


Jaqueline Barbeito de Vasconcellos; Daniela Alves Pereira Antelo; Rosane Orofino-Costa
Financial support: None
Conflict of interest: None
Submitted on: 10/10/2021
Approved on: 21/03/2022
How to cite this article: Vasconcellos JB, Antelo DAP, Orofino-Costa R. Translation and transcultural validation of a quality of life questionnaire to assess facial cosmetics procedures: a Brazilian Portuguese version. Surg Cosm Dermatol. 2022;14:e20220101
Acknowledgments: The authors thank Dr. Ramsay Alsarraff for his permission to translate and validate his quality of life questionnaire (SROE) into Brazilian Portuguese
BACKGROUND: The increased demand for cosmetic facial treatments is a universal reality, with Brazil being the second country in the world that performs them the most. Quality of life questionnaires can help assess results more objectively and reveal data not yet explored in the scientific literature. For this, the process of translation, adaptation and validation of questionnaires is necessary for the universalization of data.
OBJECTIVE: To translate, adapt and validate a specific questionnaire for the assessment of facial cosmetics procedures into the Portuguese language spoken in Brazil.
METHODS: After choosing the SROE (Skin Rejuvenation Outcome Evaluation) questionnaire, the translation process started. A literal translation was performed, with subsequent synthesis of the versions. After, reverse translation and final validation by a team of experts were carried out. The data obtained were statistically analyzed for validation.
RESULTS: The final version was called "Avaliação dos Resultados de Rejuvenescimento da Pele" (ARRP). The Cronbachs a resulted in values above 0.70, showing good internal consistency. The Intraclass Correlation Coefficient was 0.995 (p<0.001).
CONCLUSIONS: The values obtained validate the ARRP questionnaire, translated into Brazilian language and culture, which aims to evaluate the results and impact on the quality of life of facial cosmetics procedures.
Keywords: Cross-cultural comparison; Patient health questionnaire; Quality of life
Brazil is the second country in the world with the most aesthetic dermatological procedures, according to the most recent data from the International Society of Aesthetic Plastic Surgery (ISAPS, 2019), only after the United States.1 ISAPS statistics for the same year showed that the demand for surgical procedures has been decreasing (-0.6% compared to the previous year), while for non-surgical procedures has been increasing (+12%). An American Society for Dermatologic Surgery research (ASDS, 2019) indicated that the dermatologist is the most sought professional after the five main non-surgical procedures (botulinum toxin, hyaluronic acid filling, laser treatments, intense pulsed light, and peels).
Historically, the desire for facial rejuvenation and beautification procedures has been attributed to psychological disorders and narcissism. However, well-being, quality of life, and social and professional insertion are the main motivations nowadays. Maisel et al. demonstrated, through a multicenter study, that the number of patients who underwent a procedure motivated by internal desires driven by self-confidence was higher than those who did it to please others.3
The expectations and results of these procedures go beyond the clinical analysis of the aesthetic component, considering the patient’s perception, the impact on quality of life (QOL), and their social relationships.4
The international literature, including the World Health Organization (WHO), has been exploring the challenging development of tools to measure an individual’s QOL through questionnaires applied to patients. Tools such as the whoqol-100 and whoqol-bref.5-7 QOL questionnaires can help assess the results of dermatological procedures more objectively and reveal data not yet explored in medical research and scientific literature, thus improving techniques and outcomes in cosmiatry.8
The use of instruments that already exist in other languages to assess outcomes and QOL does not depend on a simple literal translation and application to the patient. Several research groups and experts in QOL measurement have studied the process and indicate that it must follow sequential and specific steps to respect the essential psychometric parameters for this evaluation.6,9
Clinical research in national cosmiatrics lacks instruments that evaluate the repercussion of cosmetic procedures, although there are national and international scientific journals aimed only at publishing these techniques.
This study aims to translate, cross-cultural adapt, and validate a quality of life questionnaire in Brazilian Portuguese to assess cosmetic procedures.
This study was submitted to the Research Ethics Committee (REC) of the Hospital Universitário XXXX, and approved on February 28, 2019, under CAAE 02792818.3.0000.5259, and conducted in the Corrective Dermatology Sector of the same hospital.
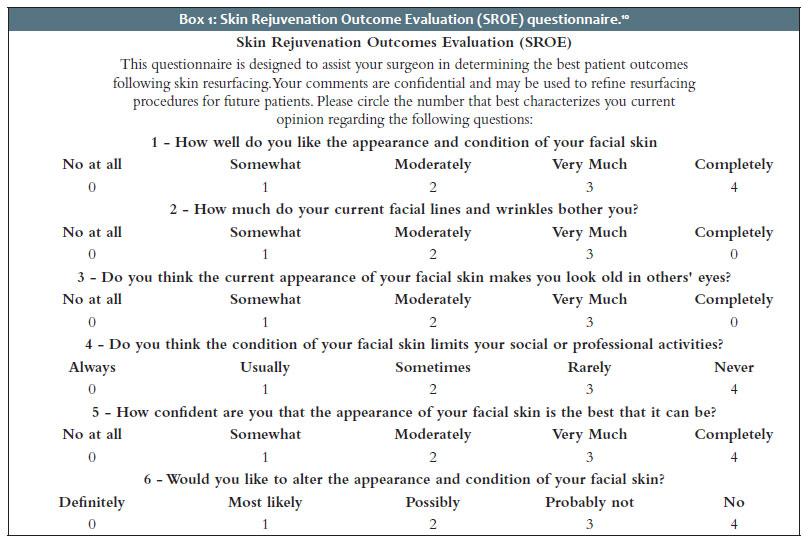
Selection – We selected the Skin Rejuvenation Outcome Evaluation (SROE) questionnaire, which already exists in American English because it is comprehensive, easy to understand, and has a short execution time (Box 1). It was created and validated to assess the results of patients undergoing facial rejuvenation procedures.10,11 Its author, the North American plastic surgeon Ramsay Alsarraff, granted authorization by e-mail for the translation and cultural adaptation into Brazilian Portuguese.
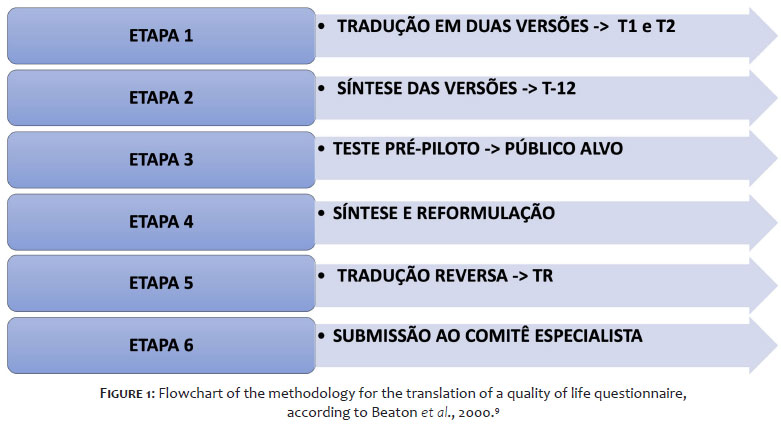
Translation and cultural validation – We conducted the translations and cultural validation through proposed methods already applied in several questionnaires translated and published in Brazilian literature,6,9 according to the flowchart shown in figure 1. Briefly, it consists of six steps: Step 1, translation, literary translation of the questionnaire from English to Portuguese, by translator 1 (T1) and translator 2 (T2), one layperson and one from the health area; Step 2, synthesis, assessment of the T1 and T2 Portuguese versions of the questionnaires by the project author together with the translators of Step 1 to verify divergences and prepare an intermediate consensual version, called T-12; Stage 3, pre-pilot test, application of the intermediate version (T-12) to at least ten patients selected from the target audience, aiming at assessing the clarity of the language - each patient answers the T-12 version individually and, when delivering the completed questionnaire, the physician asks about doubts in the patient’s understanding and interpretation; Step 4, synthesis and reformulation, review of translated items based on the answers and observations made by the first ten patients – this phase comprises some minor changes, but keeping the semantics; Step 5, reverse translation, submission of the revised T-12 version to a reverse translation, from Portuguese into English, by a professional translator, who was not part of any of the initial translations, and preferably a native English speaker, for the reverse translation (RT) version; finally, Step 6, submission to an expert committee, examination of the latest English version (TR) by an “expert committee”, composed of bilingual experts, in this case bilingual dermatologists, and by the author of the original questionnaire, Ramsey Alsarraff, with suggested adaptations being made as many times as necessary, to compare with the original version of the questionnaire and be accepted by the expert committee and by the author of the original questionnaire. In the end, there is the final translated and adapted version of the questionnaire.
We chose another general QOL questionnaire to statistically evaluate the correlation between it and the SROE: the Dermatology Life Quality Index (DLQI),12 in its translated and validated Brazilian Portuguese version, because this version is already known in the dermatological environment.13
The sample size regarding the minimum size of a sample for conducting factor analysis, according to Crocker and Algina,14 is based on the general rule of using 10 subjects per variable, with a minimum of 100 subjects in the total sample. Therefore, as the score studied has six items, it was calculated that a sample of 60 subjects would be sufficient and 100 would be ideal for carrying out this analysis. Regarding the test-retest, it is necessary to evaluate 16 patients to detect a difference of 50% of the standard deviation between the assessments, considering a power of 90%, an α of 0.05, and a correlation between the measurements of 0.8. This calculation was performed using the WINPEPI 11.65 program.15
Patients treated at the XXX Corrective Dermatology Outpatient Clinic between August 2019 and June 2021 (from March to August 2020, activities were suspended due to the Covid-19 pandemic), of any sex and gender, over 18 years of age, and who had an indication of some facial aesthetic procedure were invited to participate in the study. After signing the informed consent form (ICF), the SROE questionnaire in its final translated version and also the DLQI, in that order, were delivered to each patient individually in a closed and quiet environment, where they could respond calmly and without external interferences.
The data were entered in the Excel program and later exported to the SPSS v. 20.0 for statistical analysis. The values of the questions and the total score were described by the mean, median, standard deviation, 25th, and 75th percentiles, and minimum and maximum. We used Cronbach’s alpha to assess the internal consistency and Exploratory Factor analysis to describe the behavior of the scale in the sample considered. Also, we included the six items of the score to perform Factor Analysis, and the factor extraction method was the Varimax orthogonal rotation. The correlation between ARRP and DLQI was performed using Pearson’s correlation coefficient and the test-retest by comparing pre and post-data by Student’s t-test for paired samples and the intraclass correlation coefficient between measurements. A significance level of 5% was considered statistically significant.
The translation process followed the six steps described in the methods, using a private translation agency with native, non-native, and sworn translators. We applied the T-12 consensus version to ten patients at the XXX Corrective Dermatology outpatient clinic to assess language clarity. Two patients had doubts in only one word from one SROE item (questionnaire item 4), and it was replaced by a synonym without any damage to the semantics of the sentence (Chart 2). The expert committee was composed of the authors of this article, and the author of the original questionnaire, Ramsey Alsarraff, approved the TR version.
Sixteen patients participated in the test-retest stage. This assessment found good temporal stability in the measurements. The intraclass correlation coefficient (ICC) between the measurements was 0.995 (p<0.001). There was no statistically significant difference in the scores obtained between the test and the retest.
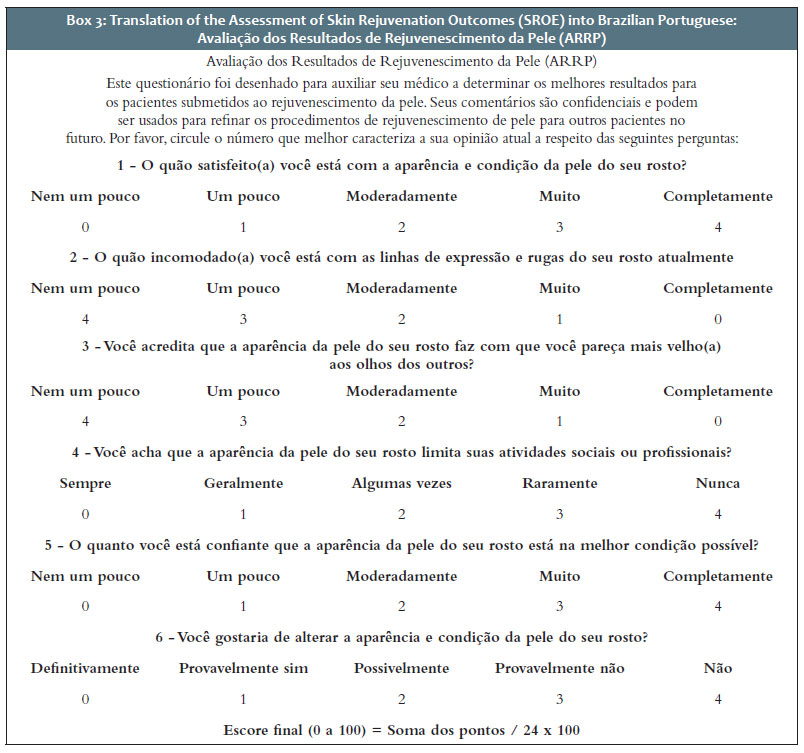
Thus, we concluded the final translated and adapted version of a specific questionnaire to evaluate the outcomes and quality of life in patients with indications for cosmetic procedures. This questionnaire was called “Assessment of Skin Rejuvenation Results” (Avaliação dos Resultados de Rejuvenescimento da Pele - ARRP), and Table 3 shows its ready-to-use translation.
In addition to the first ten patients who entered the initial translation process, 107 patients were included in this study, with a mean age of 53.9 years (standard deviation of 14.5), 95.3% of which were women.
The individual analysis of the questions measured by Cronbach’s alpha was above 0.70 in each item, and the total value between the questions was 0.79, indicating good internal consistency of the scale.
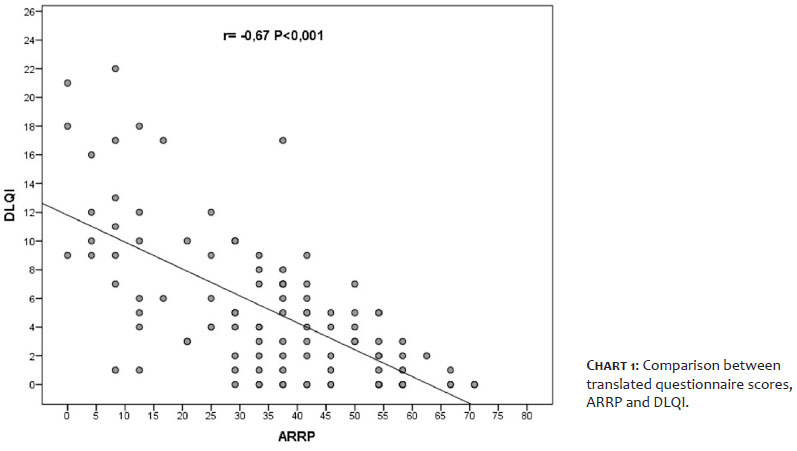
The DLQI score also showed good internal consistency (Cronbach’s α=0.86) in the same sample. We found a strong and inverse, statistically significant correlation between the ARRP and DLQI scores (r= -0.67, p<0.001), that is, as the ARRP increases, the DLQI score decreases (Chart 1).
Translating and adapting validated QOL questionnaires into other languages is probably more important than creating new assessment instruments. The advantage is to allow results to be compared consistently across different countries and cultures. Thus, there must be standardization in the translation and adaptation of the questionnaires.9
The DLQI (Dermatology Life Quality Index), in its translated and adapted version into Portuguese, has been used in studies of the most prevalent dermatoses that impact the patient’s QOL, such as psoriasis and atopic dermatitis.12,13 It is especially valid for chronic and symptomatic diseases, is directed to symptoms, and has general questions. Therefore, it is not suitable for aesthetic complaints.
In this context, for a more detailed and individualized analysis of several other dermatoses, specific questionnaires were created, such as MelasQol for melasma, RosaQol for rosacea, Acne-QoL for acne, and VitiQoL for vitiligo, among others. They were later translated and adapted to our language and culture.16-19 Consequently, a more specific evaluation concerning aesthetic complaints was gaining space in the literature, and specific questionnaires were also developed to assess procedures, most North Americans and a few still in the process of translation and adaptation to our language and culture.20
Kosowski et al., in 2009, in a systematic review, found 442 publications of questionnaires answered by patients, 47 regarding the evaluation of facial cosmetic procedures. Of these, only nine publications met the validation criteria. In English, these specific questionnaires validated for assessing QOL before and after performing cosmetic procedures vary according to the number of items, the complexity of understanding, and score calculations.20 Almost all of them have plastic surgeons’ patients as their target audience and not dermatologists. For example, the FACE-Q – satisfaction with appearance scale questionnaire, recently translated into Brazilian Portuguese in a journal, is a little more extensive and complex because it assesses other aspects of patient dissatisfaction/satisfaction, including relationships with the clinic staff, adverse events of surgical procedures, and financial cost, among others. Also, there are separate questions for each location on the face, such as nose, mouth, and eyes, providing a segmented overview of the analysis.21,22
SROE was published and validated by Ramsay Alsarraff, a plastic surgeon, between 2000 and 2002, in American English, aimed at evaluating the results and impact on quality of life in patients undergoing facial rejuvenation procedures. In the same period, Alsarraff also published three other specific questionnaires intended for evaluating techniques related to the rhinoplasty, the Rhinoplasty Outcomes Evaluation (ROE), the facelift, the Facelift Outcomes Evaluation (FOE), and blepharoplasty, the Blepharoplasty Outcomes Evaluation (BOE). These, already used in several other publications and international research,23,24 and the FOE have already gone through transcultural translation into Brazilian Portuguese.8
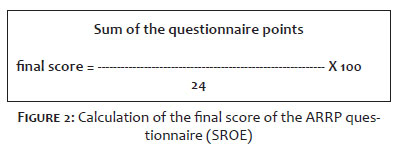
SROE is a questionnaire comprising only six items, is easy to understand, and has a short execution time. These characteristics were essential for our choice of questionnaire to translate and validate. The instrument displays the answer options on a Likert-type scale, which scores from zero to four points. The final score of the ARRP questionnaire (the translated SROE questionnaire) is calculated through the simple sum of the points of the answers marked by the patient, divided by 24 and multiplied by 100, generating a score that varies from 0 to 100 (Figure 2). The higher this score, the better the individual’s QOL.
A Brazilian study evidenced the positive impact on the quality of life of patients undergoing cosmetic procedures, using the WHOQOL-bref (Portuguese version of the WHO Quality of Life Assessment Instrument). It is a wellness and general health questionnaire with no specific questions about complaints and aesthetic evaluations.25
Specific questionnaires have been gaining more and more space for a more reliable and detailed analysis of results and impact on QOL. In the case of questionnaires in cosmiatry, the items created address the patient’s aesthetic complaint, but preserve three essential characteristics for any psychometric analysis: reliability, which translates into the ability to produce consistent and reproducible scores; validity, which is the ability to measure what is intended, and responsiveness, which is the sensitivity in detecting a difference.26
This study makes public and available the ARRP questionnaire (SROE), translated and validated for the Brazilian language and culture, aimed at evaluating outcomes and the impact on the quality of life of facial procedures in cosmiatry.
Jaqueline Barbeito de Vasconcellos 0000-0002-9726-0719
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Daniela Alves Pereira Antelo 0000-0001-8203-1772
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Rosane Orofino-Costa 0000-0002-1603-418X
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. International Society of Aesthetic Plastic Surgery. Demand for cosmetic surgery procedures around the world continues to skyrocket – USA, Brazil, Japan, Italy and Mexico ranked in the top five countries. Available at: https://www.isaps.org/wp-content/uploads/2020/12/Global-Survey-2019.pdf; 2019. Accessed in: 2020 Nov 10.
2. American Society for Dermatologic Surgery. Consumer survey on cosmetic dermatologic procedures. Available at: https://www.asds.net/medical-professionals/practice-resources/asds-consumer-survey-on-cosmetic-dermatologic-procedures; 2019. Accessed in: 2020 Nov 13.
3. Maisel A, Waldman A, Furlan K, Weil A, Sacotte K, Lazaroff JM, et al. Self-reported patient motivations for seeking cosmetic procedures. JAMA Dermatology. 2018;154(10):1167–74.
4. Ferreira MC. Cirurgia plástica estética - Avaliação dos resultados. Rev Soc Bras Cir Plast. 2000;15(1):55–66.
5. The WHOQOL Group. World Health Organization quality of life assessment (WHOQOL): position paper from World Health Organization. Soc Sci Med. 1995;41(10):1403-9.
6. Fleck MP, Leal OF, Louzada S, Xavier M, Chachamovich E, Vieira G, et al. Desenvolvimento da versão em português do instrumento de avaliação de qualidade de vida da OMS (WHOQOL-100). Rev Bras Psiquiatr. 1999;21(1):19-28.
7. Fleck MP, Louzada S, Xavier M, Chachamovich E, Vieira G, Santos L, et al. Aplicação da versão em português do instrumento abreviado de avaliação da qualidade de vida WHOQOL-bref. Rev Saúde Pública. 2000;34(2):178-83.
8. Furlani EAT. Adaptação cultural do questionário de avaliação de resultados em ritidoplastia: facial outcome evaluation. Rev Bras Cir Plást. 2015;30(3):501-5.
9. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine (Phila Pa 1976). 2000;25(24):3186-91.
10. Alsarraf R. Outcomes research in facial plastic surgery: a review and new directions. Aesthetic Plast Surg. 2000;24(3):192-7.
11. Alsarraf R. Outcomes instruments in facial plastic surgery. Facial Plast Surg. 2002;18(2):77-86.
12. Finlay AY, Khan GK. Dermatology life quality index (DLQI) - a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):2106.
13. Martins GA, Arruda L, Mugnaini ASB. Validation of life quality questionnaires for psoriasis patients. An Bras Dermatol. 2004;79:521-35.
14. Crocker L, Algina J. Introduction to classical and modern test theory. Michigan: Wadsworth Pub Co; 1986.
15. Abramson JH. WINPEPI updated: computer programs for epidemiologists, and their teaching potential. Epidemiol Perspect Innov. 2011;8(1):1.
16. Cestari TF, Balkrishann R, Weber MB, Prati C, Menegon DB, Mazzott NG, et al. Translation and cultural adaptation to Portuguese of a quality of life questionnaire for patients with melasma. Med Cutan Iber Lat Am. 2006;34:270-4.
17. Tannus FC, Picosse FR, Soares JM, Bagatin E. Rosacea-specific quality of life questionnaire: translation, cultural adaptation and validation for Brazilian Portuguese. An Bras Dermatol. 2018;93(6):836-42.
18. Kamamoto CSL, Hassun KM, Bagatin E, Tomimori J. Acne-specific quality of life questionnaire (Acne-QoL): translation, cultural adaptation and validation into Brazilian-Portuguese language. An Bras Dermatol. 2014;89(1):83-90.
19. Boza JC, Kundu RV, Fabbrin A, Horn R , Giongo N, Cestari TF. Translation, cross-cultural adaptation and validation of the vitiligo-specifi c health-related quality of life instrument (VitiQoL) into Brazilian Portuguese. An Bras Dermatol. 2015;90(3):358-62.
20. Kosowski TR, McCarthy C, Reavey PL, Scott AM, Wilkins EG, Cano SJ, et al. A systematic review of patient-reported outcome measures after facial cosmetic surgery and/or nonsurgical facial rejuvenation. Plast Reconstr Surg. 2009;123(6):1819-27.
21. Klassen AF, Cano SJ, Scott A, Snell L, Pusic AL. Measuring patientreported outcomes in facial aesthetic patients: development of the FACEQ. Facial Plast Surg. 2010;26(4):303-9.
22. Gama JT, Rossetto LA, Brito NB, Veiga DF, Ferreira LM. Cross-cultural validation of the FACE-Q Satisfaction with facial appearance overall scale (FACE-Q SFAOS) in Brazilian rhytidoplasty patients. Clinics. 2020;75:e1568.
23. Esteves SS, Ferreira MG, Almeida JC, Abrunhosa J, Almeida e Sousa C. Evaluation of aesthetic and functional outcomes in rhinoplasty surgery: a prospective study. Braz J Otorhinolaryngol. 2017;83:552-7.
24. Bater KL, Ishii M, Nellis JC, Joseph A, Papel ID, Kontis TC, et al. A Dual approach to understanding facial perception before and after blepharoplasty. JAMA Facial Plast Surg. 2018;20(1):43-9.
25. Ribeiro F, Steiner D. Quality of life before and after cosmetic procedures on the face: a cross-sectional study in a public service. J Cosmet Dermatol. 2018;17(5):688– 92.
26. Deshpande PR, Rajan S, Sudeepthi BL, Abdul Nazir CP. Patient-reported outcomes: a new era in clinical research. Perspect Clin Res. 2011;2(4):137-44.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}