


Betty Nguyen1; Antonella Tosti2
Submitted on: 29/10/202
Approved on: 17/01/2022
Financial support: None
Conflict of interest: None
How to cite this article: Nguyen B, Tosti A. Papel da dermatoscopia na distinção entre tinea nigra e nevos melanocíticos acrais. Surg Cosmet Dermatol. 2022;14:e20220108.
Dermoscopy is a practical, non-invasive tool that can be used to distinguish tinea nigra from other lesions that appear macroscopically similar, including acral nevus. Under dermoscopy, tinea nigra presents with a pattern of spiculated gray-brown pigment deposition, whereas acral nevus most often presents as brown pigment deposition in a parallel furrow pattern.
Keywords: Dermoscopy; Nevus; Tinea
Tinea nigra is an uncommon superficial mycosis of the stratum corneum caused by Hortaea werneckii, an ascomycetous yeast thought found primarily in soil, compost, and wood in (sub)tropical regions. It is characterized by the insidious onset of an asymptomatic brown-to-black macule with discrete borders. The lesions are usually unilateral and solitary, though multiple lesions can also be present. Tinea nigra preferentially affects the palmar surfaces of the hands and plantar surfaces of the feet, though they can occasionally extend to the fingers and toes. Spontaneous resolution of lesions is unlikely but has been reported.1 Topical antifungal agents generally resolve tinea nigra within 2-4 weeks.2
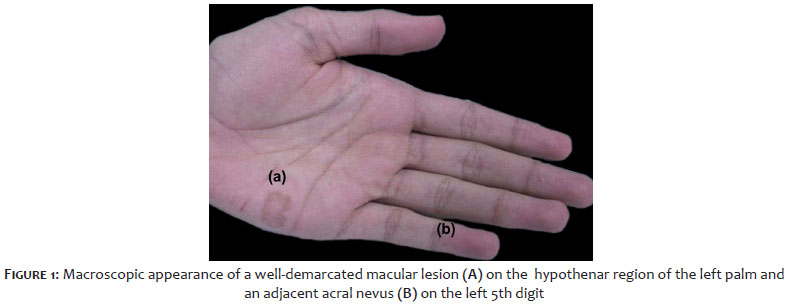
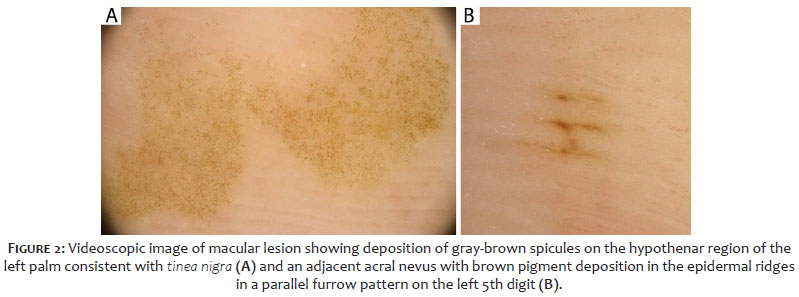
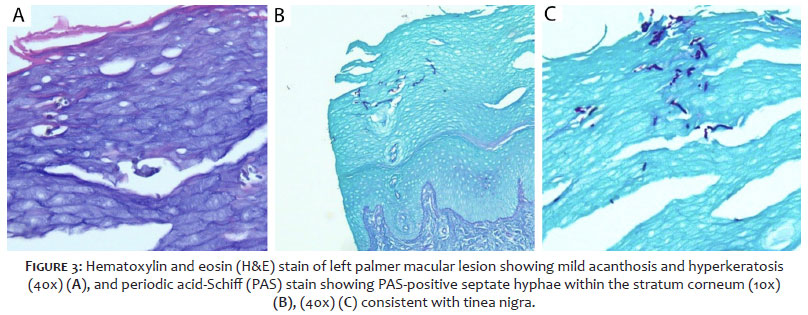
A 14-year-old man with no significant family or medical history presented to the clinic with a brown lesion on his left palm for “years.” He reported no pain or discomfort. The patient was born in Cuba and moved to the United States when he was 8. He denied significant travel history. The physical exam showed a visible macular lesion with sharp borders on the left palm in the hypothenar region (Figure 1A) and a smaller adjacent macular lesion on the left 5th digit (Figure 1B). Dermoscopy of the hypothenar lesion revealed deposition of regular gray-brown spicules (Figure 2A). Also, dermoscopy of the adjacent 5th digit lesion showed brown pigment deposition predominantly in the linear furrows consistent with acral nevus (Figure 2B). Potassium hydroxide (KOH) preparation from skin scrapings of the left palmar lesion showed branched brown hyphae with light brown septa. The subsequent polymerase chain reaction was positive for Hortaea werneckii. We observed mild acanthosis and hyperkeratosis on hematoxylin and eosin (H&E) stain (Figure 3A), and periodic acid-Schiff (PAS)-positive septate hyphae within the stratum corneum, consistent with tinea nigra (Figure 3B).
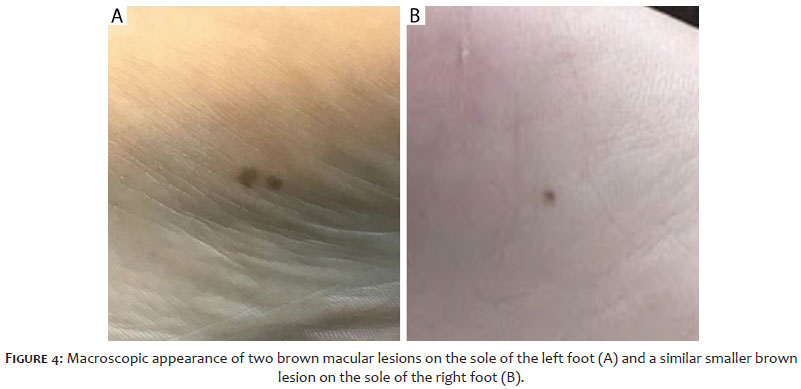
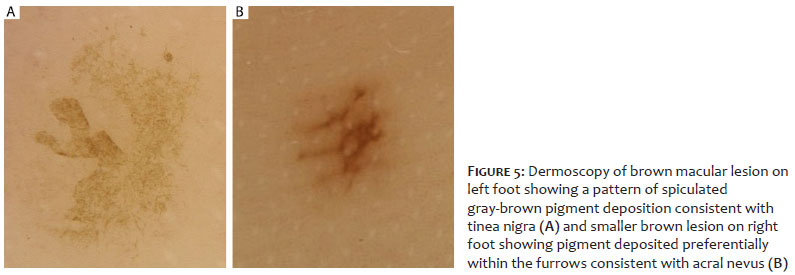
A 43-year-old man with no significant family or medical history presented to the clinic with a brown macular lesion on the sole of his left foot, as well as a smaller brown macular lesion on the sole of his right foot (Figure 4A-B). He reported no pain or discomfort. The physical exam was otherwise unremarkable. The patient was born in the United States and denied relevant travel history. Dermoscopy of the left foot lesion revealed a pattern of spiculated gray-brown pigment deposition suggestive of tinea nigra (Figure 5A), confirmed on biopsy. Also, dermoscopy of the smaller brown lesion on the right foot showed pigment deposited predominantly within the furrows suggestive of acral nevus (Figure 5B).
Given the macroscopic appearance and distribution of its lesions, tinea nigra can resemble many other conditions, including acral nevi3 and acral lentiginous melanoma4. Prompt and accurate recognition of tinea nigra is required to minimize unneeded invasive diagnostic testing, such as surgical excision. Dermoscopy can provide a quick, non-invasive, and accurate diagnosis. The dermoscopic hallmark of tinea nigra is the presence of gray-brown or light brown spiculated pigments distributed throughout the skin without preference for ridges or furrows.5, 6 In contrast, dermoscopy of acral nevi most often reveals unevenly distributed brown pigment in a parallel furrow pattern.7 One study of 50 cases found that the presumptive diagnosis of tinea nigra was made in 7/13 (53%) of cases when dermoscopy was used, as compared to 0/37 (0%) of cases that did not use this method (P<0.001).6 Recent case reports8-10 have confirmed the similar diagnostic utility of dermoscopy in tinea nigra. Our two cases reiterate the importance of dermoscopy in the clinical evaluation of these lesions to ensure prompt diagnosis and treatment initiation while minimizing the need for invasive testing.
Betty Nguyen 0000-0002-0402-3926
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Antonella Tosti 0000-0001-5516-4043
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Rossetto AL, Cruz RC. Spontaneous cure in a case of Tinea nigra. An Bras Dermatol. 2012;87(1):160-2.
2. Bonifaz A, Badali H, Hoog GS, Cruz M, Araiza J, Cruz MA, et al. Tinea nigra by Hortaea werneckii, a report of 22 cases from Mexico. Stud Mycol. 2008;61:77-82.
3. Eksomtramage T, Aiempanakit K. Tinea nigra mimicking acral melanocytic nevi. IDCases. 2019;18:e00654.
4. Babel DE, Pelachyk JM, Hurley JP. Tinea nigra masquerading as acral lentiginous melanoma. J Dermatol Surg Oncol. 1986;12(5):502-4.
5. Gupta G, Burden AD, Shankland GS, Fallowfield ME, Richardson MD. Tinea nigra secondary to Exophiala werneckii responding to itraconazole. Br J Dermatol. 1997;137(3):483-4.
6. Piliouras P, Allison S, Rosendahl C, Buettner PG, Weedon D. Dermoscopy improves diagnosis of tinea nigra: a study of 50 cases. Australas J Dermatol. 2011;52(3):191-4.
7. Altamura D, Altobelli E, Micantonio T, Piccolo D, Fargnoli MC, Peris K. Dermoscopic patterns of acral melanocytic nevi and melanomas in a white population in central Italy. Arch Dermatol. 2006;142(9):1123-8.
8. Thomas CL, Samarasinghe V, Natkunarajah J, Fogo A. Entodermoscopy: a spotlight on tinea nigra. Int J Dermatol. 2016;55(2):e117-8.
9. Abinader MVM, Maron SMC, Araújo LO, Ado AS. Tinea nigra dermoscopy: a useful assessment. J Am Acad Dermatol. 2016;74(6):e121-2.
10. Nazzaro G, Ponziani A, Cavicchini S. Tinea nigra: a diagnostic pitfall. J Am Acad Dermatol. 2016;75(6):e219-e220.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}