


Flávia Regina Ferreira1,2; Mariana Oliveira Fernandes1; Marina Thereza Fogo Pereira1; Fernanda da Rocha Gonçalves3
Submitted on: 24/06/2021
Approved on: 18/08/2021
Financial support: None
Conflict of interest: None
How to cite this article: Ferreira FR, Fernandes MO, Pereira MTF, Gonçalves FR. Cutaneous diffuse large B-cell lymphoma, leg type – a typical case. Surg Cosmet Dermatol. 2022;14:e20220065
Cutaneous diffuse large B-cell lymphoma, leg type, is a rare, aggressive, and poorly prognostic neoplasm. It corresponds to 10-20% of cutaneous B-cell lymphomas and mainly affects the lower limbs of older women. We report the case of an 81-year-old woman with painful, fast-growing nodules and tumors in her left leg. Histopathological and immunohistochemical findings, associated with the absence of extra-cutaneous involvement during staging, concluded the diagnosis of cutaneous diffuse large B-cell lymphoma, leg type. The rarity of this limphoma, its typical clinic and epidemiology, and the excellent response to treatment motivated this report.
Keywords: Immunohistochemistry; Diffuse; Lymphoma non Hodgkin; Lymphoma large B-cell, Neoplasms; Therapeutics
Primary cutaneous lymphomas are defined as a heterogeneous group of lymphoproliferative malignancies that affect the skin, with no evidence of extracutaneous involvement at the time of diagnosis.1
Cutaneous B-cell lymphomas (CBCL) account for 20% to 25% of all primary cutaneous lymphomas and are more common in women.1,2
According to clinical, histopathological, immunohistochemical, and molecular criteria, CBCLs are classified by the World Health Organization-European Organization for Research and Treatment of Cancer (WHO-EORTC) - 2018, as centrofollicular and diffuse large B cells, leg type; the latter represents only 4% of all cutaneous lymphomas.1
The rarity of this type of lymphoma, its typical clinic and epidemiology, and the excellent response obtained to treatment motivated this report.
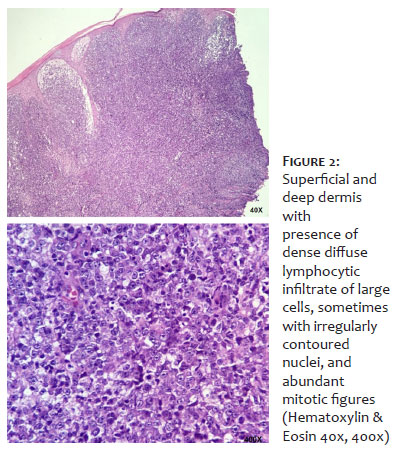
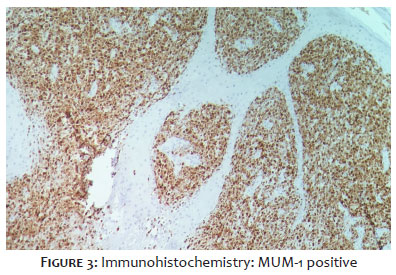
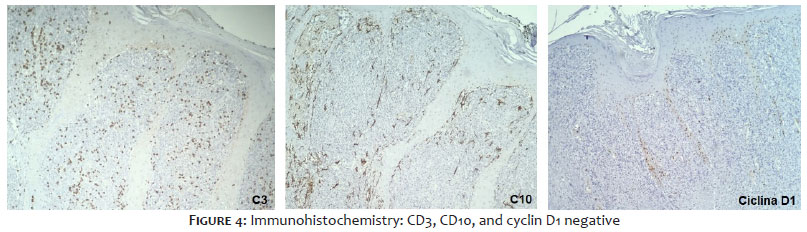
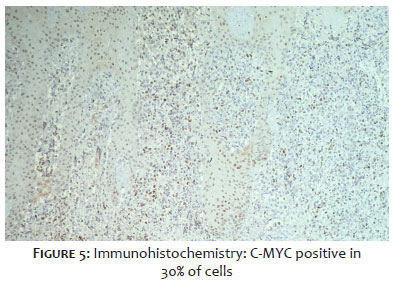
A Caucasian, 81-year-old woman came to the Dermatology Outpatient Clinic complaining of fast-growing “lumps” on her left leg, with one-month evolution. Dermatological examination revealed vegetating nodules and tumors, with an erythematous-yellow fibrinoid surface and the presence of blackened crusts (Figure 1). There was no lymph node enlargement or visceromegaly. The lesions were painful, and the patient denied any systemic symptoms. She mentioned previous trauma as a triggering factor. Also, she had peripheral venous insufficiency and type II diabetes mellitus as comorbidities. The hypotheses put forward were squamous cell carcinoma, amelanotic melanoma, cutaneous metastases, and cutaneous lymphoma. Incisional biopsies were performed in two points. The histopathological study showed ulcerated epidermis with areas of necrosis and the presence of dense and diffuse lymphocytic infiltrate consisting of large cells in the superficial and deep dermis, sometimes with nuclei with irregular contours and abundant mitotic figures (Figure 2). The immunohistochemical panel was positive for Bcl-2, CD20, and MUM1 (Figure 3) and negative for CD3, CD10, and cyclin D1 (Figure 4), concluding a B-cell non- Hodgkin lymphoma diagnosis. Bcl-6 was not performed. The proliferative index by Ki-67 was 90%, and C-MYC was positive in about 30% of the cells (Figure 5).
The patient was referred to the Hebe Camargo Cancer-Fighting Network, where she was staged and diagnosed with diffuse cutaneous large B-cell lymphoma, leg type, T2bN0M0 (Table 1).
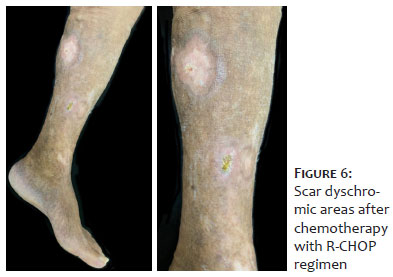
We instituted therapy with R-CHOP regimen (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) and scheduled surgical intervention, which was not performed due to the excellent evolution of the patient (Figure 6). Currently, the patient has only dyschromic cicatricial areas and is under joint follow-up with Dermatology and Oncology.
Diffuse cutaneous large B-cell lymphoma, leg type, comprises a rare, aggressive neoplasm with a poor prognosis.1,3
It corresponds to 10-20% of CBCLs and has a 5-year survival rate of 50%.1,3,4 It mainly affects women of advanced age (70-82 years).1,3,5 Clinically, it manifests as nodular, infiltrative, single, or multiple lesions, which may be located in different sites (lower limbs are the most common). It also presents a rapid progression, agreeing with what was observed in this case. Phlogistic signs and pruritus may be present.1,3
The development of extracutaneous lesions is common, especially among patients who have involvement in the lower limbs, with bone marrow, lymph nodes, and central nervous system is the most affected sites.1,5,6
The diagnosis is made by clinical, histopathological, and immunohistochemical findings.1,2
In histopathology, it is characterized by a dense infiltrate of large cells in the dermis and subcutaneous tissue, separated from the epidermis by a narrow band of collagen called the grenz zone (not observed in the present case). 2,5 Often, this infiltrate tends to be more intense in the deep dermis, called a “bottom-heavy pattern”.2
The positivity of the markers Bcl-2, Bcl-6, MUM1, and FOXP1 is characteristic of this type of lymphoma.1,5 The positivity of C-MYC seems to be related to a worse prognosis.7,8 Other indicators of poor prognosis include lower limb location, multiple injuries, and age over 75 years.6
The treatment of the more aggressive types of CBCL, mainly the leg type, includes chemotherapy with a CHOP regimen (cyclophosphamide, doxorubicin, vincristine, and prednisone). The association of rituximab (R-CHOP) may lead to better results, as observed in this patient, and increased survival.1,2,9 Surgical excision and radiotherapy are among the first-line therapies for solitary lesions. However, due to the high recurrence rates, more recently, the literature recommends treating even solitary and localized lesions with the R-CHOP regimen in the first line, followed by radiotherapy with a safety margin and/or surgery as adjuvant therapies. 9
Considering the rapid growth, the high proliferative index, and the reserved prognosis of diffuse cutaneous large B-cell lymphoma, leg type, we emphasize the importance of knowing its multiple clinical manifestations, especially its classic form in the lower limb, which allows the early diagnosis and adequate treatment, positively impacting patient survival.
Flávia Regina Ferreira 0000 0001 5679 4282
Approval of the final version of the manuscript; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Mariana Oliveira Fernandes 0000 0002 3134 7096
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Marina Thereza Fogo Pereira 0000 0002 3185 4653
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Fernanda da Rocha Gonçalves 0000 0003 2933 2845
Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
1. Sousa NA, Buffara MO, Maia RL, Pessoa AS, Cassia FF, Brotas AM. Linfoma cutâneo primário de grandes células B. Revista SPDV. 2020;78(1):61- 5.
2. Verde ASSL, Marques MVL, Jardim ACM, Damasceno JA, Soares IC. Linfoma cutâneo difuso de grandes células B, tipo perna: relato de caso. J Bras Patol Med Lab. 2021;57:1-5.
3. Rivitti EA. Dermatologia de Sampaio e Rivitti. São Paulo: Artes Médicas; 2018. p. 1282-83.
4. Senff NJ, Hoefnagel JJ, Jansen PM, Vermeer MH, van Baarlen J, Blokx WA, et al. Reclassification of 300 primary cutaneous B-Cell lymphomas according to the new WHO-EORTC classification for cutaneous lymphomas: comparison with previous classifications and identification of prognostic markers. J Clin Oncol. 2007;25(12):1581-7.
5. Hristov AC. Primary cutaneous diffuse large B-cell lymphoma, leg type: diagnostic considerations. Arch Pathol Lab Med. 2012;136(8):876-81.
6. Goyal A, LeBlanc RE, Carter JB. Cutaneous B-Cell Lymphoma. Hematol Oncol Clin North Am. 2019;33(1):149-61.
7. Valera A, López-Guillermo A, Cardesa-Salzmann T, Climent F, González-Barca E, Mercadal S, et al. MYC protein expression and genetic alterations have prognostic impact in patients with diffuse large B-cell lymphoma treated with immunochemotherapy. Haematologica. 2013;98(10):1554-62.
8. Zhou K, Xu D, Cao Y, Wang J, Yang Y, Huang M. C-MYC aberrations as prognostic factors in diffuse large B-cell lymphoma: a meta-analysis of epidemiological studies. PloS one. 2014;9(4):e95020.
9. Lang CCV, Ramelyte E, Dummer R. Innovative therapeutic approaches in primary cutaneous B-Cell lymphoma. Front Oncol. 2020;10:1163.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}