


Gladstone E. L. Faria; Clarissa L. Vilela; Alyne Queiroga Bastos; Carolina Freitas Tavares Silva; Ricardo F. Boggio
Submitted on: 03/02/2021
Approved on: 05/05/2022
Financial support: None
Conflict of interest: None
How to cite this article: Faria GEL, Vilela CL, Bastos AQ, Silva CFT, Boggio RF. Loss of definition of the submental contouring: correct diagnosis and treatment algorithm. Surg Cosmet Dermatol. 2022;14:e20220131
The search for aesthetic procedures aimed at the loss of submental definition is increasing. A correct diagnosis is imperative for successful treatment and the reduction of complications. Localized adiposity, skin flaccidity, and loss of bone structure are the main findings. A treatment algorithm was discussed in this review, remembering, of course, the possibility of combined and sequential treatments for better results.
Keywords: Deoxycholic acid; Collagen; Neck; Chin; Adipose tissue; Hydroxyapatites
The loss of definition of the submental region is popularly called a double chin. This complaint has been increasingly frequent, mainly due to changes in life habits, especially the great exposure to cameras, whether for occupational reasons, in videoconferences, or for personal motives, in social media.1
The growing search for aesthetic procedures for this region has promoted the trivialization of treatments with imprecise indications, without the correct diagnosis, and, consequently, with high rates of complications.
The definition loss of the submental contouring has several etiologies that can often be associated and, thus, be considered multifactorial.1,2 To deem the etiology of the finding and then associate it with the correct treatment(s) is the key to avoiding unsatisfactory results and minimizing complication rates.
This study aims to review the literature to promote a critical analysis for a correct diagnosis of the loss of submental definition and create an algorithm to propose an adequate treatment.
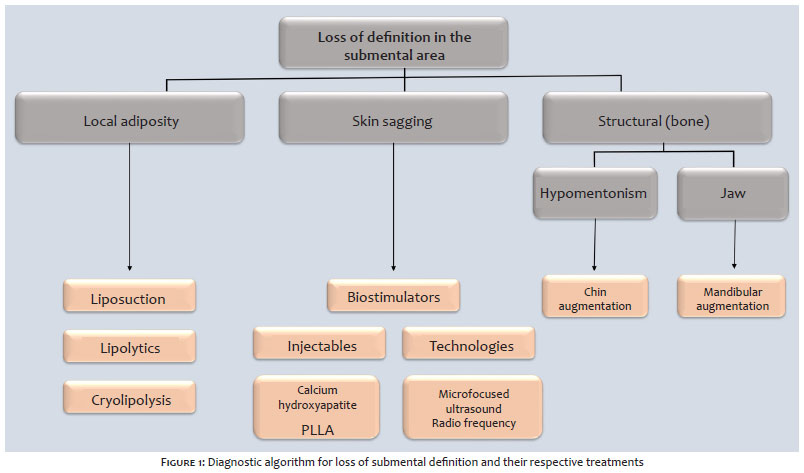
The main causes of submental contour loss are localized adiposity, skin flaccidity, and bone support loss (structural).
Understanding the anatomy of the cervicomental region is crucial for the correct diagnosis and therapeutic planning. The lower border of the mandible, the anterior border of the sternocleidomastoid muscle, the submental septum, the hyoid bone, and the thyroid cartilage delimit the cervicomental region. The sternocleidomastoid muscle into anterior and posterior triangles divides this area.
In the anterior triangle, we find the submental triangle, which is a single triangle of the neck, delimited by the body of the hyoid bone and the anterior bellies of the digastric muscle. It is the most important area in defining the contour of the face and is also the most affected by aging and adipose tissue accumulation. Therefore, it is the focus of most treatments that aim to improve the cervicomental angle.1,2,3
The accumulation of fat in the submental region is one of the most frequent complaints of patients, and can be correlated with obesity, genetic conditions, life habits, and acquired lipodystrophies.4
Treatment consists of removing excess fat, either by surgical methods, such as liposuction (still considered the gold standard) or minimally invasive methods.
Among the minimally invasive methods, we can highlight injection lipolysis (popularly known as enzymes) and cryolipolysis.
The natural aging process, the law of gravity, and weight fluctuations, constantly influence the skin in this region. The clinical finding is palpation without an increase in the volume of adipose tissue, but an overhanging, atrophic, and flaccid skin, causing damage to the contour of the area.5
This finding, in addition to the etiological conditions mentioned above, can also be considered secondary, resulting from treatments involving localized adiposity, which did not evolve with adequate skin retraction.
When skin flaccidity is the patient’s diagnosis, minimally invasive treatments become focused on skin quality, that is, on collagen biostimulators, whether injectables, threads, or technologies.
We highlight calcium hydroxyapatite, poly-L-lactic acid, and polydioxanone (PDO) threads among the injectable collagen biostimulators. Among the technologies, we spotlight microfocused ultrasound and radiofrequency.
The structural cause is the etiology related to the loss of bone support. It can be congenital, due to underdevelopment of the lower third of the face, or acquired, due to the bone aging process, which becomes more accelerated with the loss of dentition.6
Poor mandibular contour and/or hypomentonism are the two major structural causes and, once again, must be properly evaluated and treated. The replacement of these segments in a minimally invasive, simpler, and safer way is done with hyaluronic acid fillers.7
Figure 1 proposes a diagnostic algorithm and its respective treatment, recognizing that multifactorial causes are often found and, therefore, should be treated together or through sequential treatment protocols.
With this algorithm, it is easy and reasonable to indicate the appropriate treatments, considering the individual experience of each professional as well as access to the different therapeutic modalities mentioned here.
Submental fat liposuction is a minor surgical method that can be performed in an outpatient setting, with local anesthesia, or in a hospital setting associated with other procedures. The surgical technique eliminates excess adipose tissue from the subcutaneous tissue of the cervical region, improving the neck’s contour and definition with effective and lasting results and minimal downtime. Thus, this procedure is the gold standard.
The ideal patient for liposuction is young, has good skin quality, lacks sagging, and has loss of cervical contour secondary to the accumulation of fat in the submental and submandibular region. The patient needs to understand that liposuction does not replace weight loss. Although, unlike body indication, patients with a BMI above the ideal also benefit from the aesthetic results of liposuction in this region.8
The upper and lower margins of the fat compartment and its lateral limits must be demarcated. The limits of the sternocleidomastoid muscle (SCM) must be respected and serve as an anatomical reference for vascular structures of the neck. It is also essential to define the region between the lower border of the mandible and the anterior margin of the masseter muscle, where the marginal nerve of the mandible is more superficial.3
The incisions are planned according to each patient’s adiposity distribution and in most cases a single submental puncture is sufficient. Additional punctures in the insertion of the earlobe bilaterally can be used, as an exception, by more experienced professionals, due to a higher vascular risk.
Infiltration of the area is conducted with modified Klein’s solution, prepared using saline solution, lidocaine, bupivacaine, and adrenaline 1:250,000. Infiltration is performed with a 2-2.5 mm Klein cannula until the area becomes tumescent. It is recommended to wait 10-15 minutes before starting liposuction so that the vasoconstrictor effect of adrenaline takes place, thus reducing the risk of bleeding and bruising. The liposuction technique must respect the subcutaneous plane, always above the platysma muscle. The surgeon introduces the cannula through the hole in the neck in slight hyperextension, and guides its path with the contralateral hand, controlling its tip throughout the procedure to protect the deep planes from possible violations. Short cannulas of 2 mm to 3 mm in caliber are recommended, always with the holes facing downwards. Dermal lesions or superficial liposuctions can result in skin necrosis and surface irregularities, respectively.9
Compressive dressing and/or surgical mesh are recommended to avoid the formation of seromas and hematomas, and for adequate skin adhesion to the deep tissues. Skin retraction varies according to the individual characteristics of each patient but in the foreseeable possibility of little skin retraction and residual sagging, technologies aimed at skin tightening can be indicated for intraoperative use, such as diode laser, plasma jet, or radiofrequency.
Lymphatic drainage should be performed by a trained professional and started in the early postoperative period. Proper technique and frequency are essential for rapid recovery and to avoid complications such as fibrosis. Serious complications are rare, including marginal mandibular nerve neuropathy and vascular injuries. Bleeding, seroma, residual flaccidity, irregularities, and banding are the most frequent complications.
Submental liposuction is a simple, fast, and safe procedure,9 which allows the definitive resolution of the accumulation of subcutaneous fat in the submental region and has a high level of satisfaction (Figure 2).
The two main injectable lipolytic agents are deoxycholic acid and phosphatidylcholine, which can be used separated or combined for synergistic effects. Sodium deoxycholate is a bile salt with similar detergent properties used to solubilize phosphatidylcholine. It plays a central role in the emulsification and digestion of fats in the intestine. Ionic detergents such as deoxycholate disrupt membrane integrity by introducing their polar hydroxyl groups into the hydrophobic core of the bilayer, leading to membrane collapse into mixed micelles of phospholipids and detergent molecules.1,2
Phosphatidylcholine is a glycerophospholipid that facilitates the emulsification of fats, allowing absorption and transport of fat. The mechanism of subcutaneous fat lysis by phosphatidylcholine is still the subject of studies. It has been postulated that it stimulates lipases and breaks down triglycerides into fatty acids and glycerol.10
The combination of both has a synergistic action and causes vacuolization of the adipocyte, leading to its destruction and elimination by phagocytosis. It is speculated that deoxycholate in monotherapy promotes immediate and accentuated fat necrosis, with essential fibrotic effects, while its association with phosphatidylcholine it promotes a more organized fat necrosis. Therefore, the most common formulations comprise the two active ingredients in concentrations ranging from 2.5-5% for phosphatidylcholine and 2.5-4.7% for sodium deoxycholate.11
The selection of the ideal patient is essential for a good result. Treatment works best for soft fat compared to hard or fibrous fat. The latter is found more often found in young women and men.
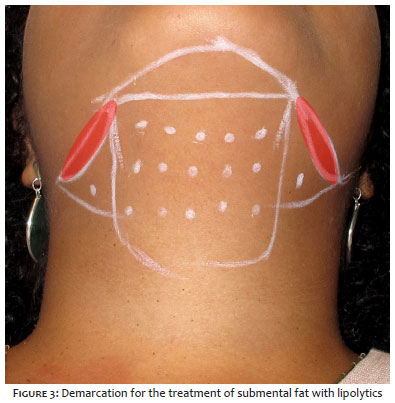
The application technique is relatively simple. The fat compartment is demarcated according to the following anatomical parameters: submental sulcus anteriorly, hyoid bone posteriorly, and a line that descends from the oral commissures laterally. After the delimitation of the area, injection points equidistant 1 cm from each other are marked. A safety zone is demarcated between 1 cm and 1.5 cm from the mandibular border, a region that should not be treated, under the risk of injury to the marginal nerve of the mandible (Figure 3).12
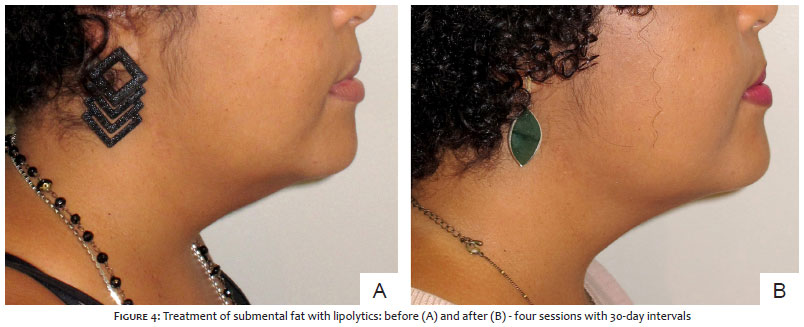
After adequate asepsis with alcoholic chlorhexidine, injections of 0.2 mL per point in the subcutaneous plane are performed, using a 1 mL syringe and a 30 G x 13 mm needle. The bi-digital pinch of the fat increases the assertiveness of the application depth, which should be from 6 mm to 10 mm. An average volume of 3-5 mL (30-50 mg) per session is recommended, avoiding extrapolating the total volume of 10 mL in the same application (corresponding to 100 mg of deoxycholate). Three to five sessions, at least four weeks apart, should be encouraged for best results (Figure 4).13
Edema, erythema, and mild pain are frequent and start within the first five minutes post-injection and last an average of 24-48 hours. Paresthesias can last longer, like two weeks. Severe complications, such as mandibular marginal nerve injury, manifest clinically with smile asymmetry, but fortunately, most resolve spontaneously. Skin ulcerations may occur as a result of superficial applications.
Cryolipolysis is a technique that applies cooling to the skin surface to promote the lysis of adipocytes, in this case, pre-platysmal adipocytes. The safety of non-invasive technology is related to the higher susceptibility of adipose tissue to injury by cooling, to the detriment of other tissues such as the skin, due to its water content. Studies prove the ability to reduce the submental fat layer by around 20%.14
In vivo, histopathological studies showed that cryolipolysis induces cellular apoptosis on the third day, with an inflammatory response between the third and 14th day, and subsequent phagocytosis by macrophages between the 14th and 30th day. In the following two-three months, there is a thickening of the interlobular septa and a significant loss of fat cells.
The FDA approved its use in the submental region in 2015, and studies have shown that cryolipolysis is a safe, comfortable, and effective treatment for reducing submental fat. The main adverse events are hematoma, erythema, edema, and paresthesia. Paradoxical adipose hyperplasia is an adverse event described with an incidence of 1:20,000 treatments and is more related to men,12, and should be treated with liposuction.
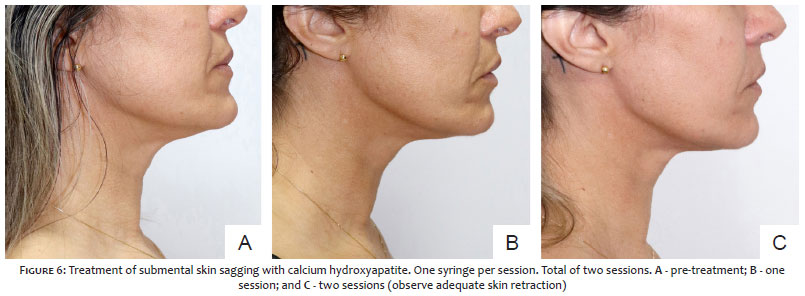
Injectable calcium hydroxyapatite is a valuable tool with biostimulating properties, that is, the production of collagen and elastic fibers, in addition to an excellent ability to retract the skin. Hydroxyapatite stands out in neck treatment since it can increase skin thickness, something very desired for this region, associated with improved elasticity, especially with great safety, especially regarding the formation of nodules.15,16
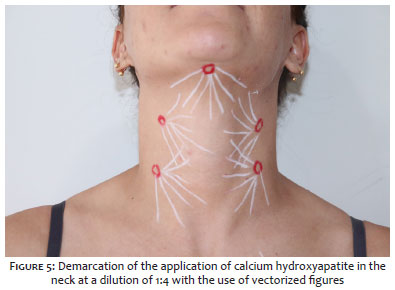
The neck is usually treated with higher dilution when compared to the face. A 1:4 dilution is usually effective and safe for this procedure. A syringe containing 1.5 mL of a product receives 6 mL of diluent (a lidocaine and saline solution). Vectorized figures are drawn covering the entire region, and the application is performed through linear retroinjections in the subdermal plane using a 22 g microcannula (Figure 5).17 Usually, three sessions, with intervals of 30 days, are recommended for better results (Figure 6). The massage performed immediately by the injector, associated with home self-massage twice a day for seven days, is indicated for better distribution and homogenization of the product.16
Poly-L-lactic acid is another tool for injectable neck biostimulation. As with calcium hydroxyapatite, neck region treatment is considered body therapy and therefore requires a higher dilution than that for facial treatment.18
The recommended dilution for neck treatment with poly-L-lactic acid provides a final total volume of 16 mL, and the protocol of prior or immediate dilution can be followed.15,16 The distribution of the diluted product in the area to be treated follows the fanning-type application technique, preferably with a microcannula, in the subdermal plane. Post-application massage care follows the same criteria as previously recommended for calcium hydroxyapatite.
Nodules are the main complication regarding the injectable biostimulator, especially poly-L-lactic acid.19 Fortunately, most are more palpable than visible and self-limiting without any treatment. Visible nodules can be treated with a vigorous massage, intranodular injection of distilled water with or without lidocaine, associated with massage to dilute the product, and, in refractory cases, intranodular injection of 5-fluorouracil and corticosteroids. Granulomas manifest as inflammatory nodules and are even rarer.
PDO threads (polydioxanone monofilament) are absorbable sutures that will be absorbed while stimulating collagen production, once positioned in the tissue. The traction threads have cones that anchor the skin and subcutaneous tissue, thus allowing lateral traction of the submentum sagging also generating a biostimulus as they are reabsorbed. Its positioning in the correct plan in this region requires the professional’s high degree of expertise. Otherwise, irregularities and skin pinch may occur in addition to the risk of damage to noble structures in the subplatysmal plane.20
On the other hand, straight threads applied in a juxtadermal plane in hashtag or parallel have the sole objective of collagen biostimulation and are used increasingly in this region due to their ease of application. However, it is noteworthy that the results are directly proportional to the number of threads per region.
The most frequent complications are hematoma, infection, irregularity, migration, and even extrusion. Less experienced professionals can also cause injury to deep structures in the neck.
The careful selection of the candidate patient for the threads is an essential point for the success of the treatment. Patients with low BMI, whose only change in the cervical region is flaccidity, are excellent candidates, while obese patients with large volumes in the submentum will have limited results.21
Microfocused ultrasound is a non-invasive device that promotes thermal injury and repair in the tissue through the ultrasound wave directed to the target tissue, resulting in collagen stimulation, tissue-lifting effect, and increased thickness of the local skin. Direct visualization allows higher safety in the treatment, in addition to more promising results by adequately reaching the target tissue.22
Numerous studies prove the device’s effectiveness for the neck region, promoting the improvement of fine wrinkles, sagging, texture, and skin retraction, both in monotherapy and associated with calcium hydroxyapatite. When treatments are combined, the effects are synergistic and can be performed on the same day, starting with technology.22,23
Radiofrequency is another device capable of improving skin quality and stimulating collagen. Its mechanism of action is the transformation of radiofrequency, applied to the skin, into thermal energy in the different layers of the skin through the frictional heating of molecules exposed to the electromagnetic field. Different tissues conduct electrical currents differently and, therefore, have different impedances, mainly related to the degree of hydration. Fat tissue has high electrical resistance and, as such, responds by generating more heat. Heat induces tissue damage, activates the inflammatory system, and the lesion repair process culminates in collagen production and skin quality improvement.24
There are several radio frequency options available: monopolar, bipolar, and multipolar, each with or without temperature control. Kinney, in 2018, demonstrated that, for the neck, the preferred protocol would be multipolar radiofrequency, with temperature control, protocoled with at least five sessions.24,25
Finally, the neck region benefits from a valuable technique that uses radiofrequency associated with microneedling. This association makes it possible to deliver radiofrequency energy directly to the area to be stimulated at a predetermined depth. It reaches better results, achieving higher temperatures and more safety, minimizing the adverse events of epidermal heating.26
The structural cause is determined by the lack of support underlying the skin, especially the jawbones. When there is not adequate support, the skin becomes redundant, resulting in apparent excess skin. A correct diagnosis of the cause of double chin is essential because, despite simulating sagging skin, which would be treated with collagen biostimulators, the cause lies in the lack of stretching of this skin and should, therefore, be treated with improved bone support.4,5,7
The lack of bone support can be congenital, due to a deficiency in the development of the mandibular bones, especially in mouth breathing patients. However, the bone resorption process inherent to the aging process can also cause it.6
The origin of the structural loss can be divided. In most cases, hypomentonism is observed and stretching and/or projection of the chin with hyaluronic acid fillers is indicated. In certain situations, the treatment of the chin can be associated with the mandibular contour improvement, promoting the three-dimensional stretching of the skin of the submental region. Individual characteristics between genders should receive special attention before filling in these regions to avoid dysmorphisms and stigmas.27,28,29
Figure 7 shows a treatment protocol for a patient diagnosed with a double chin with structural origin. In this case, stretching and projection of the chin were performed, associated with mandibular contour improvement. Supraperiosteal bolus points with high G-prime and high normal strength hyaluronic acid were used for the projection (pink points – bolus). Treatments in the subcutaneous plane were associated with stretching the chin (filling in the labrum-mental groove) and oral support at the pre-jowl level (in a triangle in Figure 7), which contributes to better mental projection, in addition to filling the body and ramus of the jaw. Figure 7 describes the doses and these points, collaborating to stretch the redundant skin in a three-dimensional way.
It is noteworthy that any patient with loss of contour of structural origin may be a candidate for definitive treatment with orthognathic surgery and this possibility should be considered before the cosmiatric procedure.
The popularly called “double chin” is something much more complex and deserves much more respect than what it has been approached recently. Neglecting this anatomical region, especially when treated by non-qualified professionals, can lead to a higher incidence of complications, which are often avoidable. A correct diagnosis and an adequate therapeutic indication, often with the creation of sequential protocols, are essential conditions for the best results.
Gladstone E. L. Faria 0000-0002-0754-2019
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Clarissa L. Vilela 0000-0003-2077-1614
Approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; critical literature review; critical revision of the manuscript.
Alyne Queiroga Bastos 0000-0002-1020-4221
Approval of the final version of the manuscript; active participation in research orientation; critical revision of the manuscript.
Carolina Freitas Tavares Silva 0000-0003-3224-5099
Approval of the final version of the manuscript; critical revision of the manuscript.
Ricardo F. Boggio 0000-0002-5139-0243
Approval of the final version of the manuscript; active participation in research orientation; critical revision of the manuscript.
1. Vanaman M, Fabi SG, Cox SE. Neck rejuvenation using a combination approach: our experience and a review of the literature. Dermatol Surg. 2016;42(Suppl 2):S94-100.
2. Dunican KC, Patel DK. Deoxycholic Acid (ATX-101) for reduction of submental fat. Ann Pharmacother. 2016;50(10):855-61.
3. Shah A, Cunha B. Anatomy, head and neck, anterior cervical region. Treasure Island: StatPearls [Internet]; 2020.
4. Farkas JP, Pessa JE, Hubbard B, Rohrich RJ. The science and theory behind facial aging. Plast Reconstr Surg Glob Open. 2013;1(1):e8-e15.
5. Cotofana S, Fratila AA, Schenck TL, Redka-Swoboda W, Zilinsky I, Pavicic T. The anatomy of the aging face: a review. Facial Plast Surg. 2016;32(3):253-60.
6. Toledo LEA, Cardoso MA, Bordoni LS, Avelar LM, Avelar JVM. Aging and sexual differences of the human skull. Plast Reconstr Surg Glob Open. 2017;5(4):e1297.
7. Braz A, Eduardo CCP. Reshaping the lower face using injectable fillers. Indian J Plast Surg. 2020;53(2):207-18.
8. Stebbins WG, Hanke CW. Rejuvenation of the neck with liposuction and ancillary techniques. Dermatol Ther. 2011;24(1):28-40.
9. Kridel RWH, Conderman CP. Liposuction of the face and neck: the art of facial sculpture In: Papel I. Facial Plastic and Reconstructive Surgery. 4th ed. New York: Thieme; 2016. p. 202-21.
10. Duncan DI, Palmer M. Fat reduction using phosphatidylcholine/sodium deoxycholate injections: standard of practice. Aesthetic Plast Surg. 2008;32(6):858-72.
11. Rotunda AM, Weiss SR, Rivkin LS. Randomized double-blind clinical trial of subcutaneously injected deoxycholate versus a phosphatidylcholine-deoxycholate combination for the reduction of submental fat. Dermatol Surg. 2009;35(5):792-803.
12. Liu M, Chesnut C, Lask G. Overview of Kybella (Deoxycholic Acid Injection) as a fat resorption product for submental fat. Facial Plast Surg. 2019;35(3):274-7.
13. Humphrey S, Femmer P, Beleznay K, Carruthers JDA. Deoxycholic acid for submental fullness and more: real-world experience with 202 patients. Dermatol Surg. 2019;45(4):624-7.
14. Lipner SR. Cryolipolysis for the treatment of submental fat: review of the literature. J Cosmet Dermatol. 2018;17(2):145-1.
15. Yutskovskaya YA, Kogan EA. Improved neocollagenesis and skin mechanical properties after injection of diluted calcium hydroxylapatite in the neck and décolletage: a pilot study. J Drugs Dermatol. 2017;16(1):68-74.
16. Almeida AT, Figueredo V, Cunha ALG, Casabona G, Faria JRC, Alves EV, et al. Consensus recommendations for the use of hyperdiluted calcium hydroxyapatite (Radiesse) as a face and body biostimulatory agent. Plast Reconstr Surg Glob Open. 2019;7(3):e2160.
17. Faria GEL, Santos DB, Tartare A, Bento AM, Boggio RF. Standardization of the body vectoring technique with calcium hydroxyapatite. Surg Cosmet Dermatol. 2020;12(S2):172-8.
18. Haddad A, Menezes A, Guarnieri C, Coimbra D, Ribeiro E, Sarubi J, et al. Recommendations on the use of injectable Poly-L-Lactic acid for skin laxity in off-face areas. J Drugs Dermatol. 2019;18(9):929-35.
19. Kadouch JA. Calcium hydroxylapatite: a review on safety and complications. J Cosmet Dermatol. 2017;16(2):152-61.
20. Karimi K, Reivitis A. Lifting the lower face with an absorbable polydioxanone (PDO) thread. J Drugs Dermatol. 2017;16(9):932-4.
21. Suh DH, Jang HW, Lee SJ, Lee WS, Ryu HJ. Outcomes of polydioxanone knotless thread lifting for facial rejuvenation. Dermatol Surg. 2015;41(6):720-5.
22. Pavicic T, Ballard JR, Bykovskaya T, Corduff N, Hirano C, Park JY, et al. Microfocused ultrasound with visualization: consensus on safety and review of energy-based devices. J Cosmet Dermatol. 2022;21(2):636-47.
23. Casabona G, Nogueira Teixeira D. Microfocused ultrasound in combination with diluted calcium hydroxylapatite for improving skin laxity and the appearance of lines in the neck and décolletage. J Cosmet Dermatol. 2018;17(1):66-72.
24. Gentile RD, Kinney BM, Sadick NS. Radiofrequency technology in face and neck rejuvenation. Facial Plast Surg Clin North Am. 2018;26(2):123-34.
25. Dayan E, Chia C, Burns AJ, Theodorou S. Adjustable depth fractional radiofrequency combined with bipolar radiofrequency: a minimally invasive combination treatment for skin laxity. Aesthet Surg J. 2019 8;39(Suppl_3):S112-9.
26. Weiner SF. Radiofrequency microneedling: overview of technology, advantages, differences in devices, studies, and indications. Facial Plast Surg Clin North Am. 2019;27(3):291-303.
27. Maio M, Wu WTL, Goodman GJ, Monheit G; Alliance for the Future of Aesthetics Consensus Committee. Facial assessment and injection guide for botulinum toxin and injectable hyaluronic acid fillers: focus on the lower face. Plast Reconstr Surg. 2017;140(3):393e-404e.
28. Sakuma TH, Hirano CF, Braz AV. How to project or lengthen the chin with soft tissue fillers respecting sexual dimorphism. Dermatol Surg. 2021;47(11):1524-5.
29. Faria GEL, Bento AM, Santos DB, Tartare A, Boggio RF. Facial beautification with fillers and main differences between genders. Rev Bras Cir Plast. 2021;36(1):100-7.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}