are surgery, radiotherapy, and chemotherapy.2 However, it tends to metastasize to regional lymph nodes and lungs, usually after repeated surgical excisions of the primary tumor. 16 The prognosis is poor, with a five-year survival rate of 10% to 35%.17
A 62-year-old man, without comorbidities, presented a progressively growing violaceous tumor on the left temporal region (Figure 1) for two weeks, accompanied by pain and local edema, with no previous history of trauma. Dermoscopy revealed the presence of erythematous areas of varying tones, structures similar to pseudo-follicular openings and rosettes (Figure 2). The initial diagnostic hypotheses were cutaneous abscess, primary cutaneous T-cell lymphoma of the follicular center type, and angiosarcoma. Systemic antibiotic therapy was instituted, and after 14 days, there was a significant enlargement of the lesion (Figure 3), infiltration of the face and scalp, and areas of ulceration and bleeding.
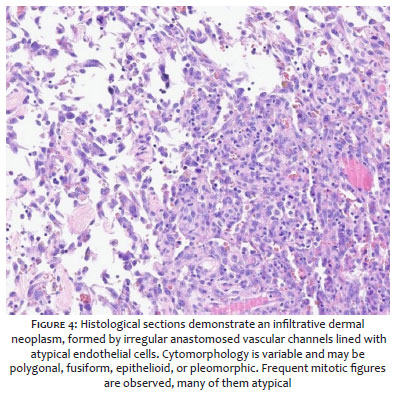
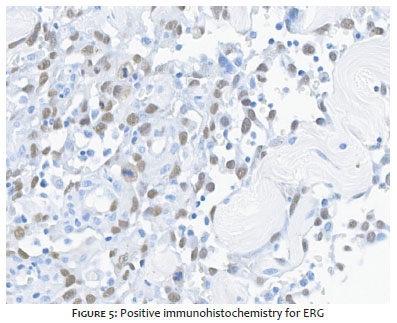
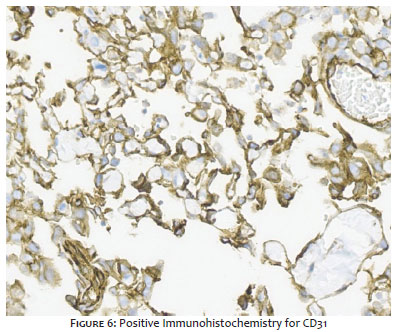
Skull CT scan showed extracranial formation in the left frontal pole without intracranial invasion. Chest, abdomen, and CT scans were normal. Serologies for HIV, hepatitis B, C, and syphilis were negative. Histopathological examination of the incisional biopsy of the lesion showed the presence of irregularly shaped anastomosing vascular channels lined by atypical cells and also spindle-shaped and epithelioid cells with ample eosinophilic cytoplasm, nuclei with coarse chromatin, evident nucleolus, and frequent mitotic figures (Figure 4). Immunohistochemistry was positive for ERG (Figure 5) and CD31 (Figure 6) and negative for HHV-8, confirming the diagnosis of angiosarcoma.
The patient was referred to the oncology service, where he is currently undergoing neoadjuvant intravenous chemotherapy with ifosfamide 1.8 g/m2, in 5 cycles, combined with doxorubicin 75 mg/m2, every three weeks, associated with granulocyte growth factor (G-CSF) 300 mcg/day, subcutaneously, with a daily dose divided into five applications. After treatment, we observed a substantial improvement in the lesion (Figure 7).
The description of rosettes in an angiosarcoma is, to the best of our knowledge, a new dermoscopic finding. We believe that sharing this information with the scientific community can broaden the range of differential diagnoses of dermatological diseases characterized by the presence of rosettes at dermoscopy, thus enabling early diagnosis and treatment of angiosarcoma.
Larissa Daniele Machado Góes 0000-0003-4140-3247
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
José Genival Alves de Macedo Júnior 0000-0001-7887-3723
Approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; critical literature review.
Manoel Benjamin de Almeida Barbosa 0000-0003-4283-4743
Approval of the final version of the manuscript; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Tayenne da Silva Gomes 0000-0003-3379-6028
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Lisandro Ferreira Lopes 0000-0003-2873-4332
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Bostancı S, Akay BN, Vural S, Ertop P, Heper AO. Hypopyon sign in dermatoscopy of cutaneous angiosarcoma. Australas J Dermatol. 2019;60(4):e366–8.
2. Fleury LFF Jr, Sanches JÁ Jr. Sarcomas cutâneos primários. An Bras Dermatol. 2006;81(3):207–21.
3. Ishida Y, Otsuka A, Kabashima K. Cutaneous angiosarcoma: Update on biology and latest treatment. Curr Opin Oncol. 2018;30(2):107–12.
4. Cruvinel SS, Bizinoto VP, Côrtes NCN, Macedo AM, Pereira DMA, Duarte AR. Peculiarities of cutaneous angiosarcoma. Brazilian J Plast Sugery. 2020;35(1):129–32.
5. Lyou Y, Barber E, Mehta R, Lee T, Goreal W, Parajuli R. Radiation - Associated Angiosarcoma of the Breast: a case report and literature review. Case Rep Oncol. 2018;11(1):216–20.
6. Ronchi A, Cozzolino I, Zito Marino F, Chiara A, Argenziano G, Moscarella E, et al. Primary and secondary cutaneous angiosarcoma: distinctive clinical, pathological and molecular features. Ann Diagn Pathol. 2020;48:151597.
7. Lallas A, Moscarella E, Argenziano G, Longo C, Apalla Z, Ferrara G, et al. Dermoscopy of uncommon skin tumours. Australas J Dermatol. 2014;55(1):53–62.
8. Oiso N, Kimura M, Kawada A. A dermoscopic figure of polymorphous atypical vessels with colour gradation. Metastatic cutaneous carcinoma into the lymphatic vessels. Acta Derm Venereol. 2011;91(6):737–8.
9. Oiso N, Matsuda H, Kawada A. Various colour gradations as a dermatoscopic feature of cutaneous angiosarcoma of the scalpaj. Australas J Dermatol. 2013;54(1):36–8.
10. Sanada T, Hata H, Sato K, Imafuku K, Kitamura S, Yanagi T, et al. Usefulness of dermoscopy in distinguishing benign lesions from angiosarcoma. Clin Exp Dermatol. 2017;42(6):676–8.
11. Caldarola G, Fania, L, Cozzani E, Feliciani, C. Simone C. Dyshidrosiform pemphigoid: a welldefined clinical entity? Eur. J. Dermatol. 2011;21(1):112-3.
12. Minagawa, A, Koga H, Okuyama R. Vascular structure absence under dermoscopy in two cases of angiosarcoma on the scalp. In. J Dermatol. 2014;53(7):e350-2.
13. González-Álvarez T, Armengot-Carbó M, Barreiro A, Alarcón I, Carrera C, García A, et al. Dermoscopic rosettes as a clue for pigmented incipient melanoma. Dermatol. 2014;228(1):31–3.
14. Liebman TN, Rabinovitz HS, Dusza SW, Marghoob AA. White shiny structures: dermoscopic features revealed under polarized light. J Eur Acad Dermatol Venereol. 2012;26(12):1493–7.
15. Alves RG, Ogawa PM, Enokihara MMSS, Hirata SH. Rosetas em pseudolinfa de células T: um novo achado dermatoscópico. An Bras Dermatol. 2021;96:68–71.
16. Wollina U, Hansel G, Schönlebe J, Averbeck M, Paasch U, Uhl J, et al. Cutaneous angiosarcoma is a rare aggressive malignant vascular tumour of the skin. J Eur Acad Dermatol Venereol. 2011;25(8):964–8.
17. Perrot JL, Habougit C, Biron Schneider AC, Couzan C, Tognetti L, Rubegni P, et al. Role of reflectance confocal microscopy and HD ultrasound in the diagnosis of cutaneous angiosarcoma of the breast. Ann Dermatol Venereol. 2019;146(5):410–3.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}