


Francine Papaiordanou1; Gabriela Pacheco de-Oliveira2; Doris Hexsel3; Antonio Carlos Amedeo Vattimo4
Submitted on: 09/11/2021
Approved on: 22/11/2021
Financial support: None
Conflict of interest: None
How to cite this article: Papaiordanou F, Oliveira GP, Hexsel D, Vattimo ACA. Colágeno e pele: da estrutura às evidências de sua suplementação oral. Surg Cosm Dermatol. 2022;14:20220110
In the aging process, the intracellular routes that regulate collagen homeostasis are influenced by the exposome, resulting in its degradation and decreased synthesis, leading to sagging skin. Current evidence indicates that oral collagen supplementation may promote wrinkles reduction in the eye area, wound healing, skin elasticity and hydration improvement, enhancement of cellulite, some dermatitis, and nails fragility. Large-scale and methodologically more robust studies are still needed to consider the use of oral collagen as an effective adjuvant treatment to different dermatological conditions.
Keywords: Collagen; Skin; Dietary supplements
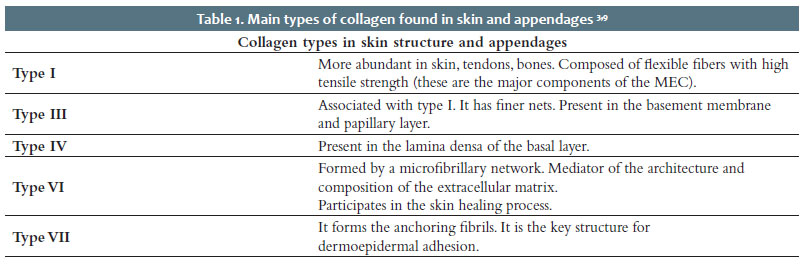
Collagen represents a family of 28 different proteins, which make up about 30% of the total mass of all proteins in the human body. It plays an essential role in the structure of various tissues such as skin and bones, providing rigidity, flexibility, traction, and integrity1,2 (Table 1).
The dermis is composed of a large extracellular matrix rich in collagen. Dermal collagen represents the most abundant protein in the extracellular matrix and constitutes most of the skin, corresponding to 90% of its dry mass.3
The collagen of the dermal connective tissue is essentially responsible for the skin’s strength and the mechanical and structural integrity.3 The complex fibers, fibrils, microfibrils, and collagen molecules form the collagen fibers. Collagen fibers provide elasticity to the skin and elastic fibers for delivering the tone.4
Over the years, profound changes occur in the dermis and epidermis structure through intrinsic and extrinsic aging processes. Collagen density in the dermis significantly decreases with age, associated with a reduction in dermal thickness. The dermal collagen network becomes increasingly fragmented, presenting shorter and less organized fibers, accumulating degraded collagen fragments, largely caused by an increased expression of matrix metalloproteinases. In parallel, the synthesis of extracellular matrix new components by fibroblasts is slower, preventing an adequate replacement of the degraded matrix. The elastic fibers of the papillary dermis lose their integrity and do not reach the dermal-epidermal junction. This global loss of elasticity and strength leads to sagging and wrinkling of the skin.5
In addition to its structural role in the skin, collagen and its fragments control different cellular functions, including cell differentiation, migration, and synthesis of several proteins.6 There is evidence that collagen plays a role in regulating genes such as Gprc, Krt, and Krtap, which encode structural components of the epidermis and skin appendages, such as hair, hair follicles, and nails.7
Collagen also participates in all stages of the healing process. In the hemostasis stage, platelets aggregate around the collagen exposed by the lesion and then secrete factors that stimulate the coagulation cascade. During the inflammation phase, inflammatory cells that have migrated to the lesion site secrete proteolytic enzymes. The action of proteolytic enzymes on the extracellular matrix constituents (mainly collagen) originates several peptides, which have a chemotactic effect for the recruitment of other defense cells, such as neutrophils and macrophages.8 When activated, these cells secrete TNF-alfa and IL-1beta, which directly influence collagen deposition in the wound, stimulating its synthesis via fibroblasts and tissue inhibitors of metalloproteinases. The collagen synthesis products also act by stimulating fibroblasts and keratinocytes proliferation, thus promoting re-epithelialization and angiogenesis.6
A triple helix of parallel polypeptides forms the primary collagen molecular structure (protein), where each third amino acid residue is a glycine (GLY). It results in X-Y-GLY, where X and Y are often proline (PRO) and 4-hydroxyproline (HYP - a subunit unique to collagen), respectively, forming PRO-HYP-GLY, the most common triple chain found in collagen. The triple helix structure is characteristic of collagens.7
The collagen turnover rate in adult humans is vastly low. Intracellular degradation is more linked to physiological processes, while extracellular degradation is more connected to pathological processes.9
Collagen molecules have a certain resistance to proteolytic actions due to their helical structure; however, there are proteolytic enzymes with high collagen specificity. This group of proteolytic enzymes is the metalloproteinases (MMPs), with 23 known types. Most of them are produced and secreted as inactive proenzymes.9
The MMPs responsible for fibrillar collagen degradation are MMP-1 (collagenase 1); MMP-2 (gelatinase A); MMP-8 (collagenase 2); MMP-12 (collagenase 3); MT1-MMP; and MT3M. MMP-3, MMP-10, and MP (membrane-associated matrix metalloproteinases) are responsible for degrading type 3 collagen.9
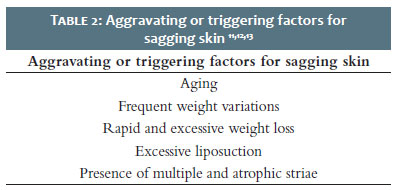
Aging is a biological process that leads to gradual changes in tissue function and structure. Intrinsic and extrinsic factors directly influence this process, which we currently call exposome. The exposome is based on internal factors (physiology, age, body morphology, genome), general external factors (socioeconomic and sociodemographic condition), and specific external factors (diet, environmental and occupational exposures, and lifestyle, among others)10 (Table 2).
These factors influence the intracellular pathways that regulate collagen homeostasis. Time and ultraviolet radiation in dermal fibroblasts lead to increased MMP activity, resulting in collagen degradation and decreased synthesis. In addition to collagen production, biological processes such as cell migration and proliferation, and neoangiogenesis decrease over the years. With time, the action of oxidative stress, and the formation of free radicals, there is intensification in the activity of MMPs and cytokines, resulting in an increase in collagen breakdown and a decrease in its synthesis. Clinically, this process can be seen as skin flaccidity.10
The main histological changes in sagging skin are the reduction in the number of collagen fibers and their fragmentation and disorganization. Elastic fibers also undergo degradation, with loss of the regular morphological pattern (fibrillary).11,12,13
There are some methods available for skin collagen assessment, often used in studies and clinical research. These are direct assessment methods (such as Cutometer, Ballistometer, SkinFibrometer) and indirect assessment (Dermascan and Ultrascan).
Direct methods assess firmness, skin relaxation after traction (return to the original state), and skin elastic properties after suction. Indirect methods consist of high-frequency ultrasound with the ability to measure the thickness of the dermis and objectively assess changes in the dermis using ultrasound markers.14-18
Oral collagen supplementation in Dermatology remains a controversial topic due to the lack of regulatory control of the quality and quantity of ingredients in the supplement market, as well as the scarcity of scientific articles on the topic. However, the interest of researchers in this subject has been growing over the years.19
Gelatin, hydrolyzed collagen, and bioactive collagen peptides are used for oral supplementation. Collagen can be extracted from connective tissue in different ways: when denatured by heat, collagen forms gelatin. After new enzymatic hydrolysis, hydrolyzed collagen (HC) is produced, composed of peptides of different lengths. HC has a lower molecular weight than gelatin, is more water-soluble, and does not harden in room air: thus, it can be formulated into liquids for oral consumption. This low molecular weight protein has been widely used because of its good biocompatibility, excellent degradability, and poor antigenicity.20 HC can be re-hydrolyzed to bioactive collagen peptides, including dipeptides and tripeptides, which are resistant to hydrolysis by peptidases and systemic hydrolytic enzymes.19
Hydrolyzed collagen can cross the intestinal barrier and reach blood circulation. These peptides are digested, absorbed, and transported to the systemic circulation as peptides in the small intestine.20 Bioavailability studies in humans demonstrate that dipeptides and tripeptides can be detected in the systemic circulation after oral ingestion. Also, in vitro studies have shown that oral ingestion of HC induces collagenase at the level of mRNA transcription and protein translation, promoting antioxidant activity and producing firmer collagen fibrils. Animal model studies conducted with rats demonstrate that tri (Gly-Pro-Hyp) and dipeptides (Pro-Hyp) reach the skin rapidly after oral ingestion, occurring after 10 minutes, and they are retained in the tissue for up to two weeks.19,20
A placebo-controlled animal model study by Zague et al. demonstrated a significant increase in collagen types I and IV in the skin’s extracellular matrix and a decrease in metalloproteinase 2.21 The antioxidant properties of HC are mainly due to the presence of hydrophobic amino acids in the peptide; however, its mechanism of action is not yet fully elucidated.20
To date, the literature has identified more than 30 peptides in the blood after ingestion of hydrolyzed collagen, mainly Pro-Hyp. These peptides can exert several functions in the body, such as fibroblasts proliferation.20 However, specific peptide sequences have demonstrated more particular beneficial effects.1,2 When the collagen protein is hydrolyzed through a specific process with known enzymes, cleavages occur at certain points leading to the formation of bioactive peptides with functionality in the skin tissue.22
The literature suggests three different possible mechanisms by which oral collagen ingestion may benefit the skin: (a) collagen fragments may be precursors for collagen synthesis in the skin; (b) collagen fragments can stimulate the production of collagen and proteoglycans in the skin; and (c) collagen and its fragments can increase skin turnover by inducing regulatory T cells (Tregs) and M2 macrophages.22
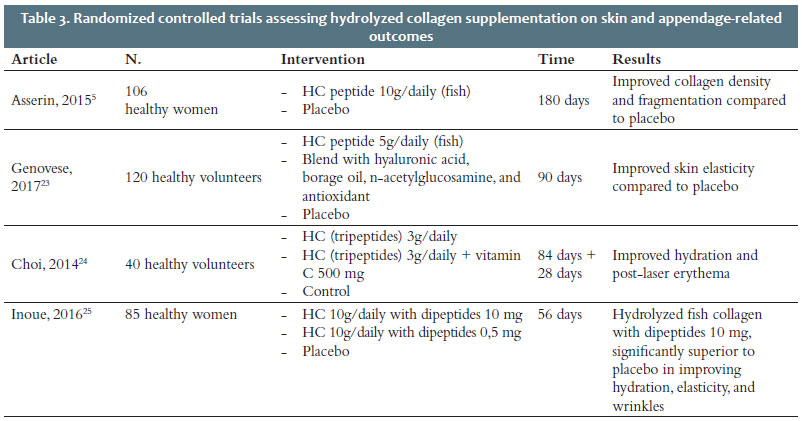
In a recently published systematic review, were analyzed randomized controlled trials using oral collagen and its effectiveness in improving skin quality, anti-aging benefits, and potential use in dermatological pathologies. The review included 11 studies were, totaling 805 patients, 699 women, 17 men, and 89 unspecified participants. The mean duration of the studies was 69.2 weeks (approximately 17 months). There were reports of eight studies conducted with hydrolyzed collagen, two studies conducted with tripeptides, and one study conducted with collagen dipeptides.23 The results demonstrate that the use of collagen supplementation is promising for the short and long term in wound healing and skin aging. Collagen supplements improved collagen elasticity, hydration, and density (in the methods assessed)19 (Table 3 and 4).
HC has been used to treat several dermatological conditions, including pressure ulcers, xerosis, and skin aging. A marked improvement in skin elasticity was observed with the use of HC. A study of 106 Caucasian women aged 40-65 years (for 12 weeks) showed that oral intake of 10g/day of hydrolyzed fish collagen led to an 8.83% increase in collagen density (versus 0% with placebo, p<0.01), and 31.2% reduction in collagen fragmentation (versus increased fragmentation with placebo, p<0.05).5 The same authors evaluated 33 women with low skin hydration who received fish collagen peptides 10g/day, porcine collagen peptides 10g/day, and placebo for 56 days. They found that fish and porcine collagen led to a 12% and 28% increase, respectively, in skin hydration compared to the placebo.5
Another study assessed, for 90 days, 120 patients, aged between 40-60 years, who consumed a nutricosmetic containing HC 5g, hyaluronic acid, borage oil, n-acetylglucosamine, and antioxidants. The participants showed a significant increase in skin elasticity (7.5% compared to baseline versus placebo, p<0.01).24,25
Two studies analyzed 40 patients (32 women and eight men) using collagen tripeptides 3g/day for four or 12 weeks. Eight patients (33-44 years old) underwent an 1150 nm fractional non-ablative laser procedure. Participants who received supplementation with bioactive peptides had a significant improvement in skin hydration on the third day (p<0.05%) and in skin elasticity on the 14th day (p<0.05%) compared to the group that received placebo. The use of collagen post-procedure also showed an improvement in post-laser erythema.26
There was a report of only one study with collagen dipeptides. This study assessed, for eight weeks, 85 Chinese women aged 25-57. Consumption of collagen dipeptide supplements improved skin hydration and elasticity, as well as decreased the number, depth, and roughness of wrinkles, as measured by VisioFace (Courage-Khazaka, Germany), compared to participants who received placebo (p<0.05%).27
Preliminary results regarding the use of HC in the treatment of xerosis, aging, cellulitis, and pressure ulcers are promising. Effects include improved hydration, skin elasticity, dermal collagen density, procollagen type 1 and elastin levels, and also decreased collagen fragmentation, transepidermal water loss (TEWL), and expression of MMPs 1 and 12.19
The use of collagen can benefit other issues not related to aesthetics. A good indication for its use is allergic contact dermatitis and atopic dermatitis (AD).
Atopic dermatitis is a disease that presents an alteration in the skin barrier function. Although no placebo was used, a 12-week study of AD patients (13 participants in total: six receiving tripeptides 3.9 g and seven receiving common collagen 3.9g) demonstrated a deficit in the production of chemokines expressed by macrophages and stromal thymic lymphopoietin. After 12 weeks, lesions, severity index (SCORAD), qualitative hydration, PTA, and pruritus improved significantly in the group that received tripeptides. The different responses to different types of collagen in AD may occur analogously in other diseases with an altered barrier function.19
Although it is generally believed that collagen peptides are hydrolyzed to amino acids in the gastrointestinal tract before being absorbed into the bloodstream, considerable evidence exists to show that peptides can be absorbed partially intact. Several studies on bioavailability in animals and humans with collagen peptides administered orally demonstrate that they are absorbed as free amino acids and also as peptides.26 The bioavailability of collagen peptides is 99%, that is, in the ingestion of 2.5 grams of bioactive peptides, 2.25 grams are absorbed.29
Ingested collagen peptides can cross the intestinal barrier and, through the integrin membrane receptor, fibroblasts signal stimulating the biosynthesis of type I collagen, proteoglycans, and elastin in the dermal extracellular matrix.28 Within the target connective tissue, the peptides can exert their action on the skin’s metabolic processes.28
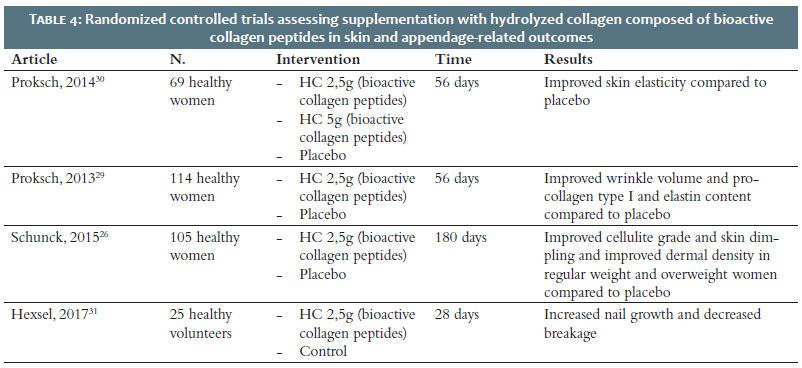
A randomized, double-blind, placebo-controlled study assessed the effectiveness of hydrolyzed collagen composed of bioactive collagen peptides on skin biophysical parameters related to skin aging. The research randomized 69 women aged 35-55 years to receive 2.5 g or 5 g of hydrolyzed collagen composed of specific peptides or a placebo once daily for eight weeks. The authors objectively measured skin elasticity, hydration, roughness, and transepidermal water loss before the first administration of the product (t0) and after four (t1) and eight (t2) weeks of regular ingestion. The study also assessed skin elasticity four weeks after the last product intake. The results showed that both doses of hydrolyzed collagen improved the parameters evaluated compared to placebo. In the assessment of skin elasticity through cutometry, there was a statistically significant improvement in both doses compared to placebo. After four weeks of the last ingestion of the peptides, significantly superior skin elasticity was demonstrated in the subgroup of elderly patients, with about 98% of positive effect after the ingestion of hydrolyzed collagen. The assessment of skin hydration by corneometry showed an increase of 11-14% in hydration in women over 50 years of age. Regarding transepidermal water loss, there was a 6-7% reduction in water evaporation in women over 50 years old. No differences were demonstrated regarding skin roughness. The results show that oral ingestion of bioactive collagen peptides promotes a significant difference in skin elasticity. Also, the effects are long-lasting, especially in women over 50.30,31
A randomized, double-blind, placebo-controlled study evaluated the efficacy of taking 5 g of hydrolyzed collagen orally in 36 postmenopausal women. The research assessed participants for skin elasticity of the cheeks using cutometry at baseline, two and four weeks after randomization, and four weeks after treatment discontinuation. The skin elasticity of participants who received HC increased compared to placebo (p=0.006 and 0.03, respectively). After four weeks of treatment discontinuation (week eight), the skin elasticity of the cheeks remained superior in the HC group compared to the placebo group (p=0.01 and 0.004, respectively).32 More recently, Miyanaga et al. (2021) conducted a double-blind, randomized, controlled trial to evaluate supplementation of 1 g to 5 g collagen peptides versus placebo regarding skin quality. The study assessed skin water content, transepidermal water loss (TEWL), skin elasticity, and thickness before treatment and after four, eight, and 12 weeks in 99 healthy patients. The research also quantified the level of natural hydration factor before treatment and after 12 weeks. The results demonstrated that oral ingestion of collagen peptides increased water content in the stratum corneum and epidermis and decreased transepidermal water loss. The study also showed an increased level of natural hydration factor in the stratum corneum. Skin elasticity and skin thickness remained unchanged.33
Regarding wrinkles, a double-blind, randomized, placebo-controlled study evaluated 114 women aged 35-55 years who were randomized to receive 2.5 g of bioactive collagen peptides or placebo once daily for eight weeks. The study objectively assessed the wrinkles in all participants before the start of treatment, after four and eight weeks of treatment, and four weeks after the last ingestion. The authors established a subgroup to perform suction blister biopsies, analyzing pro-collagen I, elastin, and fibrillin at the beginning of treatment and after eight weeks. The ingestion of the bioactive collagen peptides promoted a statistically significant reduction (7.2%) in the volume of wrinkles in the eye region compared to placebo after four weeks of treatment. The effect was even more pronounced after eight weeks of treatment, with an average reduction of 20.1% compared to placebo (p<0.01). Four weeks after the last ingestion of the product, the group that received the bioactive collagen peptides continued to demonstrate a significant 11.5% reduction in the volume of wrinkles in the eye region. After eight weeks of administration, a significantly higher amount of procollagen type I (65%) and elastin (18%) content was detected in the group treated with bioactive peptides compared to the group receiving placebo. For fibrillin, an increase of 6% was detected.32
Bioactive collagen peptides also demonstrated a relationship with clinical improvement in the treatment of moderate cellulite, in a study conducted with 105 healthy women aged 24-50 years, skin phototypes 1-3. Supplementation was performed with 2.5g/day for 180 days, resulting in a statistically significant decrease in the degree of cellulite and skin dimpling (p<0.05) in normal-weight women. The data revealed a 5.3% reduction in cellulite score after three months and a 9% reduction after six months compared to placebo. Concerning skin dimpling, there was a significant 11% reduction in normal-weight women. Also, dermal density improved significantly (p<0.05) compared to placebo. The study also observed the effectiveness of the peptides in overweight women, although the impact was less pronounced compared to normal-weight women.28
An open-label study assessed the effectiveness of collagen peptides in 25 patients with brittle nail syndrome. Patients received bioactive collagen peptides 2.5 g once daily for 24 weeks, followed by a four-week treatment-free period. Bioactive collagen peptides promoted a 12% increase in the nail growth rate and a 42% reduction in the broken nails frequency. Additionally, 64% of participants achieved clinical improvement in brittle nails, and 88% showed improvement within four weeks of treatment. The study demonstrates that daily intake of bioactive collagen peptides increases nail growth and improves brittle nail syndrome, with a notable reduction in the frequency of broken nails.33
Animal studies indicate a positive effect of the oral collagen peptides on epithelialization and reduced healing time, improving angiogenesis. In this sense, an observational study assessed the impact of bioactive collagen peptides on wound healing. The study followed up 22 patients with postsurgical wounds (Group A - 12 receiving the peptides and 10 receiving the placebo) and 20 patients with unhealed wounds (Group B - 10 receiving the peptides and 10 receiving the placebo). In both groups, patients who received bioactive collagen peptides presented significantly better healing than patients treated with placebo, who had poor or suboptimal outcomes in most cases. The results of this investigation demonstrate a positive impact of the use of collagen on wound healing, even in cases where normal healing is expected to obtain aesthetic results. The positive effect on the skin is mainly due to the direct impact on the dermal extracellular matrix turnover, with a significant increase in collagen and elastin synthesis.34
There is growing evidence showing different benefits of oral collagen peptide supplementation for the skin. To date, the available studies are heterogeneous and present methodological limitations, which makes the results often not comparable with each other, so the evidence on collagen supplementation remains controversial.
The response to oral collagen depends on several factors. The age of the patient can have a direct influence on the results. Patients over 50 years old show a better improvement in elasticity than young patients since younger patients have a higher basal elasticity and are expected to obtain a milder response.19
Other factors such as gender, ethnicity, skin type, lifestyle, comorbidities, and the patient’s skin condition may also play a role. Thus, further studies are needed to assess the efficacy in different patient niches and determine the most adequate response time.
The appropriate dose remains undefined. High doses of oral collagen (15 g 3x/day) have shown improvement in healing processes, but doses of 2.5 g of bioactive peptides have already been shown to be effective in improving periorbital wrinkles.19 Most studies were conducted with healthy women, which leads to a concern regarding the effectiveness of collagen use in patients with comorbidities.
It is noteworthy that patients who seek the use of oral collagen-based supplements, in general, have high expectations regarding their results, most of the time due to a lack of adequate information.
The results reported in the studies presented are highly dependent on measurement tools (transepidermal loss, skin hydration, elasticity, collagen density, etc.). However, patient satisfaction is also an important indicator of improved quality of life, and participants included in the studies mentioned reported positive feedback after using oral collagen.
The evidence available to date indicates that oral collagen supplementation may have an adjunctive role in the treatment of the following conditions:
- Improved skin elasticity;
- Wrinkle reduction in the eye area;
- Wound healing (including pressure ulcers);
- Cellulite improvement;Improved skin hydration;
- Improved atopic dermatitis and allergic contact dermatitis;
- Improved brittleness and increased nail growth.
Studies have also shown that, in healthy patients, the use of oral collagen is safe even at higher doses, with no reports of adverse events related to its use. Patient satisfaction with treatment has also shown good results in available studies.
However, the effectiveness of oral collagen remains controversial due to the lack of large-scale controlled studies with recognized methodology. Studies that robustly prove the superiority of collagen ingestion versus the ingestion of other sources of proteins and amino acids are recommended, as well as research proving that collagen ingested orally can be used preferentially to improve the dermis.
There is also a need for additional studies that elucidate the role of collagen in barrier function and diseases such as atopic dermatitis, thus determining the most appropriate dose for each condition, and defining the ideal patient based on age, gender, skin type, ethnicity, and presence of comorbidities.
Comparing the results of current literature with those available a few years ago, it is possible to conclude that oral collagen has shown increasing evidence of its effectiveness in the adjuvant treatment of different conditions for patients in the dermatological office. Given the high demand and good acceptance, prescribers need to be aware of the available evidence to advise patients on the expected benefits.
Francine Papaiordanou: 0000-0003-0138-8361
Study design and planning; preparation and writing of the manuscript critical literature review.
Gabriela Pacheco de-Oliveira: 0000-0001-5464-3501
Preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review
Doris Hexsel: 0000-0002-0615-9026
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; critical revision of the manuscript.
Antonio Carlos Amedeo Vattimo: 0000-0002-1976-7434
Approval of the final version of the manuscript; critical revision of the manuscript.
1. Gelse K, Pöschl E, Aigner T. Collagens - structure, function and biosynthesis. Adv Drug Deliv Rev. 2003;55(12):1531-46.
2. Ricard-Blum S. The collagen family. Cold Spring Harb Perspect Biol. 2011;3(1):a004978.
3. Quan T, Fisher GJ. Role of age-associated alterations of the dermal extracellular matrix microenvironment in human skin aging: a mini-review. Gerontology. 2015;61(5):427-34.
4. Tang M, Li T, Gandhi NS, Burrage K, Gu Y. Heterogeneous nanomechanical properties of type I collagen in longitudinal direction. Biomech Model Mechanobiol. 2017;16(3):1023-33.
5. Asserin J, Lati E, Shioya T, Prawitt J. The effect of oral collagen peptide supplementation on skin moisture and the dermal collagen network: evidence from an ex vivo model and randomized, placebo-controlled clinical trials. J Cosmet Dermatol. 2015;14(4):291-301.
6. Brett D. A review of collagen and collagen-based wound dressings. Wounds. 2008;20(12):347-56.
7. Hexsel D, Zague V, Schunck M, Siega C, Camozzato FO, Oesser S. Oral supplementation with specific bioactive collagen peptides improves nail growth and reduces symptoms of brittle nails. J Cosmet Dermatol. 2017;16(4):520-6.
8. Nedelec B, Forget NJ, Hurtubise T, Cimino S, Muszka F, Legault et al. Skin characteristics: normative data for elasticity, erythema, melanin, and thickness at 16 different anatomical locations. Skin Res Technol. 2016;22(3):263-75.
9. Sprangers S, Everts V. Molecular pathways of cell-mediated degradation of fibrillar collagen. Matrix Biol. 2019;75-76:190-200.
10. Olympio KPK, Salles FJ, Ferreira APSS, Pereira EC, Oliveira AS, Leroux IN, et al. O expossoma humano desvendando o impacto do ambiente sobre a saúde: promessa ou realidade? Rev Saúde Pública. 2019;53. Epub jan 18.
11. Shin JW, Kwon SH, Choi JY, Na JI, Huh CH, Choi HR, et al. Molecular mechanisms of dermal aging and antiaging approaches. Int J Mol Sci. 2019;20(9):2126.
12. Ortolan MCAB, Biondo-Simões MLP, Baroni ERV, Auersvald A, Auersvald LA, Netto MRM, et al. Influência do envelhecimento na qualidade da pele de mulheres brancas: o papel do colágeno, da densidade de material elástico e da vascularização. Rev Bras Cir Plást. 2013;28(1):41-8.
13. Wang H, Shyr T, Fevola MJ, Cula GO, Stamatas GN. Age-related morphological changes of the dermal matrix in human skin documented in vivo by multiphoton microscopy. J Biomed Opt. 2018;23(3):1-4.
14. Nedelec B, Forget NJ, Hurtubise T, Cimino S, Muszka F, Legault A, et al. Skin characteristics: normative data for elasticity, erythema, melanin, and thickness at 16 different anatomical locations. Skin Res Technol. 2016;22(3):263-75.
15. Bonaparte JP, Ellis D, Chung J. The effect of probe to skin contact force on Cutometer MPA 580 measurements. J Med Eng Technol. 2013;37(3):208-12.
16. Kim MA, Kim EJ, Lee HK. Use of SkinFibrometer® to measure skin elasticity and its correlation with Cutometer® and DUB® Skinscanner. Skin Res Technol. 2018;24(3):466-71.
17. Woo MS, Moon KJ, Jung HY, Park SR, Moon TK, Kim NS, et al. Comparison of skin elasticity test results from the Ballistometer(®) and Cutometer(®). Skin Res Technol. 2014;20(4):422-8.
18. Crisan M, Badea R, Cattani C, Crisan D. Senescence: imagistic noninvasive assessment of skin aging and anti-aging therapies. In: Nagata T, editor. Senescence. Rijeka: Intech; 2012. p. 773–96.
19. Choi FD, Sung CT, Juhasz ML, Mesinkovsk NA. Oral collagen supplementation: a systematic review of dermatological applications. J Drugs Dermatol. 2019;18(1):9-16.
20. Aguirre-Cruz G, León-López A, Cruz-Gómez V, Jiménez-Alvarado R, Aguirre-Álvarez G. Collagen hydrolysates for skin protection: oral administration and topical formulation. Antioxidants (Basel). 2020;9(2):181.
21. Zague V, de Freitas V, da Costa Rosa M, de Castro GÁ, Jaeger RG, Machado-Santelli GM. Collagen hydrolysate intake increases skin collagen expression and suppresses matrix metalloproteinase 2 activity. J Med Food. 2011;14(6):618-24.
22. Barati M, Jabbari M, Navekar R, Farahmand F, Zeinalian R, Salehi-Sahlabadi A, et al. Collagen supplementation for skin health: a mechanistic systematic review. J Cosmet Dermatol. 2020;19(11):2820-29.
23. Gelita do Brasil LTDA. Peptídeos de Colágeno. Available from: https://www.gelita.com/pt-pt/peptideos-de-colageno.
24. Pawlaczyk M, Lelonkiewicz M, Wiezxorowski M. Age-dependent biomechanical properties of the skin. Postepy Dermatol Alergol. 2013;30(5):302-06.
25. Genovese L, Corbo A, Sibilla S. An insight into the changes in skin texture and properties following dietary intervention with a nutricosmeceutical containing a blend of collagen bioactive peptides and antioxidants. Skin Pharmacol Physiol. 2017;30(3):146-58.
26. Choi SY, Ko EJ, Lee YH, Kim BG, Shin HJ, Seo DB, et al. Effects of collagen tripeptide supplement on skin properties: a prospective, randomized, controlled study. J Cosmet Laser Ther. 2014;16(3):132-7.
27. Inoue N, Sugihara F, Wang X. Ingestion of bioactive collagen hydrolysates enhance facial skin moisture and elasticity and reduce facial ageing signs in a randomized double-blind placebo-controlled clinical study. J Sci Food Agric. 2016;96(12):4077-81.
28. Schunck M, Zague V, Oesser S, Proksch E. Dietary supplementation with specific collagen peptides has a body mass index-dependent beneficial effect on cellulite morphology. J Med Food. 2015;18(12):1340-8.
29. Ziegler FF, Sgarbieri VC. Caracterização químico-nutricional de um isolado protéico de soro de leite, um hidrolisado de colágeno bovino e misturas dos dois produtos. Rev Nutr. 2009;22(1):61-70.
30. Siebert HC, Burg-Roderfeld M, Eckert T, Stötzel S, Kirch U, Diercks T, et al. Interaction of the α2A domain of integrin with small collagen fragments. Protein Cell. 2010;1(4):393-405.
31. Proksch E, Segger D, Degwert J, Schunck M, Zague V, Oesser S. Oral supplementation of specific collagen peptides has beneficial effects on human skin physiology: a double-blind, placebo-controlled study. Skin Pharmacol Physiol. 2014;27(1):47-55.
32. Sangsuwan W, Asawanonda P. Four-weeks daily intake of oral collagen hydrolysate results in improved skin elasticity, especially in sun-exposed areas: a randomized, double-blind, placebo-controlled trial. J Dermatolog Treat. 2020;9:1-6.
33. Miyanaga M, Uchiyama T, Motoyama A, Ochiai N, Ueda O, Ogo M. Oral supplementation of collagen peptides improves skin hydration by increasing the natural moisturizing factor content in the stratum corneum: a randomized, double-blind, placebo-controlled clinical trial. Skin Pharmacol Physiol. 2021;34(3):115-27.
34. Proksch E, Schunck M, Zague V, Segger D, Degwert J, Oesser S. Oral intake of specific bioactive collagen peptides reduces skin wrinkles and increases dermal matrix synthesis. Skin Pharmacol Physiol. 2014;27(3):113-9.
35. Hexsel D, Zague V, Schunck M, Siega C, Camozzato FO, Oesser S. Oral supplementation with specific bioactive collagen peptides improves nail growth and reduces symptoms of brittle nails. J Cosmet Dermatol. 2017;16(4):520-6.
36. Knefeli HC, Duran B. Improved wound healing after oral application of specific bioactive collagen peptides. Nutrafoods. 2017;16:9-12.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}