


Rogerio Nabor Kondo; Suellen Tormina da Silva; Gabriela Bernardi Maia; Leticia Amstalde Bertoncini
Submitted on:23/09/2021
Approved on: 27/10/2021
Financial support: None
Conflict of interest: None
How to cite this article: Kondo RN, Silva ST, Maia GB, Bertoncini LA. Usefulness of elastic compression bandage on full-thickness skin graft in lower limbs: a series of two cases. Surg Cosmet Dermatol. 2022;14:e20220095
Reconstruction with grafting for defects resulting from the removal of squamous cell carcinoma in the lower limbs is a great challenge for the dermatological surgeon. A very thin skin for the receiving area, the inhomogeneity of the local vascularization and the transient venous insufficiency make it difficult to integration of the grafted skin in these regions. For the success of this type of procedure, some techniques can be used to repair these difficulties, such as an elastic compressive dressing that we use in the first postoperative days of a total skin graft on the foot and leg, with good results
Keywords: Carcinoma squamous cell; Foot; Leg; Graft survival
Squamous cell carcinoma (SCC) is the second most common type of skin cancer.1 When located in the lower limbs, complete excision is usually performed, resulting in a defect that may require a flap or graft for closure. There is a greater preference for reconstructions in this region using a flap rather than a graft to maintain local vascularization.2
In addition to the grafted skin being too thin for the defect area of the lower limbs, the inhomogeneity of the vascularization of the receiving region2 and the transient superficial arterial and venous insufficiency caused by the surgical excision of the site make it challenging to integrate the graft.3
To improve the chances of graft integration in the lower limbs, some technical options, such as negative pressure therapy (NPT), which consists of providing subatmospheric pressure to the wound bed, have been used.4 NPT improves the exudate of venous insufficiency transient and promotes local angiogenesis.
This report aims to demonstrate the use of elastic bandage (EB) over Brown’s dressing to improve comfort and protection for the patient. We report two patients where the autograft technique was used (in the foot and the leg), with good integration, aesthetic, and functional results.
We treated two patients with SCC in the left foot and the right leg:
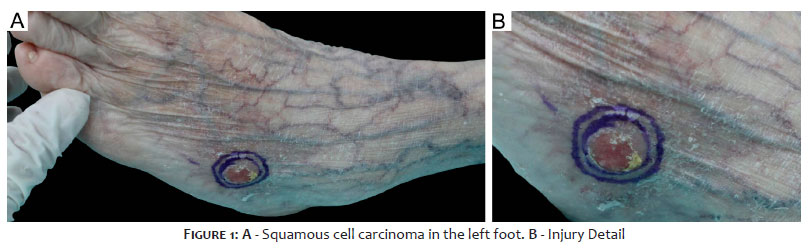
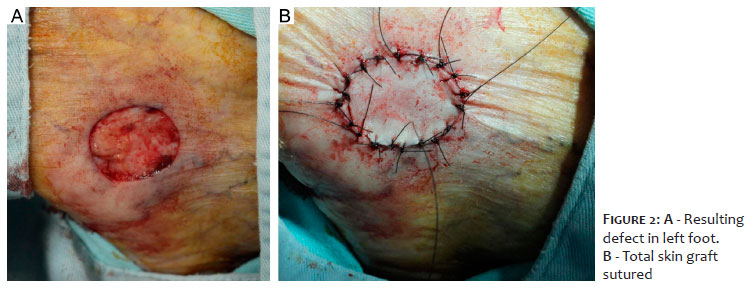
Patient 1: Woman, 78 years old, skin phototype III, from Londrina (PR), with erythematous plaque, 18 mm x 19 mm, on the left foot, compatible with SCC by histopathology. The lesion was excised with 5 mm safety margins, with free margins according to the anatomopathological examination. The resulting defect was 2.9 mm in the longest axis and a graft was chosen (Figures 1, 2, 3, and 4).
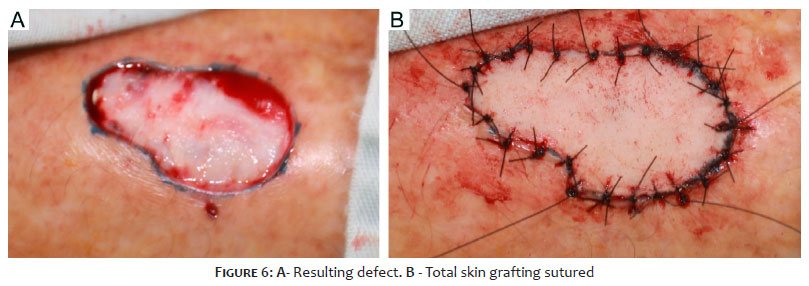
Patient 2: Man, 76 years old, skin phototype III, from Londrina (PR), with erythematous plaque, 29 mm x 15 mm, on the right leg, compatible with in situ SCC by histopathology. The lesion was excised with 5 mm safety margins, with free margins according to the anatomopathological examination. The resulting defect was 39 mm in the longest axis and a graft was chosen (Figures 5, 6, 7 and 8).
a) Patient in horizontal dorsal decubitus;
b) Marking of the lesion using methylene blue or surgical pen with 5 mm margin (Figures 1 and 5)
c) Antisepsis with topical 10% polyvinyl iodine
d) Placement of surgical drapes;
e) Infiltrative anesthesia with 2% lidocaine with vasoconstrictor;
f) Lesion incision using blade 15 and block excision;
g) Hemostasis;
h) Removal of the donor area (full-thickness graft). Patient 1, donor area from the left iliac fossa region. Patient 2, donor area from the inner arm;
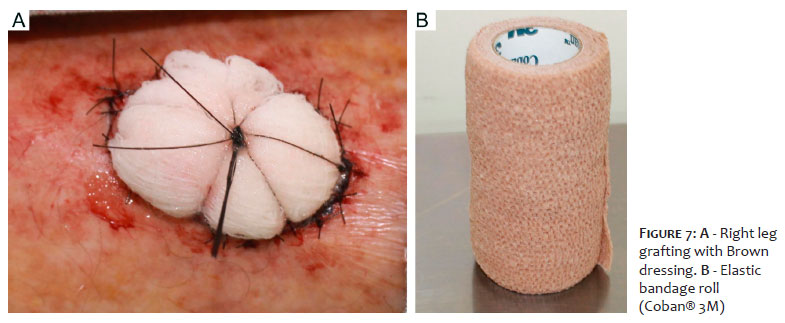
i) Positioning the graft in the receiving area using 4.0 monofilament nylon and cardinal stitches with one of the longest points for fixation of the Brown’s dressing. Between cardinal stitches, simple stitches with 4.0 mononylon (Figures 2, 3, 6 and 7A) were performed;
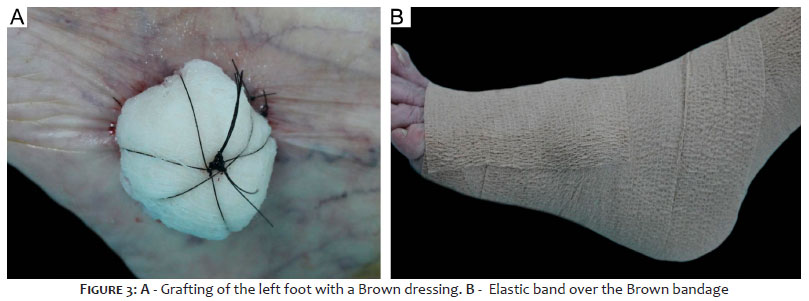
j)Fixation of Brown’s dressing (Figures 3A and 7A);
k) Wrapping with an elastic bandage, two layers Coban® 3M, 35-40 mmHG (Figure 3B, 7B e 8A).
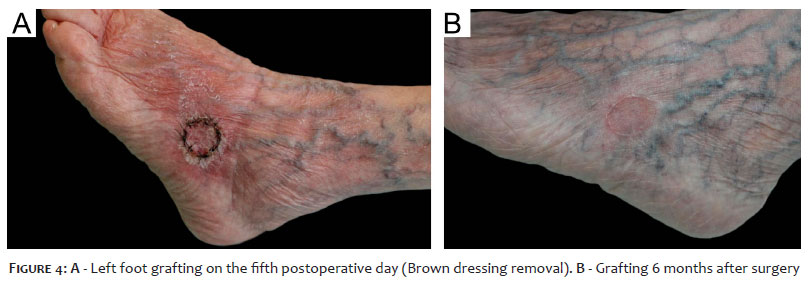
Patient 1: The patient evolved uneventfully in the immediate postoperative period. There was good healing and setting with satisfactory aesthetic results in the late postoperative period. (Figures 4A and 4B)
Patient 2: The patient evolved uneventfully in the postoperative period. There was good healing and attachment, with no epidermolysis or postoperative necrosis. (Figure 8B)
Elastic stockings and compressive dressings are therapies described in the treatment of ulcers due to venous or mixed insufficiencies, and in addition to reducing edema, they improve local perfusion.5Surgical excision of the lower limbs causes a temporary superficial venous and arterial insufficiency,3which, by itself, leads to graft failure.
Devices that provide negative pressure therapy (NPT) can also facilitate graft take. The applied subatmospheric pressure reduces edema and promotes local angiogenesis.4 The problem with NPT is its high cost, making its use unfeasible.
We used a low-cost elastic bandage (EB) (Figure 7B). We kept the Brown’s dressing on for five days and two more days after its removal, totaling seven days after surgery (time for local installation of a true circulation). Adequate limb compression (according to the manufacturer information, 2-layer Coban® 3M provides 35-40mmHg compression for up to seven days) improved venous pumping as a reduction in local edema without impairing vascular neoformation (Figures 4A and 8B).
Patient 1 showed signs of improved venous insufficiency. There was a reduction in varicosities of the foot around the graft while she used EB (Figure 4A). Also, the bandage helped protect Brown’s dressing from external trauma. (Figures 3A and 3B).
Before we implemented the EB technique, the success of lower limb graft survival was poor in our service. We made the graft intending to use it as a biological dressing in cases where the flap was not possible due to the lack of tissue mobility. Epidermolysis and necrosis were visualized when Brown’s dressing was removed.
The patients reported in the present study who used EB over Brown’s dressing had higher stability of the grafted area, with comfort and local protection. There was good integration and good aesthetic and functional results.
The use of EB can be a good option for successful lower limb grafts.
Rogerio Nabor Kondo 0000-0003-1848-3314
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Suellen Tormina da Silva 0000-0002-4687-8332
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Gabriela Bernardi Maia 0000-0002-3730-8207
Approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical revision of the manuscript.
Leticia Amstalde Bertoncini 0000-0002-4687-8332
Approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical revision of the manuscript.
1. Gheno V, Kondo RN, Lena CP. Squamous cell carcinoma of the lower lip: two cases of bilateral reconstruction with Gilles fan flap associated with zetaplasty. Surg Cosmet Dermatol. 2020;12(2):182-6.
2. Haddad Filho D, Siervo JV, Brunhara JN, Silva EL, Vieites L. Alternativas de retalhos cutâneos para lesões dermatológicas na perna. Surg Cosmet Dermatol. 2017;9(2):247-55.
3. Fonseca FP. Doppler ultra-som nas doenças venosas. In: Maffei FHA, Lastória S, Yoshida WB, Rollo HA, editores. Doenças vasculares periféricas. Rio de Janeiro: Medsi; 2002. p. 471-7.
4. Landau AG, Hudson DA, Adams K, Geldenhuys S, Pienaar C. Full- thickness skin grafts: maximizing graft take using negative pressure dressings to prepare the graft bed. Ann Plast Surg. 2008;60(6):661-6.
5. Mosti G, Iabichella ML, Partsch H. Compression therapy in mixed ulcers increases venous output and arterial perfusion. J Vasc Surg. 2012;55(1):122-8.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}