


Bruna Souza Felix Bravo1; Raquel Melo Carvalho1; L'aís Bezerra de Menezes Penedo1; Fernanda Lourenço Prestes1; Samantha Talarico2; Sabrina Talarico2; Sergio Talarico2
Submitted on: 23/02/2021
Approved on: 17/05/2022
Financial support: None
Conflict of interest: None
How to cite this article: Bravo BSF, Carvalho RM, Penedo LBM, Prestes FL, Talarico S, Talarico S, Talarico S. Does SARS-CoV-2 vaccination affect the immediate effect of botulinum toxin? First impressions. Surg Cosmet Dermatol. 2022;14:e20220138
BACKGROUND: The SARS-CoV-2 infection has spread worldwide rapidly since its identification at the end of 2019. Globally, until April 2021, there have been more than 150 million confirmed cases of Covid-19, including over 3 million deaths. Therefore, a race was promptly started to produce an effective vaccine against the new virus. Botulinum toxin injection remains the leading non-surgical cosmetic procedure worldwide, with a high rate of efficacy and patient satisfaction.
AIMS: This study aims to analyze the association between the SARS-CoV-2 vaccine and the immediate botulinum toxin response.
MATERIALS AND METHODS: This was an observational, retrospective, and multicenter study. Data were collected between April and June 2021, and a medical record review of 71 patients from 27 to 76 years old treated with botulinum toxin injection.
RESULTS AND CONCLUSION: There were no meaningful changes in the immediate outcome of patients vaccinated for Covid-19 and botulinum toxin. However, it is vital to underline that follow-up and further studies are needed to define whether the Covid-19 vaccine can alter the duration of effect and efficiency of the botulinum toxin.
Keywords: Covid-19; Botulinum toxins type A; Vaccination
The SARS-CoV-2 infection has spread worldwide rapidly since its identification at the end of 2019.1 Globally, until April 2021, there have been more than 150 million confirmed cases of Covid-19, including over three million deaths.2
According to the Plastic Surgery Statistics, over 7.6 million botulinum toxin type A injections were performed in 2019, only in the U.S.A, including onabotulinumtoxinA (Botox Cosmetic, Allergan, Inc., Irvine, CA), abobotulinumtoxinA (Dysport, Valeant Pharmaceuticals International, Montreal, Canada), and incobotulinumtoxinA (Xeomin, Merz Pharmaceuticals, Frankfurt, Germany). This number raised continually year after year: from 2018 to 2019, it increased by 4%, while in the past two decades (2000-2019), when the procedure became popular, it increased by 878%, according to the same statistical source.3
Botulinum neurotoxin (BoNT) is a neurotoxic protein produced by the bacterium Clostridium botulinum, used in medical practice.4 The United States Food and Drug Administration (FDA) approved the OnabotulinumtoxinA (Botox®) and botulinum toxin type A (BoNT-A) for temporary improvement of glabellar lines and other noninvasive facial procedures in 2002.5 The botulinum toxin injection remains the leading non-surgical cosmetic procedure worldwide, with a high rate of efficacy and patient satisfaction.6
In this pandemic scenario, a race started promptly to produce an effective vaccine against the new virus. A candidate vaccine against SARS-CoV-2 might act against infection, disease, or transmission. A vaccine capable of reducing these elements could contribute to disease control and prevent further morbidity and mortality.7 The first vaccine was approved in December 2020, and currently, there are many valid vaccine options in the world. While we were developing this research, ANVISA (National Health Surveillance Agency) approved three vaccines for emergency use in Brazil: CoronaVac (Sinovac), Vaxzevria (AstraZeneca), BNT162b2 (Pfizer-BioNTech). Also, more options like the mRNA-1273 vaccine (Moderna) and JNJ-78436735 (Johnson & Johnson – Janssen) were available abroad.8
The Covid-19 pandemic may have changed patients’ motivations and priorities for aesthetic procedures. The major ones were to do something positive, refresh their look, and gain confidence. Patients also referred to frustration, anxiety, stress, and disappointment when they couldn’t perform aesthetic treatments due to the pandemic.9
As aesthetic physician experts, the authors have been asking themselves in their daily practice whether the SARS-Cov-2 vaccine can alter the botulinum toxin response. Considering that botulinum toxin is one of the foremost aesthetic procedures performed worldwide, and the Covid-19 vaccine should be offered to all individuals within the next years, this study aims to analyze the association between the SARS-CoV-2 vaccine and the immediate botulinum toxin response.
We performed an observational, retrospective, and multicenter study for consecutive patients who underwent botulinum toxin (Botox®, Allergan; Dysport®, Galderma; Xeomin®, Merz) injection for aesthetic purposes after having received at least the first dose of SARS-Cov-2 vaccine from April to June 2021 at Bravo Clinic in Rio de Janeiro and Talarico Dermatologic Clinic in São Paulo, Brazil. The study procedure followed the principles of the 1996 Declaration of Helsinki and obtained informed consent from each participant. We performed this research following regional laws and good clinical practice for studies on human subjects. The authors reviewed subjects’ basic information, photographs, image analysis results, and subjective assessments. A simple statistical analysis of the data was performed.
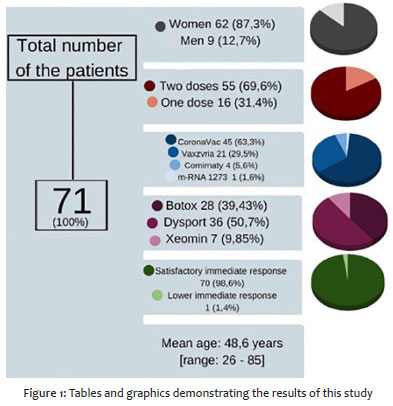
The sample investigated in this study consisted of n = 71 individuals: 9 men and 62 women. The mean age of the total sample was 48.6 years [range: 26 – 85] (Figure 1).
Fifty-three patients received two doses, while 16 patients received just one dose. Forty-five participants received CoronaVac (Sinovac), 21 Vaxzevria (AstraZeneca), 4 Comirnaty (Pfizer), and 1 patient received mRNA-1273 (Moderna). Patients received the first dose of vaccines, on average, 1.94 months before the botulinum toxin injection – ranging between 8 months to 24 hours earlier. The mean interval of the second dose was 0.88 months prior, with a maximum limit of 3 months before and 1 month later. Twenty-eight patients (39.43%) were treated with onabotulinumtoxinA (Botox Cosmetic, Allergan, Inc., Irvine, CA), 36 (50.7%) with abobotulinumtoxinA (Dysport, Valeant Pharmaceuticals International, Montreal, Canada), and 7 (9.85%) with incobotulinumtoxinA (Xeomin, Merz Pharmaceuticals, Frankfurt, Germany). The same physician that injected the BoNT-A clinically assessed all the patients enrolled in this study within 14 to 26 days after the procedure. The results were classified as mild, moderate, or satisfactory according to the improvement of dynamic wrinkles in the treatment area. Neither the physicians nor the patients observed significant inferior outcomes in the immediate result of botulinum toxin injection after being vaccinated against SARS-Cov-2 compared to their previous experiences, classifying their results as satisfactory. Only one of our patients had a moderate outcome, thus demanding a higher dose of botulinum toxin to obtain a satisfactory response, which represented 1.4% of studied individuals. Based on the small sample size, the authors reinforce that further studies are necessary to corroborate these findings.
Botulinum toxin injection is a well-established non-invasive aesthetic procedure with a muscle relaxation function that works by partially blocking nerve impulses for any muscles that have been injected and reducing excessive contractions of these muscles.10
The potent zinc proteinase neurotoxin binds to extracellular receptors on cholinergic nerve terminals, cleaving one of the three (SNARE) soluble N-ethylmaleimide-sensitive factor attachment receptor proteins. This action causes reversible inhibition of acetylcholine release by presynaptic vesicles intracellularly, leading to a transient restraint of neurotransmitter release at the neuromuscular junction. SNARE proteins also play an identified role in neurons, recognized to release glutamate, and substance R. Their actions release bradykinin, prostaglandins, histamine, and serotonin, which are proinflammatory mediators.11
As proteins synthesized by living organisms (Clostridial bacteria), botulinum toxins are biological products as opposed to conventional synthetic drugs.12
The SARS-CoV-2 virus may lead to a severe inflammatory response via elevation of cytokine levels including IL-6, IL-10, and TNF-α.2. In addition to direct viral damage, excessive inflammation and increased pro-inflammatory cytokine levels including IL-6, IL-8, TNF-α, and IL-1β are associated with disease severity and outcome in Covid-19.13
The Covid-19 Vaccine AstraZeneca is a monovalent vaccine composed of a single recombinant, replication-deficient chimpanzee adenovirus (ChAdOx1) vector encoding the S glycoprotein of SARS-CoV-2. The SARS-CoV-2 S immunogen in the vaccine is expressed in the trimeric prefusion conformation. The coding sequence has not been modified to stabilize the expressed S-protein in the pre-fusion conformation. Following administration, the S glycoprotein of SARS-CoV-2 is expressed locally and stimulates neutralizing antibody and cellular immune responses, which may contribute to protection from Covid-19.14
CoronaVac is an inactivated vaccine candidate against Covid-19. SARS-CoV-2 (CN02 strain) was propagated in African green monkey kidney cells (WHO Vero 10-87 cells) to prepare the vaccine. At the end of the incubation period, the virus was harvested, inactivated with β-propiolactone, concentrated, purified, and finally adsorbed onto aluminum hydroxide. The aluminum hydroxide complex was then diluted in sodium chloride, phosphate-buffered saline, and water before being sterilized and filtered for injection.15
Pfizer-BioNTech Covid-19 (BNT162b2) vaccine, a lipid nanoparticle-formulated, nucleoside-modified mRNA vaccine, encodes the SARS-CoV-2 spike glycoprotein prefusion, the virus that causes coronavirus disease 2019 (Covid-19). Vaccination with the Pfizer-BioNTech Covid-19 vaccine consists of two doses (30 μg, 0.3 mL each) administered intramuscularly, three weeks apart.16
Moderna Covid-19 (mRNA-1273) vaccine (ModernaTX, Inc; Cambridge, Massachusetts), a lipid nanoparticle-encapsulated, nucleoside-modified mRNA vaccine, encodes the stabilized SARS-CoV-2 spike glycoprotein prefusion. Vaccination with the Moderna Covid-19 vaccine consists of two doses (100 μg, 0.5 mL each) administered intramuscularly, one month (four weeks) apart.17
We performed a PubMed search to investigate if there are any reports about changes in the effect of botulinum toxin after vaccination, using the words “botulinum toxin & vaccine”, “botulinum toxin & vaccination”, and “onabotulinum toxin & vaccine”. One relevant article was found, comparing the protein structure of botulinum and tetanus toxins.
The tetanus toxin and BoNTs A and B show 50% amino acid similarity,18,19 and anti-tetanus toxin antibodies have been shown to bind to BoNTs A and B in vitro.20,21 It has been theorized that prior Immunogenicity of botulinum toxins immunization against tetanus may prime a patient’s immune system to BoNT.21 A preclinical study conducted in mice showed that prior active immunity against tetanus toxins did not enhance the host antibody response against injected BoNT.21 However, no clinical studies have been performed to examine whether this holds for humans.22 As little is known about Covid-19, the relationship between the SARS-Cov-2 vaccine and a possible modification of the immediate response to botulinum toxin has been questioned.
Since the number of patients seeking BTX treatment keeps growing as the vaccination happens throughout the world and the majority of the population gets vaccinated, it is essential to reassure the safety and efficacy of the aesthetic use of botulinum toxin.
Our study observed no meaningful changes in the immediate outcome of the patients who underwent botulinum toxin injection after being vaccinated against SARS-Cov-2 with the CoronaVac and Astrazeneca vaccines. As just one of our patients demanded a higher dose of botulinum toxin to obtain the satisfactory previous result, representing only 1,4% of studied patients, our sample is small and further studies will be necessary to elucidate if it is relevant.
The two main limitations of this study are the number of patients and their follow-up; however, this is an initial phase that could set the basis for future complete studies.
To the best of our knowledge, this is the first study analyzing the botulinum toxin immediate response in patients undergoing SArs-Cov-2 vaccination. This study is unprecedented and relevant because it aims to bring information about patients vaccinated for SARS-Cov-2 and treated with botulinum toxin in a moment when little is known about this disease. The injectors, who are experienced dermatologists, clinically evaluated all our patients.
There was no meaningful change in the immediate outcome of patients vaccinated for Covid-19 and submitted to botulinum toxin procedure. Because the number of patients seeking BTX treatment keeps growing as the vaccination happens throughout the world and the majority of the population gets vaccinated, it is essential to reassure the safety and efficacy of the aesthetic use of botulinum toxin.
It is paramount to underline that follow-up and further studies are necessary to define whether the Covid-19 vaccine can alter the duration of effect and efficiency of the botulinum toxin. There is a need to observe a larger number of cases and a longer follow-up, around six months.
Bruna Souza Felix Bravo 0000-0001-9692-7967
Approval of the final version of the manuscript; study design and planning; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Raquel Melo Carvalho 0000-0002-3991-4569
Preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Laís Bezerra de Menezes Penedo 0000-0002-8629-7196
Statistics analysis; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Fernanda Lourenço Prestes 0000-0001-5595-9639
Statistical analysis; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Samantha Talarico 0000-0001-9220-6572
Author's Contribution: Approval of the final version of the manuscript; data collection, analysis, and interpretation; critical revision of the manuscript.
Sabrina Talarico 0000-0002-7133-4900
Approval of the final version of the manuscript; Data collection, analysis, and interpretation; critical revision of the manuscript.
Sergio Talarico 0000-0002-5606-077X
Approval of the final version of the manuscript; study design and planning; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Türsen Ü, Türsen B, Lotti T. Aesthetic dermatology procedures in coronavirus days. J Cosmet Dermatol. 2020;19(8):1822-5.
2. World Health Organization [homepage]. Who coronavirus (Covid-19) Dashboard. Available at: https://Covid19.who.int/. Accessed on: 2021 April 28.
3. The Aesthetic Society. Top 5 procedures: surgical & nonsurgical. 2019. Available from: https://www.surgery.org/sites/default/files/Top-5.pdf.
4. Erro R, Scannapieco S, Russo M, Picillo M, Barone P. Impact of Covid-19 on neurological patients attending a botulinum toxin service. Neurol Sci. 2021;42(2):433-5.
5. Park MY, Ahn KY. Scientific review of the aesthetic uses of botulinum toxin type A. Arch Craniofac Surg. 2021;22(1):1-10.
6. Bravo BSF, Carvalho RM, Gallo BF, Bravo LG. A retrospective study supporting the importance of individualizing the dose of botulinum toxin according to the age. J Cutan Aesthet Surg. 2021;14(1):88-92.
7. Hodgson SH, Mansatta K, Mallett G, Harris V, Emary KRW, Pollard AJ. What defines an efficacious Covid-19 vaccine? A review of the challenges assessing the clinical efficacy of vaccines against SARS-CoV-2. Lancet Infect Dis. 2021;21(2):e26-e35.
8. Agência Nacional de Vigilância Sanitária (Brasil). Available at: https://www.gov.br/anvisa/pt-br.
9. Burleigh A, Beleznay K, Humphrey S. Aesthetic medicine during Covid-19: patient perspectives and motivations amidst a pandemic. J Cosmet Dermatol. 2021;20(3):711-3.
10. Allergan, Inc. Botox Cosmetic (botulinum toxin type A) purified neurotoxin complex (Package Insert). Irvine, CA: Allergan, Inc; 2019.
11. Padda IS, Tadi P. Botulinum toxin. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022.
12. Benedetto AV. Botulinum toxins in clinical aesthetic practices. 3th ed. Florida: CRC Press; 2018.
13. Akdogan N. Severe hyperalgesia and pain during botulinum toxin injection avoiding application in a patient 1 week after Covid-19 infection. J Cosmet Dermatol. 2021;20(3):755-6.
14. European Medicines Agency. Available at: https://www.ema.europa.eu/en/documents/product-information/Covid-19-vaccine-astrazeneca-product-information-approved-chmp-29-january-2021-pending-endorsement en.pdf
15. Wu Z, Hu Y, Xu M, Chen Z, Yang W, Jiang Z, et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine (CoronaVac) in healthy adults aged 60 years and older: a randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect Dis. 2021;21(6):803-12.
16. Oliver SE, Gargano JW, Marin M, Wallace M, Curran KG, Chamberland M, et al. The advisory committee on immunization practices' interim recommendation for use of Pfizer-BioNTech Covid-19 Vaccine - United States, December 2020. Morb Mortal Wkly Rep. 2020 18;69(50):1922-4.
17. Oliver SE, Gargano JW, Marin M, Wallace M, Curran KG, Chamberland M, et al. The advisory committee on immunization practices' interim recommendation for use of Moderna Covid-19 Vaccine - United States, December 2020. Morb Mortal Wkly Rep. 2021;69(5152):1653-6.
18. Whelan SM, Elmore MJ, Bodsworth NJ, Brehm JK, Atkinson T, Minton NP. Molecular cloning of the Clostridium botulinum structural gene encoding the type B neurotoxin and determination of its entire nucleotide sequence. Appl Environ Microbiol. 1992;58(8):2345-54.
19. Hutson RA, Collins MD, East AK, Thompson DE. Nucleotide sequence of the gene coding for non-proteolytic Clostridium botulinum type B neurotoxin: comparison with other clostridial neurotoxins. Curr Microbiol. 1994;28(2):101-10.
20. Halpern JL, Smith LA, Seamon KB, Groover KA, Habig WH. Sequence homology between tetanus and botulinum toxins detected by an antipeptide antibody. Infect Immun. 1989;57(1):18-22.
21. Dolimbek BZ, Jankovic J, Atassi MZ. Cross reaction of tetanus and botulinum neurotoxins A and B and the boosting effect of botulinum neurotoxins A and B on a primary anti-tetanus antibody response. Immunol Invest. 2002;31(3-4):247-62.
22. Naumann M, Boo LM, Ackerman AH, Gallagher CJ. Immunogenicity of botulinum toxins. J Neural Transm (Vienna). 2013;120(2):275-90.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}