


Zuzanna Swierczewska; Wioletta Baranska-Rybak
Financial support: None
Conflict of interest: None
Submission on: 09/11/2021
Approved on: 22/11/2021
How to cite this article: Swierczewska Z, Baranska-Rybak W. Attagenus larva in the sinus cavity in a patient with complications after the use of hyaluronic acid filler. Surg Cosmet Dermatol. 2022;13:e20220109
A wide range of dermal fillers is now available for use in the beauty industry. We present a case of a 33-year-old woman with complications after hyaluronic acid injection by a non-medical practitioner. Two weeks after the injection, bilateral sinus pain, fever, and burning sensation occurred in the cheek area. She underwent a detailed diagnosis revealing Attagenus larva in the paranasal sinus. Despite treatment, the symptoms remained. Thus, hyaluronidase was administered in the infraorbital area, obtaining a full remission.
Keywords: Hyaluronic acid; Nasal cavity; Dermatology; Larva; Dermal fillers.
Dermal fillers injection is one of the most common procedures in aesthetic medicine practice. According to Aesthetic Plastic Surgery Statistics from 2020, it is among the top two most popular non-surgical procedures, right after injection of neurotoxins.
Although facial filler treatments with hyaluronic acid (HA) are reasoned as minimally invasive, they are not free from complications. The most frequent non-vascular adverse events of hyaluronic acid administration include swelling, granulomas, and infections. However, ischemia, necrosis, and blindness are considered the most common vascular complications. Injections with hyaluronidase are indicated as the treatment of choice in dealing with complications after the use of HA fillers.1
We present a case of a patient with nasal infestation with Attagenus larva discovered during the diagnosis.
A 33-year-old woman was admitted in March 2021 due to exacerbation of persistent pain in the right infraorbital area starting four days before the hospitalization. At admission, the patient presented no concomitant edema, but a periodic burning sensation. Physical examination revealed soft skin with even consistency and no inflammation and no tissue resistance.
Detailed anamnesis revealed a history of rheumatoid arthritis, in remission for four years, as well as hypothyroidism. Also, the patient reported two episodes of acute urticaria of unknown etiology requiring ER intervention several years ago. Numerous cosmetic procedures were performed in the past.
In August 2020, a beautician performed a procedure to fill the cheeks and the tear trough with hyaluronic acid of unknown origin, 1 ml per side. Two weeks after the injection, the patient reported bilateral sinus pain, fever, and burning sensation in the cheek area. Therefore, amoxicillin with clavulanic acid was administered but without effect.
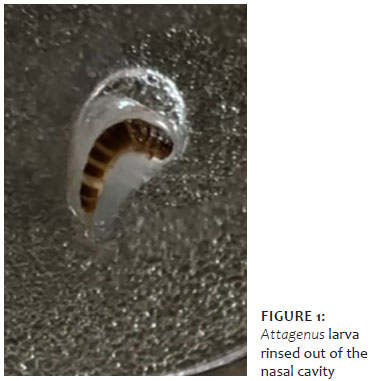
Due to lack of clinical improvement, a month later clindamycin 600 mg twice daily was included for a week. Also, nasal irrigation was performed by the ENT specialist, rinsing out the larva that was identified as Attagenus larva (Figure 1) in The Institute of Maritime and Tropical Medicine in Gdynia, Poland.
The patient was assessed with computed tomography (CT) scan twice over five months. The first CT scan revealed no visible foreign body in the sinus cavity, circular thickening of the mucous membranes in the maxillary sinuses suggestive of an inflammatory process, bilateral obstruction of the maxillary sinus ostia, and deviated nasal septum to the right side. The second CT scan showed only trace mucosal changes in the right maxillary sinus and no inflammation in the remaining paranasal sinuses.
During the appointment in March 2021, we implemented methylprednisolone 16 mg/day, azithromycin 500mg/day, and bilastine 20 mg twice daily. At the three-week follow-up visit, the patient admitted pain reduction; nonetheless, paresthesia was still inherent. Given these facts, hyaluronidase in the total dose of 30 IU was administered in the area of the right tear trough. Methylprednisolone was reduced to 12 mg daily.
Seven days after the hyaluronidase administration, we observed full remission of pain and paresthesia. Further reduction of methylprednisolone was applied, this time to 4 mg every seven days.
Due to the growing popularity of aesthetic medicine and its profitability, many other practitioners with minimal or no training and medical background have ventured into the aesthetic industry.2 It is estimated that complications after treatments in aesthetic medicine occur relatively more often in patients treated by practitioners from outside the medical area.2,3,4 Lack of appropriate professional qualification, incorrect injection technique, and absence of asepsis may lead to serious complications.
Regarding the facial aesthetic procedures, collecting a profound history of allergies, systemic diseases, current treatment, and previous procedures is mandatory.5 Filler treatments are contraindicated in active autoimmune diseases such as rheumatoid arthritis, systemic lupus erythematosus, and Hashimoto’s disease. Our patient report is an example of how dermal filler treatments may be contraindicated, particularly due to a history of rheumatoid arthritis, and should undoubtedly be consulted with an experienced physician. Thus, we want to emphasize the necessity to perform aesthetic medicine treatments by trained doctors. Complementary measures by law enforcement and the communities themselves may help decrease the supply of illegal cosmetic procedures.3,4
Direct trauma to the nerve, straight injection of filler into the nerve, or product compression can emerge into unintentional nerve injury, an uncommon complication of dermal filler procedures. Nerve injury is divided into reversible or permanent. The most frequent localization of paresthesia and anesthesia is the infraorbital nerve.6 Presented patient’s main symptoms, pain and paresthesia, must probably have resulted from compression of the infraorbital nerve caused by the dermal filler. Complete reduction of symptoms after the hyaluronidase administration supports this hypothesis.
Hyaluronidase is an enzyme that breaks down hyaluronic acid, and the Food and Drug Administration (FDA) has approved its off-label use in cosmetic medicine.1 With the increasing popularity of hyaluronic acid fillers, hyaluronidase has become an essential tool for correcting complications and unsatisfactory outcomes following filler injection. For this reason, adequate knowledge of hyaluronidase is needed when conducting procedures involving hyaluronic acid filler. No major randomized trials are available on its use in aesthetic medicine, so the only information accessible is focused on a literature review and the authors’ practical recommendations. Since different HA formulations exhibit different susceptibility to degradation after hyaluronidase administration, there are no defined recommendations for hyaluronidase dosage in overcorrection.
The authors have found only a few reports discussing the infestation on the nasal cavity.7,8 Typically, it can occur in tropical and developing countries. Our patient was an accidental Attagenus larva host and probably became infested while on vacation in Masuria, Poland, in August 2020. To our knowledge, this is the first case report of infestation of the sinus cavity with Attagenus larva in humans. In conclusion, an infestation of the nasal cavity is a rare occurrence that often causes a mild self-limited illness. Nonetheless, it can pose a diagnostic challenge to physicians unaware of this condition. Furthermore, the lack of data on consensus treatment will make managing these cases more challenging.8
Zuzanna Swierczewska 0000-0003-3555-3070
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Wioletta Baranska-Rybak 0000-0002-4018-6706
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical revision of the manuscript.
1. Zegarska B, Ambroziak M, Ornatowska M, Barańska-Rybak W. Management of complications associated with the use of hyaluronic acid fillers. Recommendations of the Aesthetic Dermatology Section of the Polish Dermatological Society. Dermatol Rev/Przegl Dermatol. 2020;107:15–31.
2. Chayangsu O, Wanitphakdeedecha R, Pattanaprichakul P, Hidajat IJ, Evangelista KER, Manuskiatti W. Legal vs. illegal injectable fillers: The adverse effects comparison study. J Cosmet Dermatol. 2020;19(7):1580-6.
3. Brody HJ, Geronemus RG, Farris PK. Beauty versus medicine: the nonphysician practice of dermatologic surgery. Dermatol Surg. 2003;29(4):319-24.
4. Mayer JE, Goldberg DJ. Injuries attributable to cosmetic procedures performed by unlicensed individuals in the United States. J Clin Aesthet Dermatol. 2015;8(10):35-7.
5. Heydenrych I, Kapoor KM, De Boulle K, Goodman G, Swift A, Kumar N, et al. A 10-point plan for avoiding hyaluronic acid dermal filler-related complications during facial aesthetic procedures and algorithms for management. Clin Cosmet Investig Dermatol. 2018;11:603-11.
6. Funt D, Pavicic T. Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Clin Cosmet Investig Dermatol. 2013;6:295-316.
7. Manfrim AM, Cury A, Demeneghi P, Jotz G, Roithmann R. Nasal myiasis: case report and literature review. Int Arch Otorhinolaryngol. 2007;11(1):74-9.
8. Katabi A, Aguirre M, Obeidat Y, Al-Ourani M, Assad S, Zeid F. Nasal myiasis in myasthenic crisis, a case report and literature review. Respir Med Case Rep. 2020;31:101212.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}