


Mônica Albuquerque Costa1; Érika Santos Freire1; Maria Cristina Vieira Andrade1; Marcio Roberto Silva2; Maria Christina Marques Nogueira Castañon3; Nádia Rezende Barbosa Raposo1
Submitted on: 25/06/2021
Approved on: 03/11/2021
Financial support: None
Conflict of interest: None
How to cite this article: Costa MA, Freire ES, Andrade MCV, Silva MR, Castañon MCMN, Raposo NRB. Microneedling and epidermal growth factor (EGF) as strategies for the acne scars treatment. Surg Cosmet Dermatol. 2022;14:e20220068
BACKGROUND: The microneedling technique and the transdermal drug delivery are indicated to treat acne scars.
OBJECTIVE: Evaluation of the microneedling technique associated with the drug delivery of the epidermal growth factor (EGF).
METHODS: Randomized double-blind clinical trial of 30 patients divided into two groups: (1) - two microneedling sessions with a 30-day interval, (2) - two microneedling sessions with the same interval but associated with EGF drug delivery. The patients were evaluated clinically (global acne scarring grading system - Goodman and Baron) global acne scarring grading system via multispectral image and through self-perception questionnaires. The statistical analysis (Student T-test, SNK test, analysis of variance) was performed with the SisVar software (UFLA, 1996).
RESULTS: The groups were homogeneous regarding age, gender, and phototype. Clinical assessments showed a reduction in severity scores for both groups. The multispectral analysis revealed a decrease in porphyrins (p = 0.0296) and an improvement in skin texture in group 2 subjects.
CONCLUSION: Microneedling therapy was effective and safe for the acne scars treatment, and EGF demonstrated to be a promising strategy as well.
Keywords: Acne vulgaris; Cicatrix; Skin
Acne is an inflammatory disorder, and its primary complication is the development of scars.1 These can occur at any stage of the disease, but early intervention in the treatment of acne is believed to be the most effective way to prevent them.2 They cause a negative aesthetic impact and generate psychosocial damage, reducing the quality of life of affected patients.3 The treatment of acne scars still represents a challenge and instigates the search for other therapies and/or safer and more effective procedures.
The microneedling technique, also known as percutaneous collagen induction,4 is considered a minimally invasive procedure, where a device pierces the skin, physically breaking up compact bands of collagen in the superficial layer of the dermis, leading to the formation of microchannels, thus allowing the transdermal administration of substances (drug delivery).5 This technique can induce an inflammatory response and stimulate neovascularization and formation of type III collagen, later replaced by type I collagen.6 Also, it promotes the release of transforming growth factors (TGF) alpha and beta, connective tissue growth factors (CTGF), platelet-derived growth factors (PDGF), and fibroblast-derived growth factors (bFGF), as well as epidermal growth factor (EGF).7
EGF decreases sebum production by suppressing lipogenesis. It also demonstrates an anti-inflammatory effect, modulating the expression of cytokines in keratinocytes, inducing changes in the differentiation and maturation of suprabasal keratinocytes, and promoting downregulation of pro-fibrotic factors such as TGF beta-1.8 These effects suggest that its use is effective and that it is a promising therapeutic option for acne scars.
It is the first clinical trial that assessed the influence of EGF in drug delivery associated with microneedling technique, simultaneously comparing these strategies through multispectral analysis of skin conditions and acne scar assessment tools: global acne scarring grading system (Goodman, Baron, 2006), quality of life assessment questionnaires – Dermatology Quality of Life Index (DLQI), and adapted Cardiff Acne Disability Index (CADI).
It was a randomized, double-blind, experimental clinical study with a quantitative research model, conducted in a group of patients with acne scars who underwent two microneedling sessions associated or not with EGF drug delivery, performed by a dermatologist. The Ethics Committee in Research with Human Beings of the Federal University of Juiz de Fora approved this study under protocol number 2,702,622. Informed consent was obtained from all participants included in the study.
We performed randomization using Excel software, allocating patients randomly and equally (n=15) into group one (intervention = two microneedling sessions) or group two (intervention = two microneedling sessions associated with drug delivery of EGF), with subsequent loss to follow-up of two patients, one from each group.
The study design was entirely randomized, with responses repeated over time. The criteria analyzed to obtain the results were: analysis of the parameters obtained in the technological device (VISIA®) that performs multispectral analysis of skin conditions; responses obtained through the adapted CADI and DLQI questionnaires; and the values obtained in the Goodman and Baron’s (2006) global acne scarring grading system. The groups analyzed over time were formed by a combination of treatments (one and two) and sex (woman and man), constituting four groups.
We included patients with a clinical diagnosis of acne scars, of both sexes, aged between 18-45 years, Fitzpatrick’s skin phototype IV, and who did not use any type of systemic and/or topical dermatological or aesthetic treatment in the last six months in the face. We excluded individuals who were pregnant/lactating, who presented photosensitivity, immunosuppression, active infection (such as herpes simplex, impetigo, among others), severe types of acne (acne conglobata and fulminant), predisposition to keloid formation, presence of cutaneous malignancies, self-declared allergy to EGF and/or anesthetic, and those who did not complete all stages of the study.
In group one, two microneedling sessions were performed as a single strategy and with an interval of 30 days between sessions, and in group two, in addition to the two microneedling sessions of the same interval, application of 1 ml of epidermal growth factor (EPIfactor® in 30g of vehicle – 4000 ng/g) after the procedure. Only the use of sunscreen was indicated for home care.
The disposable manual device used was a dermaroller (DrRoller MTS Roller, MiRoll, Korea), containing a mobile cylinder with eight rows of 2 mm stainless steel needles, totaling 192 needles.
The facial skin surface was sanitized with 70% ethanol, and then an anesthetic block was performed using 2% lidocaine and 4% lidocaine cream (topical) to minimize discomfort.
Each facial region was pierced eight times in different directions (vertical, up and down, horizontal, right and left, and both diagonal directions) to achieve the endpoint of uniform petechiae and purpura across the entire face. We did not conduct skin preparation with retinoid derivatives or depigmenting agents to avoid confounding bias in the study.
At time zero (T0), we perform the clinical assessment and classification of acne scars using the Goodman and Baron scale (2006), multispectral skin analysis, and quality of life assessment using the adapted DLQI and CADI questionnaires. At time one (T1), corresponding to three to seven days after T0, we performed the first session of microneedling alone or associated with EGF. We conducted the second microneedling session, multispectral imaging assessment, clinical assessment, and quality of life assessment at time two (T2 - 30 days after T1). At time three (T3 - 60 days after T1) and time four (T4 - 90 days after T1), we performed multispectral analysis and clinical evaluation. The last quality of life assessment was performed applying the described questionnaires at time five (T5 - 180 days after T1). The same investigator conducted all these instruments for each volunteer.
For the statistical analysis, the transformation of the mean values and the tests were conducted: T-Test (to compare the groups between the proposed treatments) and SNK Test (to compare the treatments over the study period).
The simple stratified sampling method with stratification defined for four groups, aiming to meet the analysis domains established for the study (treatment strategies: one [microneedling] and two [microneedling associated with EGF drug delivery], in addition to gender [man and woman]), was used as a strategy to reduce the coefficient of variation and, thus, allow intragroup and intergroup comparisons over time. Therefore, each individual became his or her control over time.
Demographic characteristics
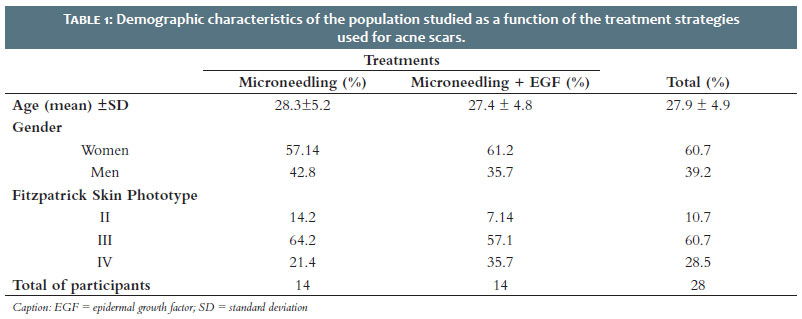
There were no statistically significant differences regarding the demographic characteristics (age, sex, and skin type) of the patients between the two treatment groups (Table 1). Regarding the clinical pattern of acne scar classification, all patients had a combination of atrophic scar subtypes in the studied period: icepick, boxcar, and rolling.
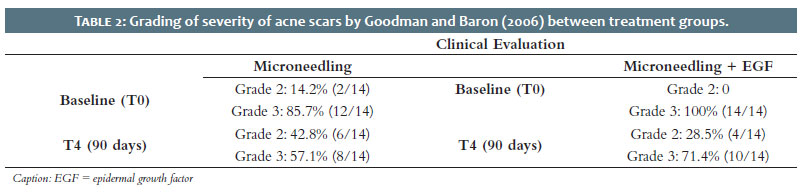
The classification of acne scars severity by Goodman and Baron (2006) global acne scarring grading system scores four grades that classify them into grade one (macular scar); grade two (mild), grade three (moderate), and grade four (severe). Before performing any treatment strategy (time zero or baseline), two (7.1%) patients were classified as grade two (mild) and 26 (92.8%) as grade three (moderate), considering the studied population (n=28). At the end of treatment (90 days - T4), 10 (35.71%) patients were classified as mild and 18 (64.28%) as moderate, considering the population studied. Table 2 summarizes the results regarding the stratification by groups, and no statistically significant differences were found between the initial and final scores for both strategies employed (p=0.25 for group one and p=0.12 for group two).
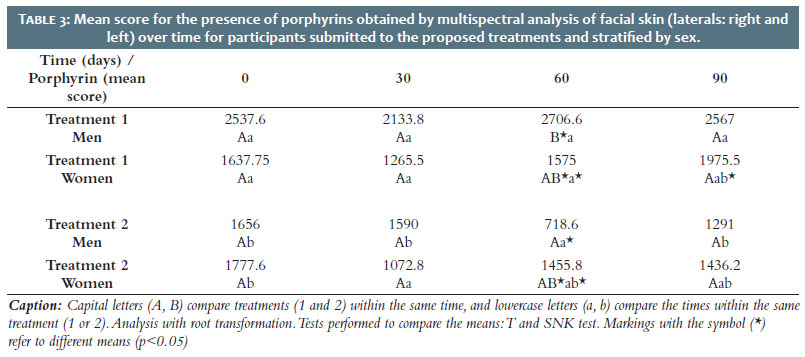
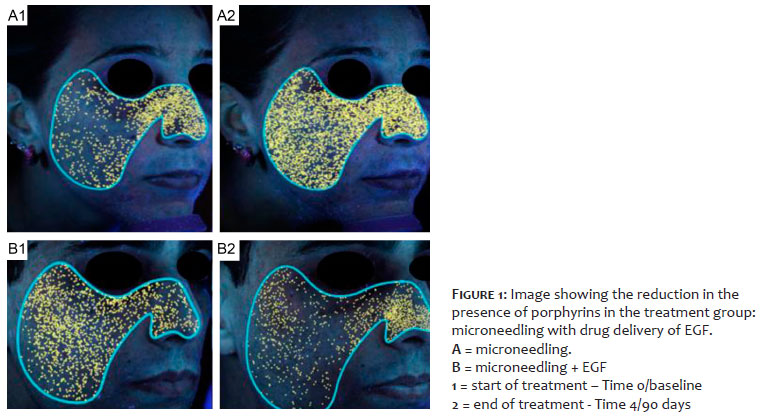
There was a reduction in porphyrin means, which may reflect a reduction in bacterial colonization by Cutibacterium acnes (C. acnes) (p=0.0296). Porphyrins means in group one in both sexes did not change significantly over time, but for treatment group two, they tended to decrease at time 60 (men) and time 30 (women). At time 60, the porphyrin means in both groups was significantly different for men, with a higher mean for group one than for group two, indicating that the use of EGF in group two was important to control the proliferation of C. acnes and thus reduce the total amount of porphyrins on the face (Table 3 and Figures 1A and 1B).
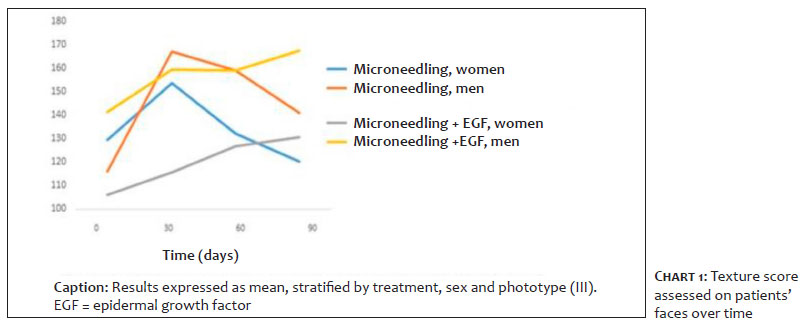
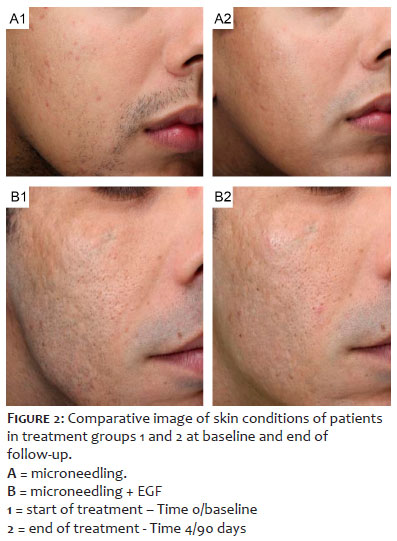
For the variables pores, wrinkles, red area, and spots on the entire face, the comparison of means between the times and treatments performed did not show a statistically significant difference (p>0.05). However, regarding texture in the frontal region, the overall analysis without stratification by sex and skin phototype showed a trend towards improved skin quality (p=0.059) for the treatment effect. Regarding the texture in the lateral area, when performing stratification by sex and skin phototype, a slight increase in the mean values of this parameter was observed, which clinically translates into a skin improvement (Chart 1) without, however, being statistically significant (p=0.18). In Figure 2, it is possible to notice the improvement in the skin texture of patients belonging to the proposed treatments.
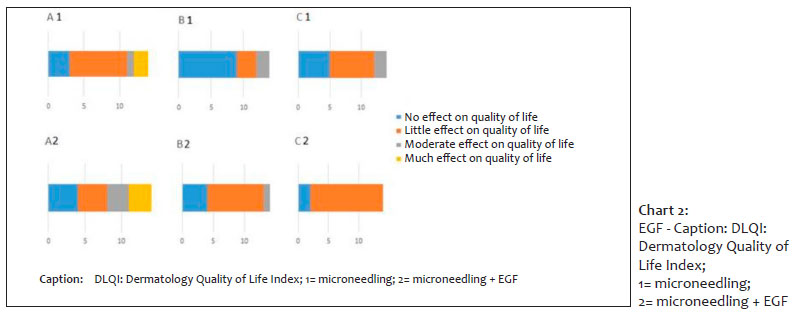
DLQI is a questionnaire that assesses skin diseases in general and grades them according to the following score: 1 (0-1 point) the skin disease does not interfere with the patient’s quality of life; 2 (2-5 points), the skin disease interferes little with the quality of life; 3 (6-10 points), the interference is moderate; 4 (11-20 points), there is a lot of interference in the quality of life; and 5 (21-30 points), there is huge interference in the quality of life of those affected. The results showed no significant differences in the total variation of scores (final score – initial score) for both treatments used (p=0.25 for treatment one and p=0.12 for treatment two). Before the intervention (time zero or baseline), of the 28 patients who participated of the study, 7 (25%) were classified as score 1; 12 (42.85%) as score 2; 4 (14, 28%) patients as score 3; 5 (17.85%) as score 4; and no patient was classified as score 5 (n=28). Based on the stratification of the groups by treatment, in treatment one (microneedling), 3 (21.42%) patients were classified as grade 1; 8 (57.14%) as grade 2; 1 (7.14%) as grade 3; and 2 (14.28%) as grade 4 (n=14). For treatment two (microneedling associated with drug delivery of EGF), 4 patients (25.57%) were classified as grade 1; 4 (25.57%) as grade 2; 3 (21.42%) as grade 3; and 3 (21, 42%) as grade 4 (n=14). At the end of the treatment, 7 (25%) patients scored 1; 19 (67.85%) scored 2; 3 (10.71%) scored 3; and no patients scored 4 and 5, considering the population studied (n=28). Based on the stratification of the groups by treatments, in treatment one (microneedling), 5 (35.71%) patients were classified as grade 1; 7 (50%) as grade 2; and 2 (14.28%) as grade 3 (n =14). For treatment two (microneedling associated with drug delivery of EGF), 2 (14.28%) patients were classified as grade 1 and 12 (85.71%) as grade 2 (n=14) (Chart 2).
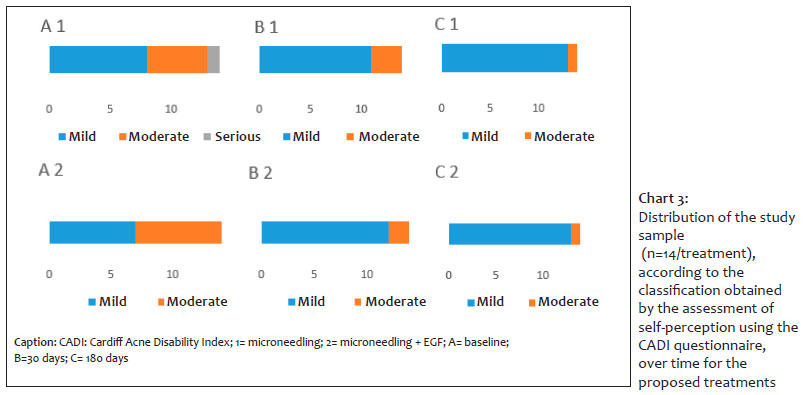
The score obtained in the CADI questionnaire grades acne as mild (1) when the sum of the points obtained in the questionnaire varies from 0-5; moderate (2), when the sum varies from 6-10; and severe (3), when this sum varies from 11-15 points. Before conducting the intervention (time 0 or baseline), 15 (53.57%) patients were ranked as mild; 12 (42.85%) as moderate; and 1 (3.57%) as severe. In the last period of evaluation (time 5/180 days), 26 (92.85%) patients were graded as mild, and 2 (7.14%) as moderate (n=28). In treatment group one (time 0 or baseline), 8 (57.14%) patients were classified as mild, 5 (35.71%) as moderate, and 1 patient (7.14%) as severe. At the end of the study (time 5/180 days), 13 (92.85%) patients were graded as mild and only 1 (7.14%) as moderate (p=0.062). For treatment group two, 7 (50%) patients were ranked as mild and 7 as moderate, at time 0-baseline. At the end of treatment (time 5/180 days), 13 (92.85%) patients were classified as mild and only 1 (7.14%) as moderate (p = 0.12) (Chart 3).
Acne scar management has been a challenging task and a focus of interest for dermatologists. Skin microneedling is a modality for remodeling acne scars, with minimal damage to the epidermis, few adverse events, and shorter recovery time after the procedure, compared to other methods with the same purpose.10,5,11 Regarding patient selection, the literature presents several clinical trials with microneedling treatment for acne scars in young patients of both sexes. As verified by Harris et al. (2015), the average number of microneedling sessions needed to achieve satisfactory results was three sessions with mean intervals of four weeks (two to eight weeks), chiefly using 1.5 mm needles (1 mm to 3 mm) in length.12 In agreement with most of the studies analyzed, we selected 30 patients with acne scars, with a mean age of 27.9 ± 4.9 years, skin phototypes IV, of both sexes. After the loss to follow-up (n=2), 17 women and 11 men completed the study (n=28). Two microneedling sessions were performed using a 2 mm needle at an interval of four weeks between them.
Kalil, Frainer et al. (2015) selected 10 patients aged 20-40 years, of both sexes, with atrophic acne scars, who underwent three sessions of microneedling using a 2mm needle. The study used anatomopathological analysis and digital photographs.13 There was application drug delivery of growth factors (EGF, IGF, TGF-beta3) using masks. The authors did not find improvement in icepick scars, but they did notice an overall improvement in skin texture and a slight improvement in acne scars. In our study, we also observed an overall improvement in skin texture, especially in those patients who had EGF drug delivery after two microneedling sessions. Additionally, icepick scars slightly improved with shallowing of their depths.
The literature describes that EGF decreases sebum production and has an anti-inflammatory effect, reducing follicular hyperkeratosis. In addition to acting on active acne, it also stimulates the production of dermal matrix constituents, stimulating the production of organized collagen, downregulating TGF-beta1, which has a pro-fibrotic action. With its application in drug delivery, it is expected not only improvement of acne scars but also an enhancement in those patients who have associated active acne (Kim, Yeo, Li et al., 2014; Draelos, 2016; Lian and Li, 2016).8,14,15
Based on these data, applying EGF in drug delivery after microneedling is justified due to its direct effect on the pathogenesis of acne and acne scars and its anti-inflammatory action, which can be beneficial for a more efficient repair of the lesion caused by the procedure.
Al Qarqaz et al. (2018) evaluated 48 patients with skin phototypes III-VI treated with microneedling (Dermastamp® electronic device) and noticed a statistically significant improvement when comparing the treatment scores (before and after) obtained by the Goodman and Baron scales and the post-acne hyperpigmentation index (PAHPI).16 Our study also used different methods to assess the effectiveness of the procedure: Goodman and Baron’s global acne scarring grading system, digital photographs, and adapted generic (DLQI) and specific (CADI) self-perception questionnaires. The generic questionnaires assess the quality of life outside the clinical context (Halioua, Beumont, and Lunel, 2000).17 The specific ones, in turn, are used for a particular disease and, considering that they are manifestations of a determined clinical condition, they are more sensitive when compared to generics. Also, our study demonstrated a reduction in the global acne scarring grading system when comparing the scores before and after treatment, but without statistically significant differences between the grades obtained at the beginning and the end of the treatment.
A literature review performed in consultation with PubMed from 1946-2015 and Embase from 1947-2015, by Harris et al. (2015)12, for microneedling research to treat acne scars, assessed the effectiveness of the procedure alone, combined with other therapies, histological changes, and adverse events. When assessing the technique in isolation, all studies showed improvement with treatment with a reduction in scar severity, based on the Goodman and Baron scale, one of which decreased from 11.7 points to 6.5. Our study showed a reduction in the means with this same assessment instrument in both treatment groups and for both sexes. However, this difference between the beginning (baseline, time zero) in which 7.1% of the patients were classified as grade 2 (mild), and 92.8% as grade 3 (moderate), and the end of the follow-up (90 days, time four) where 35.7% of patients were classified as grade 2 (mild) and 64.2% as grade 3 (moderate), was not statistically significant. However, it is worth noting that the 28.6% reduction in cases classified as grade 3 in both groups may translate into clinical improvement.
Microneedling therapy was effective and safe for treating acne scars, with minimal adverse events and short recovery time. The clinical response, expressed through the variation of the global acne scarring grading system, showed that all patients improved to varying degrees. EGF, used in drug delivery, proved to be a promising active pharmaceutical ingredient as an adjuvant in the acne scars treatment and most patients presented an improvement in quality of life, expressed by the reduction of the values obtained in the adapted DLQI and CADI questionnaires when compared to the initial values.
Mônica Albuquerque Costa 0000-0002-7254-4379
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Érika Santos Freire 0000-0002-2106-2310
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Maria Cristina Vieira Andrade 0000-0002-4205-0618
Author’s contribution: Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Marcio Roberto Silva 0000-0002-0755-4415
Statistical analysis; approval of the final version of the manuscript; study design and planning; active participation in research orientation.
Maria Christina Marques Nogueira Castañon 0000-0002-2995-1761
Approval of the final version of the manuscript; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Nádia Rezende Barbosa Raposo 0000-0001-5271-1048
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Clark AK, Saric S, Sivamani RK. Acne scars: how do we grade them? Am J Clin Dermatol. 2018;19(2):139-44.
2. Fife D. Practical evaluation and management of atrophic acne scars: tips for the general dermatologist. J Clin Aesthet Dermatol. 2011;4(8):50-7.
3. Dréno B, Bissonnette R, Gagné-Henley A, Barankin B, Lynde C, Kerrouche N, et al. Prevention and reduction of atrophic acne scars with adapalene 0.3%/Benzoyl Peroxide 2.5% gel in subjects with moderate or severe facial acne: results of a 6-month randomized, vehicle-controlled trial using intra-individual comparison. Am J Clin Dermatol. 2018;19(2):275-86.
4. Lima E, Lima M, Takano D. Microagulhamento: estudo experimental e classificação da injúria provocada. Surg Cosmet Dermatol. 2013;5(2):110-4.
5. Alster TS, Graham PM. Microneedling: a review and practical guide. Dermatol Surg. 2018;44(3):397-404.
6. Fernandes D. Minimally invasive percutaneous collagen induction. Oral Maxillofac Surg Clin North Am. 2005;17(1):51-63.
7. Fernandes D, Signorini M. Combating photoaging with percutaneous collagen induction. Clin Dermatol. 2008;26(2):192-9.
8. Kim HK, Yeo IK, Li K, Kim BJ, Kim MN, Hong CK. Topical epidermal growth factor for the improvement of acne lesions: a randomized, double-blinded, placebo-controlled, split-face trial. Int J Dermatol. 2014;53(8):1031-6.
9. Goodman GJ, Baron JA. Postacne scarring: a qualitative global scarring grading system. Dermatol Surg. 2006;32(12):1458-66.
10. Iriarte C, Awosika O, Rengifo-Pardo M, Ehrlich A. Review of applications of microneedling in dermatology. Clin Cosmet Investig Dermatol. 2017;10:289-98.
11. Minh PPT, Bich DD, Hai VNT, Van TN, Cam VT, Khang TH, et al. Microneedling therapy for atrophic acne scar: effectiveness and safety in vietnamese patients. Open Access Maced J Med Sci. 2019;7(2):293-7.
12. Harris AG, Naidoo C, Murrell DF. Skin needling as a treatment for acne scarring: an up-to-date review of the literature. Int J Womens Dermatol. 2015;1(2):77-81.
13. Kalil C, Frainer H, Dexheimer S, Tonoli R, Boff L. Tratamento das cicatrizes de acne com a técnica de microagulhamento e drug delivery. Surg Cosmet Dermatol. 2015;7(2):144-8.
14. Draelos ZD. The effect of a combination of recombinant EGF cosmetic serum and a crosslinked hyaluronic acid serum as compared to a fibroblast-conditioned media serum on the appearance of aging skin. J Drugs Dermatol. 2016;15(6):738-41.
15. Lian N, Li T. Growth factor pathways in hypertrophic scars: molecular pathogenesis and therapeutic implications. Biomed Pharmacother. 2016;84:42-50.
16. Al Qarqaz F, Al-Yousef A. Skin microneedling for acne scars associated with pigmentation in patients with dark skin. J Cosmet Dermatol. 2018;17(3):390-5.
17. Halioua B, Beumont MG, Lunel F. Quality of life in dermatology. Int J Dermatol. 2000;39(11):801-6.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}