


Gisele Viana Oliveira1; Leandra D’Orsi Metsavaht2
Submitted on: 10/10/2021
Approved on: 22/11/2021
Financial support: None
Conflict of interest: None
How to cite this article: Oliveira GV, Metsavaht LD. A.S.A.P. - The first algorithm to treat keloids and hypertrophic scars. Surg Cosmet Dermatol. 2022;14:e20220100.
Keloids (K) and hypertrophic scars (HS) are highly prevalent, but their treatment is still challenging. Several treatments are beneficial to treat K/HS, but there is still no protocol or algorithm to address scars following an organized step-by-step and justifying each type of treatment in the scar phases.This study aims to present an algorithm to treat keloids/scars. It has been used for several years in our clinic and helps organize several therapies to treat scars. Combined, these sequences of treatments lead to progressive improvement in K and HS.
Keywords: Acne keloid; Hypertrophic scar; Keloid.
Keloids (K) and hypertrophic scars (HS) are highly prevalent. However, their treatment is still significantly challenging.1 Symptoms such as itch and pain, and aesthetic and psychological complaints negatively interfere with affected individuals’ health-related quality of life (HRQL) and burden of keloid disease.1,2 Surgery frequently leads to recurrence,1,2 and the bad outcome can be interpreted as malpractice in litigation, which is always a concern among plastic surgeons and dermatologists.3
During a prospective randomized study to investigate the effectiveness of silicone dressings to treat scars due to an anti-scarring silicone effect, or occlusion, we employed silicone or hydrocolloid sheets on a group of K/HS, and we observed that both dressings were successful in decreasing K/ HS physical and subjective parameters.We also observed that the injection of triamcinolone in previously softened lesions was less painful, and the drug could diffuse throughout the whole lesion.4 On our outpatient clinic focused on K/HS treatment, we later found out that after using this “softening” procedure for several weeks, fewer injections of steroids were sufficient to treat large lesions that previously would require more sessions.5We have later incorporated technologies such as Intense Pulsed Light (IPL), which made the injections even easier, motivating us to write a protocol to treat scars.5 Also, the increased number of patients with atrophic scars after steroid injections on K/HS referred to our ambulatory became part of our incentive; we observed that following the guidelines of our protocol could avoid scar atrophy, which also leads to patient dissatisfaction.
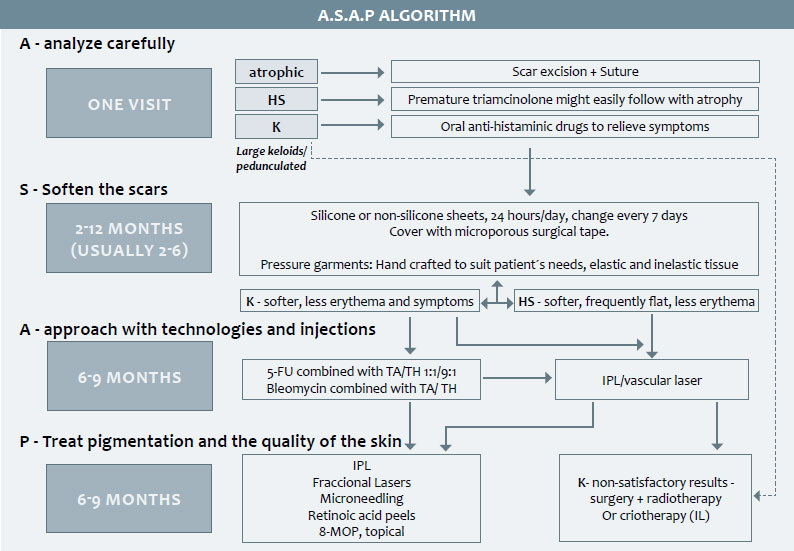
The objective of this manuscript is to share a simple algorithm to treat K and HS.The A.S.A.P algorithm discusses the rationale to combine four sequential steps, leading to a progressive improvement in K/HS.
Patients that come to their first appointment to the keloids and scars outpatient clinic can be separated into four groups of scars:
1) K/HS, without previous treatments; 2) Post-burn or post-traumatic scars, referred to our facility after hospital discharge; 3) Recurrent keloids, after previous therapies; usually treated with surgery, cryotherapy, or steroid injections; 4) Atrophic scars, after the complete resolution of a previous K/HS, due to corticosteroid injections.
This last subset of patients is usually as dissatisfied as patients of the three other groups.Although previous K or HS improved after receiving multiple triamcinolone injections, or even occlusive steroids impregnated tapes for long periods, these scars evolved into depressed, achromic, teleangiectasic lesions.
Steroid injections are popular among dermatologists and plastic surgeons due to the apparent ease of the technique and the possibility to be performed during the first appointment as an in-office procedure.Thus, they are usually chosen as the first approach to K/HS.While litigation and lawsuits involving cosmetic surgery are a growing concern, verifying the real need for drug administration or a medical procedure is an essential step to avoid iatrogenesis.3
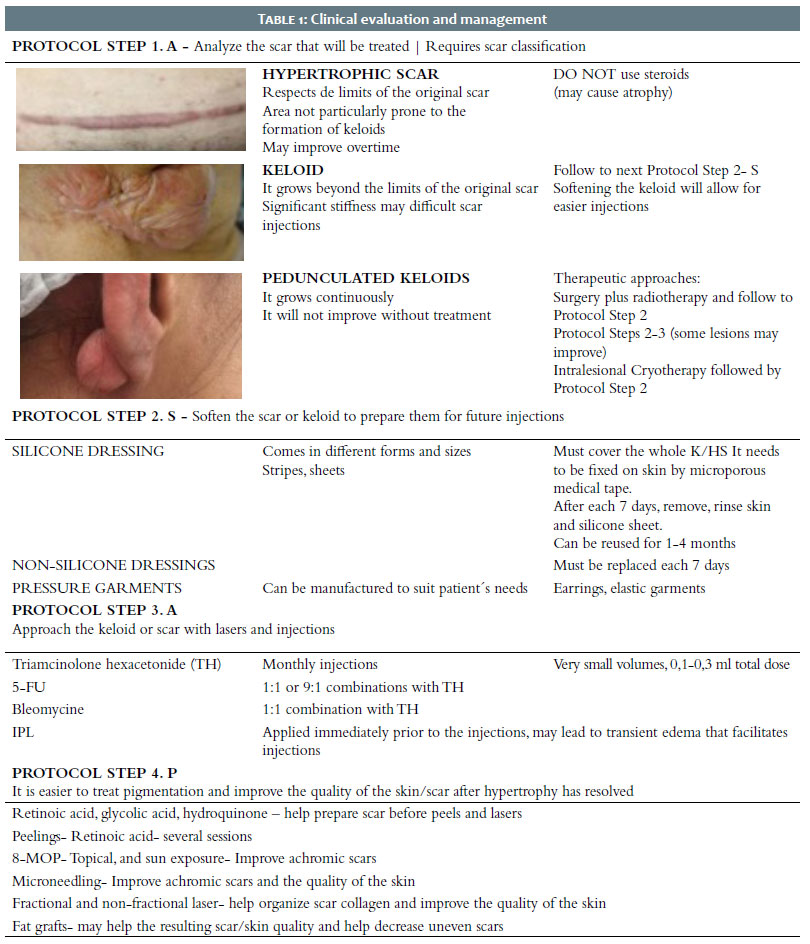
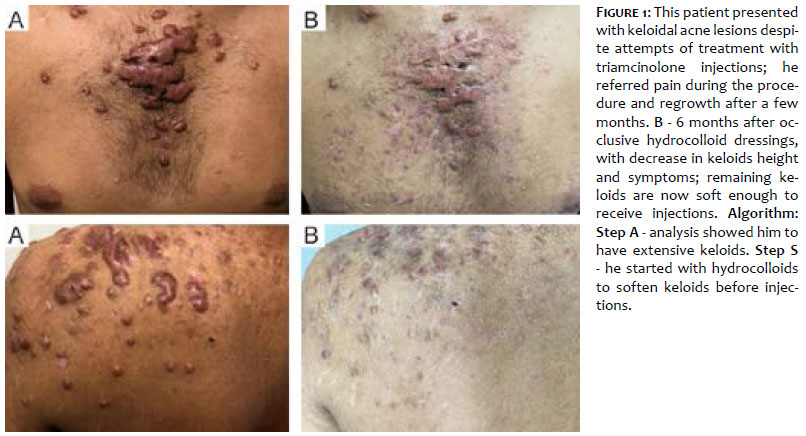
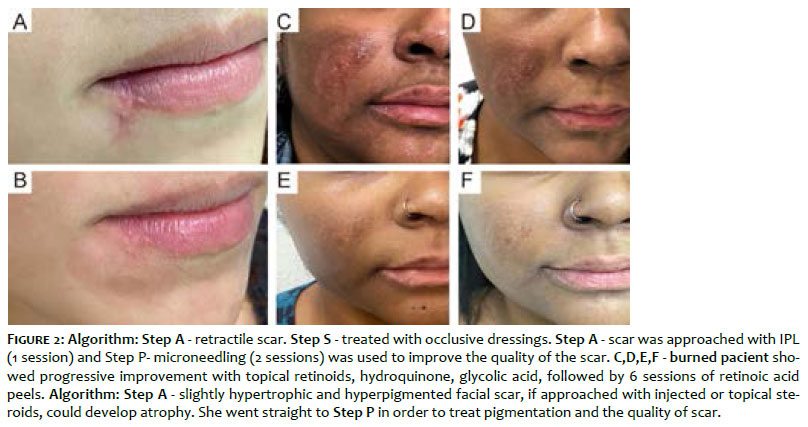
The first algorithm phase (“A” - assessment) requires the physician to classify the scar to be treated, and analyze the best approach for each one of these lesions (Table 1). Steroids should not be used as a first method to treat hypertrophic scars, as natural subsequent atrophy might follow, and steroids could maximize the outcome. Keloids may need steroids injections at some point, but they may respond better to injections after softening by occlusive dressings – the next algorithm (Step “S” - Figure 1). Large lesions such as pedunculated earlobe keloids may be referred for surgery plus radiotherapy, or intralesional cryotherapy, with further follow-up and eventual referral to algorithm Steps 2, 3, and 4 to avoid keloid recurrence (Table 1). Retractile scars may also benefit from surgery in the beginning, although some may be treated with noninvasive methods5 (Figure 2.A and B).
Histamine H1 blockers are anti-inflammatory and antiproliferative drugs that relieve pain and itching sensations on keloids and hypertrophic scars. They inhibit the deposition of collagen by a mechanism of TGF-beta suppression.6 Oral antihistaminic drugs are given on this first treatment phase to relieve symptoms of very itchy scars.Therefore, Step A - “Analyze before any treatments” is the first algorithm stage (Figure 1, A, C, Figure 3,Table 1).
Steroids and anti-neoplastic injections are worldwide accepted methods to treat K and HS. However, their use on keloids with substantial stiffness can be challenging, causing significant patient discomfort and pain. We have previously described that occlusive dressings can help soften the scars before the injections, decreasing pain and allowing lower steroid doses to diffuse better on the fibrotic tissue4 (Figure 1,A, B,Video 1).
Occlusive silicone and hydrocolloid dressings lead to a comparable decrease in volume, symptoms, and erythema, finally softening the K/HS.4 Scars treated with both dressings improve Vancouver Scar Scale parameters and reduce intra-scar pressure, facilitating intralesional triamcinolone (TA) injections.4 Hydrocolloids are self-adhering and chosen to treat body regions that have greater mobility, such as eyelids and hands.5 Silicone and non-silicone dressings are covered with microporous tape and can be changed each 7-15 days.4,5 After 2-4 months, a significant improvement in pain/itching and scar pliability are observed, and injections are easily performed in softer scars4,5 (Video 1). Occlusive dressings and pressure garments may lead to a satisfactory outcome even without injections and technologies (Figure 1. C, D, E).
Pressure garments (PG) are a worldwide accepted method to treat K/HS6 and they are also employed in this phase. Garments’ correct use is mandatory to exert their effects; they should contact the whole scar for several hours/day, and promote blanching.7 PG helps dressings stay in place and protects the scar from sun exposure.We customize handcrafted garment devices using elastic and inelastic fabrics combined in different models to suit patients’ needs.4 Most HS become flat solely by the dressings and PG, as well as small K (Figure 1. C, D, E). An adverse event commonly observed in this phase is “miliaria”, due to the long periods of occlusion. We advise patients to remove the dressings and garments for two days, rinsing the affected skin several times. It is important to mention that pain and itching significantly decrease during algorithm stage “S”.4,5 Patients who present complete flattening do not need to go through the next algorithm step (“A”), but can follow to the last algorithm phase (“P”) (Figure 3).
Algorithm step 2 “S” can be achieved after 1-4 months of occlusive (silicone and non-silicone) dressings and pressure garments.
Once the K/HS is softened, it becomes prone to receive less painful injections with a better drug diffusion into the scar tissue4 (Figure 1, B).Triamcinolone acetonide (TA) is the preferred intralesional drug to treat HS/K. However, it has been discontinued in Brazil, where triamcinolone hexacetonide (TH) is now used with satisfactory results.5 The combination of TA with 5FU is more effective to treat scars than TA.5 It can be used in different combinations with acceptable results.8 Bleomycin seems to be more effective than 5-FU,9 but it needs extra care during dilution to prevent inhalation, because it shows a higher incidence of hyperpigmentation, and its manipulation may require extra regulatory rules that may limit its use.Antineoplastic drugs are used in low doses, always combined with triamcinolone.The rationale is to be highly effective with the lowest possible volume. Pregnancy should always be ruled out.5
Intense Pulsed Light (IPL) is effective to treat HS/K, targeting scar vascular proliferation and pigmentation.10 IPL is used immediately before the injections. Scars covered with dressings for several weeks become less pigmented, allowing a safer IPL session, except for higher skin phototypes11 patients.The transient swelling that follows IPL application might enhance TH spreading throughout the scar.
Algorithm Step 3 - “A”- can be achieved using triamcinolone injections, which may be associated with antineoplastic drugs Bleomycin and 5-FU, with IPL sessions immediately before the injections.
K/HS treated with occlusion, pressure garments, IPL, triamcinolone, and antineoplastic drugs become flat and pale. However, hyper/hypopigmentation frequently remains.The last stage of this algorithm (“P”) focuses on improving the quality of the skin and the mixed scar pigmentation.Topical retinoids, the association of glycolic acid and hydroquinone, chemical peelings, and microneedling are then combined to achieve a more uniform scar color.12 Topical tretinoin improves skin/scar by modulating keratinization and the differentiation of fibroblasts and keratinocytes. Retinoic acid (RA) peels are safely used in higher phototypes, leading to clinical improvement in the skin texture and appearance13 after 5-10 serial sessions (Figure 2. C, D, E, F, table 1).
The inkless tattoo microneedling has been described as an effective “needle dermabrasion” treatment for different scar types, with special benefits regarding achromic scars repigmentation14 (Figure 2.A,B).Satisfactory results can be achieved after just one session in different types of scars14 (Table 1).
Similar to other authors, we also treat the achromic scars using topical psoralen combined with daylight exposure.15 A compounding 0,5%-1% (8-methoxypsoralen) cream was applied to the scar, exposed to sunlight starting 3 minutes/day, 3-4 times/week, and increasing 2 minutes/week up to 15 minutes (Table 1).
Autologous melanocytes transplantation16 and fat graftings17 may also be used on the last protocol phase to help achieve improved cosmetic results, as well as IPL, erbium, and CO2 fractional lasers. K is frequently observed in the skin of color and Brazilian patients culturally prone to sun exposure, leading to scar hyperpigmentation, although during the previous steps the skin usually loses its tanning (Table 1).
Nonablative fractional erbium (1540 wavelength), CO2 and ablative 2950 wavelength lasers contribute to a final retouch, allowing improvement of scar color and texture17,18,19 (Table 1).
The A.S.A.P. algorithm has been extensively used in our clinic. It helps organize the several steps needed to improve those lesions (Figure 1, Figure 2), which may be used as a guide to treat virtually any HS/K after trauma, surgery, piercings, acne, and viral diseases that affect skin and burns (Figure 3).
Gisele Viana Oliveira 0000-0001-5101-7097
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Leandra D’Orsi Metsavaht 0000-0001-9009-9929
Approval of the final version of the manuscript; preparation and writing of the manuscript; study design and planning; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
1. Bijlard E, Kouwenberg CA, Timman R, Hovius SE, Busschbach JJ, Mureau MA. Burden of keloid disease: a cross-sectional health-related quality of life assessment. Acta Derm Venereol. 2017;97(2):225-9.
2. Bock O, Schmid-Ott G, Malewski P, Mrowietz U. Quality of life of patients with keloid and hypertrophic scarring. Arch Dermatol Res. 2006;297(10):433-8.
3. Peer RF, Shabir N. Iatrogenesis: a review on nature, extent, and distribution of healthcare hazards. J Family Med Prim Care. 2018;7(2):309-14.
4. Oliveira GV, Nunes TA, Magna LA, Cintra ML, Kitten GT, Zarpellon S, et al. Silicone versus nonsilicone gel dressings: a controlled trial. Dermatol Surg. 2001;27(8):721-6.
5. Oliveira GV, Gold MH. Hydrocolloid dressings can be used to treat hypertrophic scars: an outpatient dermatology service devoted to treat keloids and challenging scars. J Cosmet Dermatol. 2020;19(12):3344-8.
6. Viera MH, Amini S, Valins W, Berman B. Innovative therapies in the treatment of keloids and hypertrophic scars. J Clin Aesthet Dermatol. 2010;3(5):20-6.
7. DeBruler DM, Baumann ME, Zbinden JC, Blackstone BN, Bailey JK, Supp DM, et al. Improved scar outcomes with increased daily duration of pressure garment therapy. Adv Wound Care (New Rochelle). 2020;9(8):453-61.
8. Metsavaht LD, Garcia CAR. Intralesional injections of 5-FU in the treatment of keloids, hypertrophic scars, and contractures. Surg Cosmet Dermatol. 2015;7(1):17-24.
9. Sharma S, Vinay K, Bassi R. Treatment of small keloids using intralesional 5-fluorouracil and triamcinolone acetonide versus intralesional bleomycin and triamcinolone acetonide. J Clin Aesthet Dermatol. 2021;14(3):17-21.
10. Erol OO, Gurlek A, Agaoglu G, Topcuoglu E, Oz H. Treatment of hypertrophic scars and keloids using intense pulsed light (IPL). Aesthetic Plast Surg. 2008;32(6):902-9.
11. Fitzpatrick RE. Treatment of inflamed hypertrophic scars using intralesional 5-FU. Dermatol Surg. 1999;25(3):224-32.
12. Shenoy A, Madan R. Post-inflammatory hyperpigmentation: a review of treatment strategies. J Drugs Dermatol. 2020;19(8):763-8.
13. Cucé LC, Bertino MC, Scattone L, Birkenhauer MC. Tretinoin peeling. Dermatol Surg. 2001;27(1):12-4.
14. Silva BAC, Ataide MS, Mamere LRO, Dias GF. Microneedling in scars treatment: benefits of a single session. Surg Cosmet Dermatol. 2020;12(1):57-62.
15. Alzahrani Z, Ghobara YA, AlJasser MI. Postburn leukoderma successfully treated with topical daylight psoralen UVA therapy. Dermatol Ther. 2020;33(2):e13248.
16. Vyas NS, Lawrence KL, Griffith JL, Hamzavi IH. Autologous, noncultured epidermal cell suspension grafting in the management of mechanically and chemically induced leukodermic scars. J Cutan Med Surg. 2015;19(5):488-93.
17. Klinger M, Klinger F, Caviggioli F, Maione L, Catania B, Veronesi A, et al. Fat grafting for treatment of facial scars. Clin Plast Surg. 2020;47(1):131-8.
18. Willows BM, Ilyas M, Sharma A. Laser in the management of burn scars. Burns. 2017;43(7):1379-89.
19. Oliveira GV, Metsavaht LD, Kadunc BV, Jedwab SKK, Bressan MS, Stolf HO, et al. Treatment of keloids and hypertrophic scars. Position statement of the Brazilian expert group GREMCIQ. J Eur Acad Dermatol Venereol. 2021;35(11):2128-42.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}