


Brayan Styven Merchan Rojas1; Jose Luis De-la-hoz1; Gustavo Facchini2; Gustavo Henrique da Silva2; Ana Lúcia Tabarini Alves Pinheiro3; Samara Eberlin2
Submitted on: 16/12/2021
Approved on: 16/07/2022
Financial support: Megalabs SAS, Bogotá, Colombia, sponsored this study
Conflict of interest: None
How to cite this article: Rojas BSM, De-la-hoz JL, Facchini G, Silva GH, Kawakami CM, Pinheiro ALTA, Eberlin S. Comparative study to evaluate the wound healing efficacy of topical formulations containing Triticum aestivum L. (Triticum vulgare) in a native human skin model. Surg Cosmet Dermatol. 2022;14:e20220118
INTRODUCTION: Plant extracts and actives derived from plants were developed to improve and enhance the skin healing process including Triticum aestivum L. (Triticum vulgare).
PURPOSE: To evaluate the effect of whole grain extract (EGTA-PR) and aqueous extract (EATA-FI) of Triticum aestivum L., on ex vivo skin healing.
METHODS: Skin fragments obtained from elective plastic surgery were subjected to tissue damage and treated with extracts for eight days for histological evaluation of re-epithelialization and immunofluorescence for epidermal growth factor (EGF).
RESULTS: EGTA-PR and EATA-FI accelerated the re-epithelialization process in human skin culture submitted to tissue injury. Additionally, we observed increased EGF protein labeling after treatment with EGTA-PR.
CONCLUSION: EGTA-PR showed a better performance in re-epithelialization when compared to EATA-FI, as it presented a higher protein labeling for EGF in human skin culture. Likewise, the histological results showed that the dermal redensification obtained with EGTA-PR was visually superior to that observed with EATA-FI. The results obtained are promising and corroborate the several biological actions already reported in the literature for Triticum aestivum L. extract in tissue healing stages.
Keywords: Regeneration; Epidermal growth factor; Triticum; In vitro techniques; Wound healing
Tissue healing is a dynamic and complex process composed of four phases: hemostasis, inflammation, proliferation, and tissue remodeling. After tissue injury, a clot is formed followed by infiltration of neutrophils, macrophages, and endothelial cells, promoting an inflammatory and immune response and providing tissue reconstruction.1
This metabolic arsenal produces cytokines, chemokines, and growth factors, stimulating and activating cell proliferation and migration, orchestrating the healing process.1-2 Among the growth factors, we highlight the epidermal growth factor (EGF), platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-β), vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF) and insulin-like growth factor (IGF).3-4
FGF, TGF-β, and PDGF stimulate fibroblast infiltration at the lesion site. TGF-β and PDGF also initiate phenotypic changes in these cells, converting fibroblasts into myofibroblasts that line the edges of the extracellular matrix, generating a constrictive force for wound closure.5-6
Hours after the damage, the re-epithelialization process begins, releasing EGF, TGF-β, FGF, and keratinocyte growth factor (KGF or FGF7), which stimulate the migration and proliferation of epithelial cells. Once the wound is closed, keratinocytes start the process of stratification and differentiation to restore the barrier.7-8
Matrix formation requires the removal of granulation tissue. Then the structure is saturated with proteoglycans and glycoproteins. Tissue remodeling involving TGF-β-mediated synthesis of new collagen and cleavage of old collagen by PDGF follows this step. The end product of this process is healing tissue.7-8
The healing success depends on growth factors, cytokines, and chemokines involved in a harmonic integration of signals that coordinate cellular processes. We assessed the effects of two herbal products for topical use containing standardized extracts of the species Triticum aestivum L. (synonym: Triticum vulgare) for skin re-epithelialization and tissue growth factors production using an experimental model of native human skin.
Megalabs SAS, Bogota, Colombia, supplied the topical herbal products containing standardized extracts of Triticum aestivum L. (Triticum vulgare). The chief formulation presents as an active ingredient the whole wheat Triticum aestivum L. grain extract (EGTA-PR; PROCICAR REGENERIX®). This extract is obtained under standardized time, lighting, and temperature conditions that favor the seeds’ activation and germination for subsequent aqueous extraction. These conditions favor the starch enzymatic hydrolysis and oligosaccharides production with certain molecular weights associated with pharmacological activity. To compare the specificities of each extraction method, we evaluated in parallel the biological responses produced by an herbal formulation containing Triticum aestivum L. aqueous extract (EATA-FI; FITOSTIMOLINE®).
The study used human skin from a 36-year-old female donor, skin phototype II, who underwent elective plastic surgery in the abdominal region (abdominoplasty). After the surgical procedure, the skin fragments were collected in plastic bottles with 0.9% saline solution and kept under refrigeration for up to 24 hours. This project does not include the storage and stock of biological material for future use. Therefore, the remaining fragments were properly disposed of as infectious waste. The Research Ethics Committee of Universidade São Francisco - SP, CAAE 82685618.9.0000.5514, approved the use of human skin fragments from elective surgery for this study under the number 2,493,285.
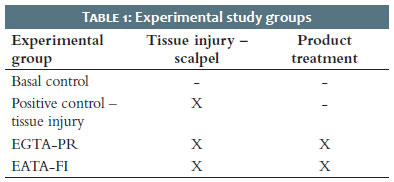
Human skin was fractionated into 12 fragments of approximately 1.5 cm2, distributed in triplicate to each of the four experimental groups (Table 1). The basal control group was maintained as the experimental control during the eight days, with only culture medium changes every 48 hours. The positive control included only tissue injury without treatment. The groups treated with EGTA-PR and EATA-FI were submitted to tissue lesions with a scalpel, treated daily with the evaluated products in the proportion of 25-30 mg/cm2, and kept in an incubator at 37°C in the presence of 5% of CO2 for eight consecutive days.
The skin fragments containing tissue lesions were treated during all incubation days. Then, the fragments were submitted to histological analysis to assess the epidermal re-epithelialization by hematoxylin & eosin staining (Sigma, San Luis, MO, USA) and to perform the immunofluorescence assay for EGF. We also collected skin culture supernatants for the quantification of KGF and TGF-β.
For histological evaluation, skin fragments were embedded in Tissue-Tek® O.C.T.TM, and then serial 12 micron sections were collected directly on cryostat silanized slides (Leica Biosystems, Buffalo Grove, IL, USA). The sections were washed with phosphate buffer and incubated overnight with anti-EGF (Bioss, Woburn, MA, USA). Subsequently, the sections were rinsed again and incubated for one hour with Alexa Flour 488-Secondary Antibody (Life Technologies, Calsbad, CA, USA). We performed a further incubation with DAPI (4’-6-diamidino-2-phenylindole; DNA tag; Sigma) followed by washes with phosphate buffer.
Slides were prepared using specific mounting media and analyzed under a microscope (Olympus, Tokyo, Japan) using standard CellSens software (© 2010 Olympus Corporation). We evaluated the intensity of the fluorescence parameter emitted by specific antibody labeling. After obtaining the images, the fluorescence intensity was quantified using the ImageJ software (version 1.48; Arbitrary Units - U.A.).
Quantification of KGF and TGF-β was conducted in the supernatant by enzyme immunoassay, using a kit purchased commercially (R&D Systems, Minneapolis, MN, USA). The absorbance reading was performed at 450 nm in a Multiskan GO monochromator (Thermo Scientific, Waltham, MA, USA).
The statistical evaluation used the ANOVA test to measure the variation of the results, comparing the data between the groups. Then, the Bonferroni post-test was applied, strengthening and making the ANOVA result more accurate. A significance level of 5% (GraphPad Prism v6) was used.
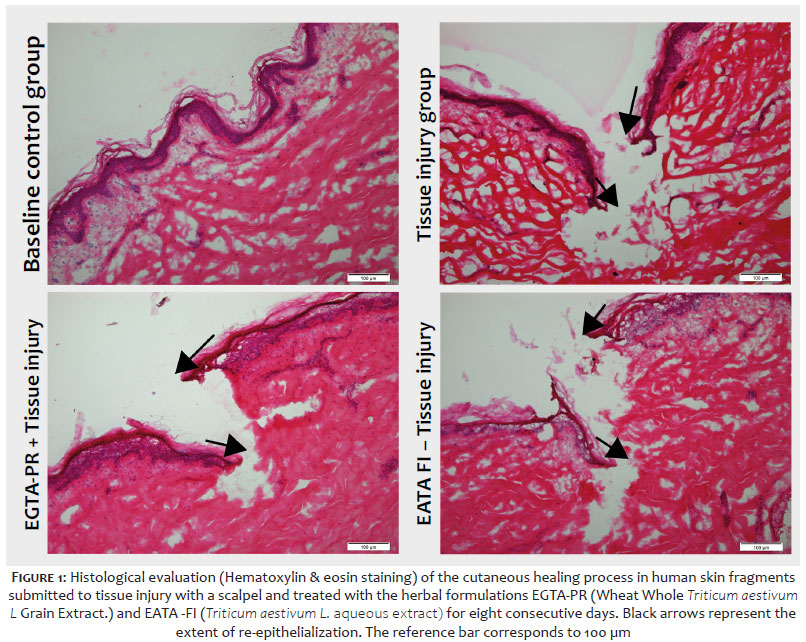
Figure 1 presents the results of the re-epithelialization process in fragments of native human skin submitted to tissue injury and treated with the EGTA-PR and EATA-FI formulations.
We can observe that the skin fragments submitted to the scalpel cut showed a tissue lesion in the epidermis and dermis. After eight days of culture, the group submitted only to the lesion showed a sign of re-epithelialization (represented by the black arrows in figure 1). However, the skin fragments submitted to both treatments with EGTA-PR and EATA-FI showed a higher re-epithelialization compared with the untreated group. Treatment with the formulations also demonstrated an improvement in dermal regeneration, visualized by redensification of the extracellular matrix, with emphasis on treatment with EGTA-PR.
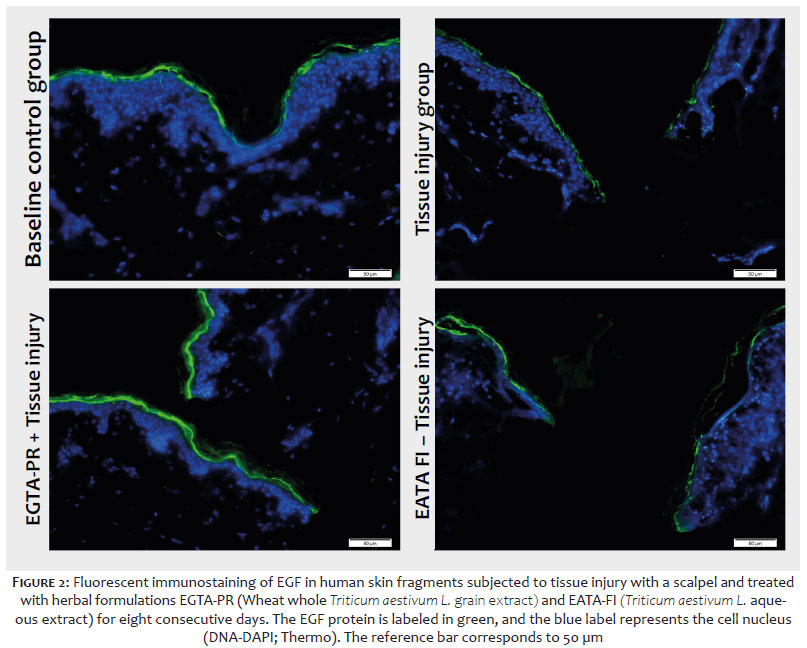
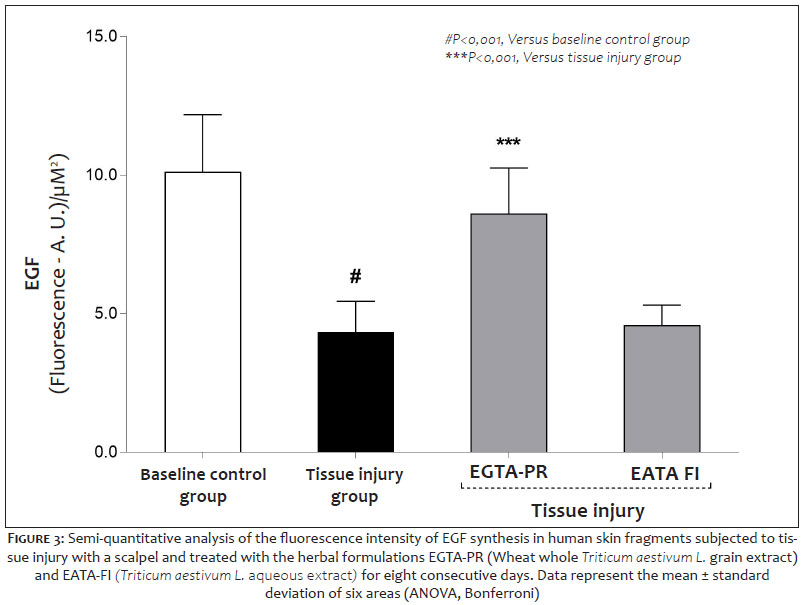
Figures 2 and 3 show the results of immunostaining and semi-quantitative analysis of EGF, respectively, in ex vivo skin fragments submitted to tissue injury with a scalpel and treated with the EGTA-PR and EATA-FI formulations.
Figure 3 represents the quantification of the fluorescence intensity of EGF through analysis of the images obtained in Figure 2. We can observe that the fragments submitted only to tissue injury with a scalpel showed a reduction of 57.18% in the production of EGF regarding the basal control (P<0.001) after eight days of culture. Treatment with the EGTA-PR formulation promoted an increase of 98.68% (P<0.001) in the production of EGF compared to the group submitted only to tissue injury. On the other hand, the EATA-FI formulation did not show significant changes in the production of EGF compared to the group with tissue injury.
Skin tissue integrity plays a vital role in interfacing with the external environment. Therefore, the occurrence of damage to this organ can result from an unsightly scar to the systemic disruption of the health of the being it involves.
Despite several modern skin care and treatment, healing does not always occur harmoniously. Tissue recovery after the damage is a complex process, dependent on the various cell types and mediators interacting in a highly sophisticated temporal sequence. It is a dynamic process, triggered in response to tissue injury, aiming to repair matrix and cellular damage and restore the integrity of the skin barrier, going through four overlapping phases: hemostasis, inflammation, proliferation, and remodeling.9
The healing process begins with the hemostasis phase, which consists of a blood clot formation that fills the lesion to stop bleeding and preserve tissue structures. This step is linked to the formation of a temporary matrix, the secretion of cytokines, and other growth factors that, when interacting with the components of the extracellular matrix (ECM), trigger the entire repair process. Subsequently, neutrophils under the influence of macrophages initiate the inflammatory phase, clearing the site of bacteria and debris and releasing pro-inflammatory cytokines and more growth factors responsible for the recruitment and activation of fibroblasts and epithelial cells.10
The proliferative phase begins, on average, on the third day of the injury and it is characterized by the reconstruction of the injured tissue and the increase in the number of cells at the wound site due to the migration and proliferation of fibroblasts, endothelial cells, and keratinocytes.11 During this phase, fibroblasts, in the presence of newly formed blood vessels, proliferate actively and synthesize ECM components that, in addition to their structural role, fulfill a signaling function, regulating the later stages of remodeling. This last phase occurs when the wound surface is contracted, a new epithelium is developed, and the final scar tissue is formed.
In this study, we assessed the effects of two topical formulations containing standardized extracts of Triticum aestivum L. (Triticum vulgare) on the skin re-epithelialization process, using an experimental model of human skin culture.12-13 The results showed that the formulation containing the whole wheat Triticum aestivum L. grain extract (EGTA-PR) and Triticum aestivum L. aqueous extract (EATA-FI) could accelerate the reepithelialization process after eight days of treatment in human skin culture submitted to tissue lesion. Additionally, increased dermal redensification and protein EGF labeling was observed, particularly after treatment with EGTA-PR.
It is essential to highlight that the results obtained with the formulation containing the whole Triticum aestivum L. grain extract (EGTA-PR) were more effective than those containing the aqueous extract (EATA-FI) in the parameters evaluated in this study. It is due to the particularities of the different processes for obtaining these extracts, which affect the phytochemical composition and, consequently, the pharmacological specificity.
These findings are crucial for the skin healing process, as they indicate the beginning of a proliferative phase that precedes remodeling and the formation of new tissue.14 The role of epidermal growth factor (EGF) has been extensively investigated in normal wound healing and pathological conditions and is implicated in keratinocyte migration, fibroblast function, and granulation tissue formation.15
Skin wound healing has been studied for decades, and several plant extracts and plant-derived actives have been developed to improve and potentiate the repair process. Among them, Triticum aestivum L. (Triticum vulgare) has been widely used in traditional medicine thanks to its acceleration of tissue repair properties.16-20
Several studies have shown that the T. aestivum L. extract could induce the proliferation of fibroblasts and endothelial cells, accelerating wound repair in part due to the presence of malto-oligosaccharides of molecular weight greater than 1000.21-25 In vivo studies in animal models confirmed this action, where the extract regenerated skin lesions.25 In addition to the extract›s regenerating properties, further evidence indicated its ability to reduce the inflammatory response and prevent irreversible tissue damage.26
Tito et al. also showed an action of the T. aestivum L. (T. vulgare) extracts in stimulating the synthesis of fibronectin, a key component in the formation and organization of the extracellular matrix, and also of the enzyme hyaluronan synthase 2, a precursor of the acid hyaluronic acid.9 These same authors attributed the property of restoring the skin barrier to the extract due to increased ceramides synthesis.9
Several extracts and isolated fractions of T. aestivum L. were assessed and confirmed the ability of this species in different mechanisms involved in the tissue regeneration process. However, the results reported in the literature and the data presented in this study demonstrate that the applied extraction method, in addition to the pharmacotechnical basis, is mandatory in the observed biological activity, making comparative performance studies difficult.
The results presented in this research constitute a predictive study using the experimental model of human skin from elective plastic surgery. This system represents, among the alternative methods, the one that is closest to a real condition of use, as it preserves the characteristics of the native skin cell population. Despite the promising results obtained in improving the tissue repair process, additional studies in this model and clinical ones are necessary to prove effectively this Triticum aestivum L. extracts action.
The speed and robustness of the tissue repair process are essential to forming an adequate and esthetically acceptable scar. Despite various modern care and treatments, the use of herbal products plays a vital role in wound healing, especially in complementary medicine. In this study, we assessed the effect of two herbal products for topical use containing standardized extracts of Triticum aestivum L. (Triticum vulgare) on wound healing, using an ex vivo model of skin re-epithelialization. The results allowed us to infer that the whole grain extract (EGTA-PR) presented a better performance in re-epithelialization than the aqueous extract (EATA-FI), as it presented a significantly higher EGF synthesis in human skin culture. Likewise, the histological results show that the dermal redensification obtained with EGTA-PR was visually superior to that observed with the aqueous extract. Although further studies are necessary, the results obtained with the whole wheat Triticum aestivum L. (Triticum vulgare) grain extract (EGTA-PR; PROCICAR REGENERIX®) are promising and corroborate the numerous biological actions already reported in the literature in the stages of tissue healing.
Brayan Styven Merchan Rojas 0000-0003-4322-1084
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Jose Luis De-la-hoz 0000-0001-9944-8961
Study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Gustavo Facchini 0000-0003-0111-7596
Statistical analysis; study design and planning; data collection, analysis, and interpretation.
Gustavo Henrique da Silva 0000-0003-0215-2246
Statistical analysis; study design and planning; data collection, analysis, and interpretation.
Ana Lúcia Tabarini Alves Pinheiro 0000-0002-0226-2544
Study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Samara Eberlin 0000-0001-7001-801X
Preparation and writing of the manuscript; critical literature review.
1. Martin P. Wound healing--aiming for perfect skin regeneration. Science. 1997;276(5309):75-81.
2. Hom DB, Linzie BM, Huang TC. The healing effects of autologous platelet gel on acute human skin wounds. Arch Facial Plast Surg. 2007;9(3):174-83.
3. Xie Z, Paras CB, Weng H, Punnakitikashem P, Su LC, Vu K, Tang L, Yang J, Nguyen KT. Dual growth factor releasing multi-functional nanofibers for wound healing. Acta Biomater. 2013;9(12):9351-9.
4. Koca Kutlu A, Ceçen D, Gürgen SG, Sayın O, Cetin F. A comparison study of growth factor expression following treatment with transcutaneous electrical nerve stimulation, saline solution, povidone-iodine, and lavender oil in wounds healing. Evid Based Complement Alternat Med. 2013;2013:361832.
5. Barrientos S, Stojadinovic O, Golinko MS, Brem H, Tomic-Canic M. Growth factors and cytokines in wound healing. Wound Repair Regen. 2008;16(5):585-601.
6. Hantash BM, Zhao L, Knowles JA, Lorenz HP. Adult and fetal wound healing. Front Biosci. 2008;13:51-61.
7. Raja, Sivamani K, Garcia MS, Isseroff RR. Wound re-epithelialization: modulating keratinocyte migration in wound healing. Front Biosci. 2007;12:2849-68.
8. Abraham J, Klagsbrun M. Modulation of wound repair by members of the fibroblast growth factor family. In: Clark RA, editor. The molecular and cellular biology of wound repair. 2nd ed. New York: Plenum Press; 1996. p.195-248.
9. Tito A, Minale M, Riccio S, Grieco F, Colucci MG, Apone F. A Triticum vulgare extract exhibits regenerating activity during the wound healing process. Clin Cosmet Investig Dermatol. 2020;13:21-30.
10. Lucas T, Waisman A, Ranjan R, Roes J, Krieg T, Müller W, et al. Differential roles of macrophages in diverse phases of skin repair. J Immunol. 2010;184(7):3964-77.
11. Velnar T, Bailey T, Smrkolj V. The wound healing process: an overview of the cellular and molecular mechanisms. J Int Med Res. 2009;37(5):1528-42.
12. Eberlin S, Facchini G, Silva GH, Eberlin S, Bragatto AR, Pinheiro ALTA, et al. Ex Vivo human skin: an alternative test system for skin irritation and corrosion assays. Altern Lab Anim. 2021;49(4):137-46.
13. Eberlin S, Silva MSD, Facchini G, Silva GHD, Pinheiro ALTA, Eberlin S, et al. The Ex Vivo skin model as an alternative tool for the efficacy and safety evaluation of topical products. Altern Lab Anim. 2020;48(1):10-22.
14. Lee HJ, Jang YJ. Recent understandings of biology, prophylaxis and treatment strategies for hypertrophic scars and keloids. Int J Mol Sci. 2018;19(3):711.
15. Hardwicke J, Schmaljohann D, Boyce D, Thomas D. Epidermal growth factor therapy and wound healing--past, present and future perspectives. Surgeon. 2008;6(3):172-7.
16. Lordani TVA, Lara CE, Ferreira FBP, Souza Terron Monich M, Mesquita da Silva C, Felicetti Lordani CR, et al. Therapeutic effects of medicinal plants on cutaneous wound healing in humans: a systematic review. Mediators Inflamm. 2018;2018:7354250.
17. Thakur R, Jain N, Pathak R, Sandhu SS. Practices in wound healing studies of plants. Evid Based Complement Alternat Med. 2011;2011:438056.
18. Lin TK, Zhong L, Santiago JL. Anti-inflammatory and skin barrier repair effects of topical application of some plant oils. Int J Mol Sci. 2017;19(1):70.
19. Martini P, Mazzatenta C, Saponati G. Efficacy and tolerability of fitostimoline in two different forms (soaked gauzes and cream) and citrizan gel in the topical treatment of second-degree superficial cutaneous burns. Dermatol Res Pract. 2011;2011:978291.
20. D'Agostino A, Pirozzi AVA, Finamore R, Grieco F, Minale M, Schiraldi C. Molecular mechanisms at the basis of pharmaceutical grade triticum vulgare extract efficacy in prompting keratinocytes healing. molecules. 2020;25(3):431.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}