


Iago Gonçalves Ferreira1,2; Livia Giacomet2; Ana Cristina Dornelles1; Renan Minotto1
Submitted on: 24/06/2021
Approved on: 18/08/2021
Financial support: None
Conflict of interest: None
How to cite this article: Ferreira IG, Giacomet L, Dornelles AC, Minotto R. Surgical approach to retronychia refractory to clinical treatments. Surg Cosmet Dermatol. 2022;14:e20220064
Retronychia is an inflammatory onychopathy characterized by the disordered growth and stacking of nail plates, associated with an imbalance in the matrix production of plaques, which tend to overlap. This condition may be associated with trauma, evolving with an inflammatory reaction along the proximal nail fold and granulation tissue formation. We report the case of a patient with retronychia in the left hallux, submitted to surgical treatment after failure of therapeutic responses with previous clinical treatments. The surgical approach led to the avulsion of the overlapping nail plates and the excision of voluminous granulation tissues, achieving adequate postoperative evolution.
Keywords: Nail diseases; Nails; Nails ingrown
Retronychia is an inflammatory onychopathy whose etiopathogenesis is still poorly understood. It is characterized by the disordered growth and overlapping of nail plates, associated with an imbalance in the matrix production of plaques and inflammation in the region of the proximal nail fold.1–3 The term “retronychia” originates from the Latin “retro” (“backward”) and Greek “onychia” (“nail”), being first described by De Berker and Renall in 1999 during the 8th Congress of the European Academy of Dermatology and Venereology.4,5
The primary triggering mechanism of retronychia is nail microtrauma, which causes the nail plate to lose its attachment to the matrix, leading to new matrix production of plaques and the growth of a new blade under the previous one. This rare condition mainly affects the hallux, and factors such as wearing tight, non-malleable shoes and activities associated with repetitive trauma (running, mountaineering, dancing, among others) can precipitate it.2,3,6–8
In refractory to clinical treatments, the surgical approach can be adopted for diagnostic and curative purposes, and it’s performed through the avulsion of the overlapping nail plates and excision of the granulation tissue.3,6,9 This study aimed to describe a surgery technique adopted in the case of retronychia in the hallux.
We report the case of a 35-year-old man, without comorbidities, presenting pain, swelling, and redness in the proximal nail fold and left hallux cuticle, with evolution for about four months. He used antibiotics (cephalexin and amoxicillin) and anti-inflammatory drugs, in addition to topical use of clobetasol, including occlusive mode, fusidic acid, mupirocin, and gentamicin, without improvement. The signs and symptoms arose from the habit of supporting the distal ends of the hallux on the floor while working on the computer at the home office due to the covid-19 pandemic. He denied a similar previous condition and the use of tight shoes, even referring to using flip-flops, socks, or even being barefoot.
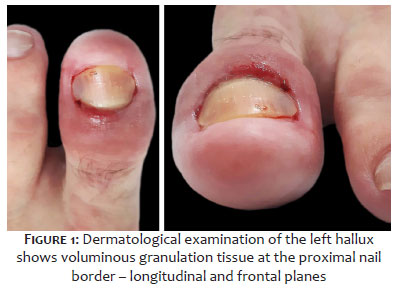
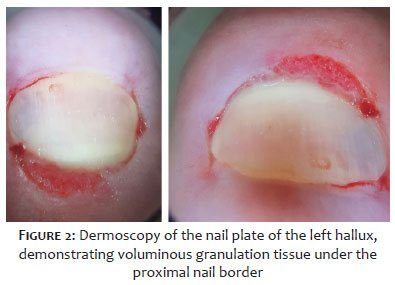
On examination, the nail apparatus of the left hallux showed erythema and an inflammatory aspect of the nail folds, edema and apparent hypertrophy of the hyponychium region, onycholysis, white-yellowish chromonychia, and granulation tissue emerging under the cuticle (Figures 1 and 2).
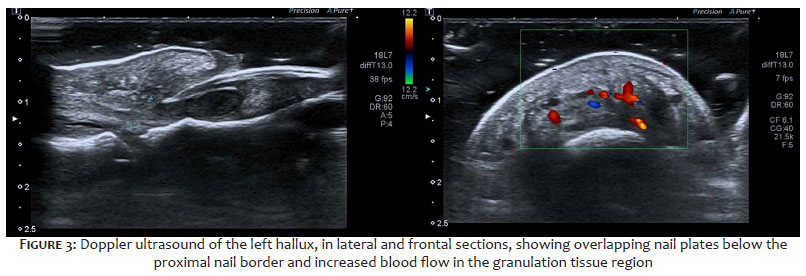
Ultrasonography showed significant thickening of the proximal nail fold and a hypoechoic halo around the nail matrix, associated with disruption of the proximal portion of the ventral nail plate, suggestive of a fragment. No bone remodeling was identified. The Doppler revealed an increase in flow near the proximal nail fold and matrix (Figure 3).
The surgical procedure started with the patient being placed in the supine position, supporting the affected limb, flexed, on padded support, with the sole on the surface of the operating bed. Then, the organization of the operating table, local antisepsis, and placement of surgical drapes were conducted.
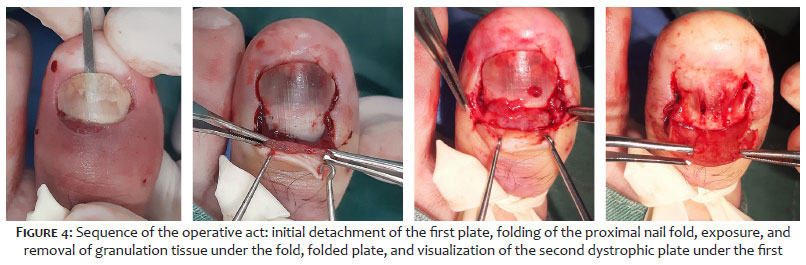
Local anesthesia was performed by anesthetic block (digital, distal, bilateral of the affected hallux) with lidocaine 2% without vasoconstrictor. Subsequently, hemostasis was performed using a number 2 Penrose drain, in a tourniquet, followed by the detachment of the first nail plate and retraction of the proximal nail fold with an electrocautery tip (Figure 4). The detachment of the nail plate evidenced voluminous granulation tissue, which was excised, then proceeding with the removal of the second and third nail plates, in sequence.
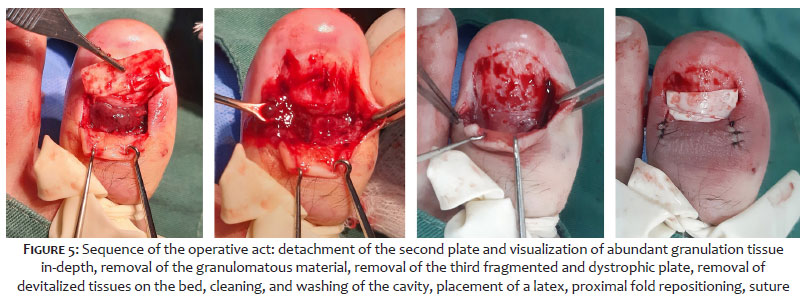
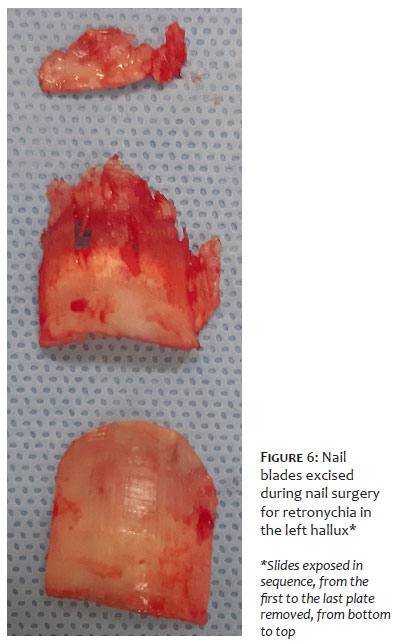
Then, the excision of granulation tissue and inflammatory debris was performed in-depth, with total cleaning of the cavity with saline solution. The proximal nail fold was repositioned with the placement of wide-lumen latex surgical drain, with the distal end advancing over the bed to drain postoperative secretions (Figures 5 and 6). We then proceeded to bilateral suture using 5-0 mononylon and applying a bulky containment dressing with mupirocin, gauze, and crepe bandage. The patient was instructed to perform daily dressings, in addition to the use of antibiotics, anti-inflammatories, and analgesics.
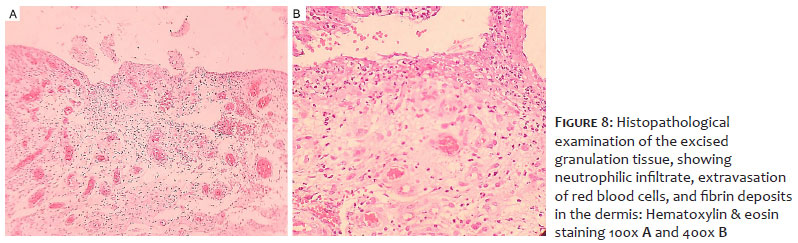
The patient had a good postoperative recovery, with clinical improvement (Figure 7). The anatomopathological examination showed chronic ulcerated inflammation with the formation of exuberant granulation tissue in the nail bed (Figure 8).
We present a case report of retronychia with extensive inflammatory reaction in a young patient, evolving with paronychia and pain in the left hallux. The diagnosis of retronychia is based on clinical manifestations, including paronychia, onychomadesis, chromonychia, reduction and nail growth interruption, and formation of new plaques in conglomerates, in addition to the granulation tissue production, emerging under the nail fold.1–3,6 Also, other nail changes can be observed, such as xantonychia, onycholysis, and subungual hematoma.2,6 Despite the characteristic clinical picture, cases of retronychia are often underdiagnosed, making ultrasound an essential diagnostic resource.2
In this regard, Fernández et al. established diagnostic ultrasound criteria for retronychia: the presence of a hypoechoic halo or band around the origin; distance between the nail plate origin and the distal phalanx base (≥5.1 mm in the hallux and/or difference ≥0.5 mm regarding the contralateral hallux); proximal nail fold thickness (≥2.2 mm for men or ≥1.9 mm for women and/or ≥0.3 mm concerning the contralateral hallux). Thus, the simultaneous presence of three criteria may indicate the diagnosis of unilateral retronychia, and, in bilateral cases, the presence of at least two criteria, one of which is the presence of a hypoechoic halo, may favor the diagnosis.10
In the case reported here, ultrasonography demonstrates the three diagnostic ultrasonographic criteria (increased distance between the nail plate origin and the distal phalanx base; increased proximal nail fold thickness, and a hypoechoic halo below the origin of the plaque). There is also a growth in blood flow in the dermis of the nail fold posterior to Doppler.
Regarding the retronychia treatment, in mild forms, a conservative approach can be adopted, considering that some of these types may spontaneously involute. Conservative therapy includes using adhesive tape and orthoses to fix the “loose” nail plate in the proximal region or applying topical corticosteroids to the proximal nail edge. Topical therapy can act by reducing inflammation and swelling in the proximal nail fold, as observed by Lencastre et al., where topical steroids, associated or not with occlusion, showed a complete or partial clinical response in 41.1% and 28.5% of cases of retronychia, respectively.11 However, despite the clinical improvement, recurrences in these situations are frequent.
Thus, in advanced and/or recurrent cases, the surgical approach is more indicated, promoting the resolution of the condition from the avulsion of the overlapping nail plates and excision of the granulation tissue,1,3,6,7 as performed in the reported case. The histopathological examination is not essential for diagnosis; however, it is recommended that the excised material is sent to pathological analysis to exclude the diagnosis of neoplasms of the proximal nail fold, as conducted in this case.
Concerning the postoperative complications, they involve onychocryptosis, micronychia, onychodystrophy, and periungual tissue hypertrophy.1,3,6,7 Post-surgical recurrence is rare, but it can occur. Therefore, patients should be instructed on preventive measures to avoid triggering factors such as the use of properly sized shoes, correction of orthopedic disorders of the feet, and deviations in nail growth.3,6,9
We described the surgical technique adopted in the case of exuberant retronychia without previous clinical response. We observed an abundant amount of granulation tissue intraoperatively, including under the plates, emphasizing the severity and peculiarity of the case, rarely reported in the literature. It’s noteworthy that the technique described is one of the possible options for the surgical treatment of these cases.
Iago Gonçalves Ferreira 0000-0002-4695-1982
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Livia Giacomet 0000-0001-8474-7002
Approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation critical literature review; critical revision of the manuscript.
Ana Cristina Dornelles 0000-0001-8597-117X
Approval of the final version of the manuscript; study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied case; critical revision of the manuscript.
Renan Minotto 0000-0002-1451-0461
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Ventura F, Correia O, Duarte AF, Barros AM, Haneke E. "Retronychia--clinical and pathophysiological aspects". J Eur Acad Dermatol Venereol. 2016;30(1):16-9.
2. Nagrani N, Castillo DE, Al-Mohanna H, Tosti A. Occupational retronychia: a report of a case in a UPS employee. Skin Appendage Disord. 2019;5(3):169-71.
3. Litaiem N, Drissi H, Zeglaoui F, Khachemoune A. Retronychia of the toenails: a review with emphasis on pathogenesis, new diagnostic and management trends. Arch Dermatol Res. 2019;311(7):505-12.
4. Berker D, Renall J. Retonychia - proximal ingrowing nail. Eur Acad Dermatol Venereol. 1999;12(Suppl 2):S126.
5. Berker DA, Richert B, Duhard E, Piraccini BM, André J, Baran R. Retronychia: proximal ingrowing of the nail plate. J Am Acad Dermatol. 2008;58(6):978-83.
6. Mello CDBF, Souza MDRE, Noriega LF, Chiacchio ND. Retronychia. An Bras Dermatol. 2018;93(5):707-11.
7. Sudy E, Urbina F, Wortsman X. Retronychia. Asian J Res Dermatol Sci. 2018;1(1):1–9.
8. Alonso-Pacheco ML, Miguel-Mendieta E, Maseda-Pedrero R, Mayor-Arenal M. Retronychia: a case report including ultrasound imaging and surgical treatment. Actas Dermosifiliogr. 2016;107(5):e33-7.
9. Gerard E, Prevezas C, Doutre MS, Beylot-Barry M, Cogrel O. Risk factors, clinical variants and therapeutic outcome of retronychia: a retrospective study of 18 patients. Eur J Dermatol. 2016;26(4):377-81.
10. Fernández J, Reyes-Baraona F, Wortsman X. Ultrasonographic criteria for diagnosing unilateral and bilateral retronychia. J Ultrasound Med. 2018;37(5):1201-9.
11. Lencastre A, Iorizzo M, Caucanas M, Cunha N, Trakatelli MG, Zaraa I, et al. Topical steroids for the treatment of retronychia. J Eur Acad Dermatol Venereol. 2019;33(9):e320-22.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}