


Luisa Homem de Mello Maciel Campilongo1; João Gabriel Rodrigues Alberti1; Francisco Macedo Paschoal1; Marisa Homem de Mello Maciel Campilongo1 ; Fernanda Modolo de Paula Moura Campos2
Submitted on: 13/01/2022
Approved on: 21/02/2022
Financial support: None
Conflict of interest: None
How to cite this article: Campilongo LHMM, Alberti JGR, Paschoal FM, Campilongo MHMM, Campos FMPM. Neurothekeoma of the left upper eyelid: rare case report. Surg Cosmet Dermatol. 2022;14:e20220124
Neurothekeomas are rare, benign dermal tumors of presumed fibrohistiocytic lineage. They present multiple differential diagnoses, making their identification challenging at the dermatological and anatomopathological examination. We report the case of a 28-year-old man who presented a hardened papule growth on the left upper eyelid with histopathology and immunohistochemistry suggestive of neurothekeoma.
Keywords: Eyelid neoplasms; Neurothekeoma; Case reports
Neurothekeoma (NTs) are rare, benign, superficial soft tissue neoplasms of presumed fibrohistiocytic lineage. Generally, they affect women (F:M, 2:1) in the second and third decades and present as pink-erythematous, solitary, well-defined, slow-growing papules or nodules, asymptomatic, with a diameter smaller than 2 cm.1,2
Despite being described in 1969, NTs present uncertain pathogenesis and diverse histological patterns. The multiplicity of differential diagnoses, including the anatomopathological one, makes its identification challenging.1-3
A 28-year-old man, skin phototype V, observed the appearance and growth of a hardened papule on the left upper eyelid (Figure 1) six months ago. He denied pain, itching, or secretion and reported frequent manipulation and sun exposure. He had no relevant dermatological personal history. Regarding his family history, he mentioned “skin cancer” (sic) in his maternal grandmother. We opted for excision of the lesion and sent the material for anatomopathological examination.
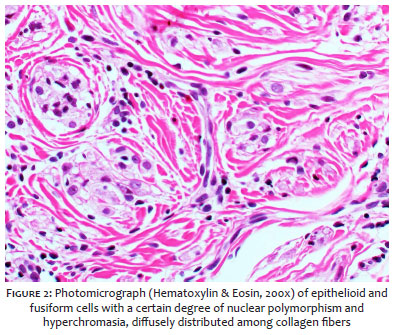
The anatomopathological examination showed a dermal lesion composed of fusiform/oval cells arranged randomly with collagenized stroma, areas of collagen entrapment in the periphery, intermingled capillary proliferation, and rare mitotic figures (Figure 2).
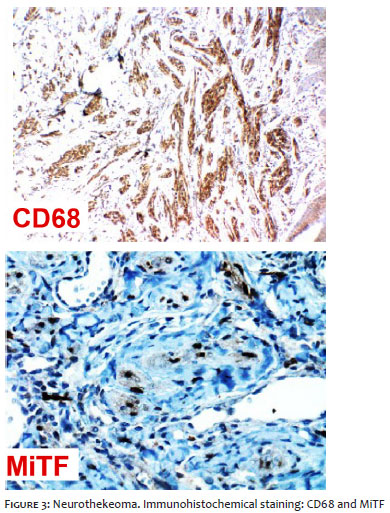
The immunohistochemical study revealed expression for CD68 and MiTF and negativity for HMB-45, p16, BCL2, and protein S-100 (Figure 3). A low proliferative index (1%) was reported. Lesion findings fell within the spectrum of plexiform fibrohistiocytic tumor/ neurothekeoma. However, the immunoexpression of MiTF favored the diagnosis of neurothekeoma.
At follow-up the patient had a recurrence with the same aspects as the previous lesion two months after excision.
Neurothekeoma is a rare, benign dermal neoplasm of uncertain pathogenesis and frequent diagnostic difficulty.1,2 Until 2019, the literature described only 10 case reports of eyelid neurothekeoma.4
The differential diagnosis of NTs is diverse and includes benign, malignant, and inflammatory neoplasms. Histology is the gold standard for diagnosis and is characterized by the presence of a circumscribed and lobular dermal lesion. Nests of epithelioid cells or tumor cells predominate in a subtle spiral pattern. Abundant eosinophilic granular cytoplasm, with round or oval nuclei, is observed.1,3
NTs are classified according to the anatomopathological amount of the myxoid matrix. Their immunohistochemical profile is not specific. However, they are typically reactive to NK1-C3 and CD10 and negative to S-100, HMB-45, Melan-A, and CD56.3
Recent studies in histogenetics have evaluated the close relationship between NTs and plexiform fibrohistiocytic tumors. Even with common histogenesis, microphthalmia-associated transcription factor (MiTF) expression can be used as a reliable marker to differentiate between tumors.2,5
The chance of TN recurrence after surgical excision is approximately 3%,3 and its complications are restricted to an aesthetic scar.1
Given the unusual presentation of NTs and their clinical-histological similarities with benign and malignant tumors, head and neck surgeons, dermatologists and pathologists should be aware of the morphobiological spectrum of the neoplasm to perform an accurate diagnosis and appropriate treatment and follow-up of the patient.1
Luisa Homem de Mello Maciel Campilongo 0000-0002-1555-807X
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
João Gabriel Rodrigues Alberti 0000-0001-6495-8419
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Francisco Macedo Paschoal 0000-0002-6264-1538
Approval of the final version of the manuscript; study design and planning; data collection, analysis, and interpretation; active participation in research orientation; critical literature review; critical revision of the manuscript.
Marisa Homem de Mello Maciel Campilongo 0000-0001-7584-3748
Approval of the final version of the manuscript; study design and planning; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Fernanda Modolo de Paula Moura Campos 0000-0001-7471-4717
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Kao EY, Kernig ML. Neurothekeoma [Internet]. Treasure Island (FL): StatPearls Publishing; c2020 [citado em 20 Mar 2021]. Disponível em: https://www.ncbi.nlm.nih.gov/books/NBK519525/.
2. Stratton J, Billings SD. Cellular neurothekeoma: analysis of 37 cases emphasizing atypical histologic features. Mod Pathol. 2014;27(5):701-10.
3. Navarrete-Dechent C, Curi-Tuma M, Marín C, González S, Sandoval-Osses M. Cellular neurothekeoma: case report and its (un) relation with nerve sheath myxoma. An Bras Dermatol. 2015; 90(3 Suppl 1):156-9.
4. Choe S, Lee KS, Khwarg SI, Kim N. Rare case of nerve sheath myxoma of the eyelid misdiagnosed as mucocele. Korean J Ophthalmol. 2019;33(2):202-3.
5. Fox MD, Billings SD, Gleason BC, Moore J, Thomas AB, Shea CR, et al. Expression of MiTF may be helpful in differentiating cellular neurothekeoma from plexiform fibrohistiocytic tumor (histiocytoid predominant) in a partial biopsy specimen. Am J Dermatopathol. 2012;34(2):157-60.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}