


Elisa Nunes Secamilli1; Juliana Yumi Massuda-Serrano1; Rafael Fantelli Stelini2; Thais Helena Buffo1; Paulo Eduardo Neves Ferreira Velho1
Submitted on: 21/12/2021
Approved on: 27/01/2022
Financial support: None
Conflict of interest: None
How to cite this article: Secamilli EN, Massuda-Serrano JY, Stelini RF, Buffo TH, Velho PENF. Exclusive surgical treatment of a primary cutaneous marginal zone lymphoma: a case report. Surg Cosmet Dermatol. 2022;14:e20220120
Primary cutaneous B-cell lymphomas are non-Hodgkin lymphomas presenting only in the skin and represent 25% of all primary cutaneous lymphomas. Based on their clinical behavior, they are classified into indolent and intermediate forms. Treatment of indolent forms includes surgery, radiotherapy, and, in extensive disease, rituximab. We report a case of a 57-year-old woman with a single nodule in the left arm treated with surgical excision with 5-mm security margins, without relapse after 36 months. Surgery is a therapeutic option in these lymphomas without compromising disease-free survival.
Keywords: Lymphoma B-Cell; Lymphoma B-Cell marginal zone; Lymphoma non-Hodgkin; Surgical oncology
Primary cutaneous B-cell lymphomas (PCBCL) are B-cell non-Hodgkin lymphomas that affect the skin exclusively, with no evidence of systemic involvement in the initial evaluation. They represent approximately 25% of primary cutaneous lymphomas, with an incidence of four cases per million people, and they are more frequent in men and after 50 years of age.1 They are divided into two main clinical groups through their morphological and immunophenotypic analysis: marginal zone and centrofollicular, considered to have indolent clinical behavior; and primary cutaneous large B-cell lymphoma, leg type, and primary cutaneous intravascular large B-cell lymphoma, regarded as presenting intermediate clinical behavior.2
There are no randomized trials to treat indolent primary cutaneous B-cell lymphomas (PCBCLs). The treatment is indicated based on case series and consensus from the World Health Organization (WHO) and the European Organization for Research and Treatment of Cancer (EORTC). Low-dose radiotherapy, surgery, or intralesional infiltration of corticosteroids or rituximab are the therapy of choice for localized disease. Clinical follow-up, multi-field radiotherapy, or rituximab may be indicated in patients with multiple lesions.1 Surgical treatment still does not have well-established protocols, and it is not possible to know the ideal surgical security margin or whether or not the size of the margin influences the recurrence of lesions.
We report the case of a patient with PCBCL of the marginal zone, surgically treated with 5 mm security margins, without recurrence in 36 months of follow-up.
A 57-year-old white woman reported the appearance of an asymptomatic lesion in the left upper limb for three years. She denied fever, weight loss, or night sweats (Figures 1).
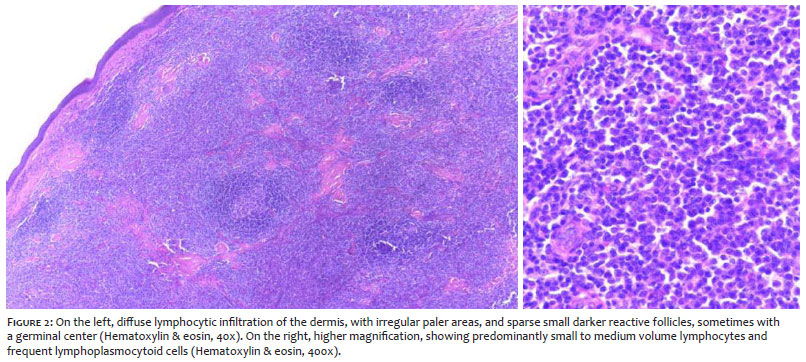
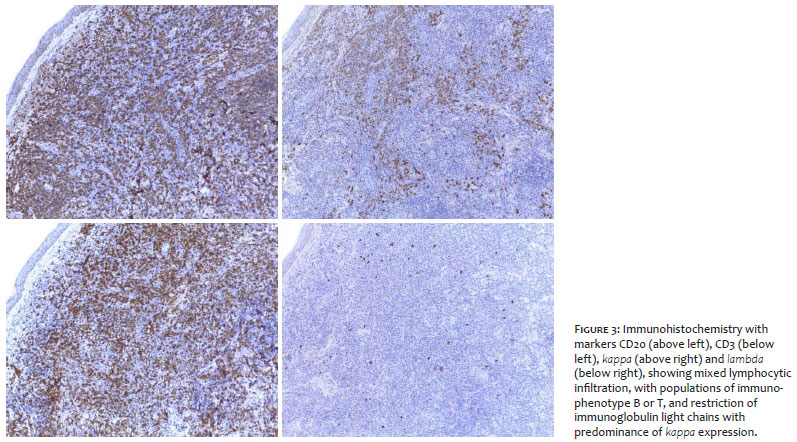
The examination showed clustered papules and lumpy nodules, forming a 1.5 cm x 1.2 cm plaque on the left arm. There was no peripheral lymphadenopathy or palpable visceromegaly. Clinical hypotheses included cutaneous lymphoma, sarcoidosis, pseudolymphoma, lupus tumidus, and tertiary syphilis. The histopathological study with immunohistochemical assay showed nodular and diffuse lymphocytic infiltration in the dermis, with 60% of this infiltrate composed of lymphocytes (CD20+, CD10- and BCL6-), frequent reactive T lymphocytes (CD3+), Ki67 proliferation index relatively low (10-20%), frequent plasma cells, and immunoglobulin light chain restriction (kappa: lambda index greater than 10:1), suggesting the diagnosis of marginal zone B-cell lymphoma (Figures 2 and 3).
After this result, we investigated systemic disease using computed tomography scans of the neck, chest, abdomen, and pelvis, which did not show extracutaneous manifestations. Laboratory tests, including blood count and LDH, were normal, and serology for HIV and syphilis were not reactive.
The diagnosis of PCBCL of the T1a marginal zone was made. We chose surgical excision with 5 mm security margins as the patient had a single lesion. The patient has been under outpatient follow-up for 36 months, with no local recurrence or appearance of new lesions.
Marginal zone PCBCL is an indolent cutaneous lymphoma with a five-year survival rate close to 100%. The reported case presents an excellent oncological and cosmetic result in a 57-year-old woman with high estimated survival.
Little is known about the possibility of recurrence with surgical treatment of indolent PCBCL. A study by Servitje et al., 2013, including only patients with marginal zone PCBCL, showed no difference in the recurrence rate or disease-free survival between the groups treated with surgery, radiotherapy, or surgery + radiotherapy. There was a non-statistically significant increase in initial site recurrence in patients treated with surgery alone.3
Parbhakar and Cin retrospectively analyzed the database of their oncology center and identified 25 patients with indolent PCBCL: 16 treated with low-dose radiotherapy (30-40 Gy) and nine treated with surgical excision with a 5 mm security margin. Only one patient treated with radiotherapy had a recurrence and underwent surgical excision. The mean follow-up time was four years. The authors also report no local complications in patients treated with surgery; on the other hand, 14/16 of patients treated with radiotherapy had acute radiodermatitis, and 2/16 had a chronic ulcer at the irradiated site lasting up to a year and a half.4
Hamilton et al. retrospective analysis revealed that four of 12 patients treated with surgery experienced recurrence at the treated site. In this same series, only two of the 92 patients treated with radiotherapy had a recurrence in the irradiated field. However, there was no difference in disease-free survival at five years, which means that radiotherapy as a secondary treatment can be delayed until clinical recurrence of the lymphoma, without changing the patient’s prognosis.5
In conclusion, surgical treatment is a valid option for radiotherapy in patients with primary cutaneous B-cell lymphomas of indolent clinical behavior with single or localized lesions. The rarity of the disease leads to scarcity of randomized clinical studies between the two therapeutic modalities, as well as the definition of the ideal surgical margins. Based on the previous studies, the authors used a 5 mm security margin. Long-term follow-up of these patients is recommended.
Elisa Nunes Secamilli 0000-0001-9036-4200
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Juliana Yumi Massuda-Serrano 0000-0002-5221-2385
Approval of the final version of the manuscript; study design and planning; ; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Rafael Fantelli Stelini 0000-0003-0618-1693
Study design and planning; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Thais Helena Buffo 0000-0002-6833-7596
Study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Paulo Eduardo Neves Ferreira Velho 0000-0002-7504-8370
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; critical literature review; critical revision of the manuscript.
1. Wilcox RA. Cutaneous B-cell lymphomas: 2018 update on diagnosis, risk stratification, and management. Am J Hematol. 2018;93(11):1427-30.
2. Willemze R, Cerroni L, Kempf W, et al. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood. 2019;133(16):1703-14.
3. Servitje O, Muniesa C, Benavente Y, Monsálvez V, Garcia-Muret MP, Gallardo F, et al. Primary cutaneous marginal zone B-cell lymphoma: Response to treatment and disease-free survival in a series of 137 patients. J Am Acad Dermatol. 2013;69(3):357-65.
4. Parbhakar S, Cin AD. Primary cutaneous B-cell lymphoma: role of surgery. Can J Plast Surg. 2011;19(2):e12-4.
5. Hamilton SN, Wai ES, Tan K, Alexander C, Gascoyne RD, Connors JM. Treatment and outcomes in patients with primary cutaneous B-cell lymphoma: the BC Cancer Agency experience. Int J Radiat Oncol Biol Phys 2013;87(4):719- 25.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}