


Iago Gonçalves Ferreira1,2; Gustavo Bottene Ribolli2; Luyze Homem de Jesus2; Fabiane Cristina Lersch1; Mariele Bevilaqua1
Submitted on: 21/06/2021
Approved on: 18/08/2021
Conflict of interest: None
Financial support: None
How to cite this article: Ferreira IG, Ribolli GB, Jesus LH, Lersch FC, Bevilaqua M. Cutaneous sarcoidosis and facial filling: a possible triggering event? Surg Cosmet Dermatol. 2022;14:e20220063
Sarcoidosis is a systemic granulomatous disease with skin involvement in 10% to 25% of cases. This skin condition has been associated with previous trauma, including the use of skin fillers. We present the case of a patient with an erythematous plaque on the nasal dorsum with 12 months of evolution and a history of previous facial fillings with polymethylmethacrylate and hyaluronic acid. Skin biopsy showed a granulomatous inflammatory process with an epithelioid pattern and multinucleated giant cells, characteristic of cutaneous sarcoidosis. Sarcoidosis can occasionally manifest without systemic involvement and may be associated with the previous use of long-term tissue fillers.
Keywords: Hyaluronic acid; Dermatology; Polymethyl methacrylate; Dermal fillers; Sarcoidosis
Sarcoidosis is a systemic granulomatous disease involving multiple organs – including lungs, lymphatic system, and skin. It has a higher prevalence among adults, black individuals, and women.1 This condition may present cutaneous involvement in about 10% to 25% of cases, occasionally manifesting without associated systemic implication, affecting only the skin.2
The use of cutaneous fillers can cause early adverse events, such as erythema or hematomas,3 or late complications, such as immune-mediated inflammatory disorders and non-infectious granulomatous disorders.4,5 Late granulomatous reactions occur mainly in the form of foreign body granulomas. However, in some rare cases, granulomatous lesions can occur through sarcoid reactions, characterizing cutaneous sarcoidosis (CS).1,5,6 These granulomas do not have well-defined pathophysiology and etiology, and they are associated with skin trauma caused by perforation of cannulas regarding the antigens of the fillers used.1,3,4,7 Given the relevance of complications related to aesthetic procedures, this report aims to discuss a case of CS in a patient with previous skin filling.
A 50-year-old woman patient reported an erythematous plaque on the nasal dorsum with an asymptomatic evolution for about a year and a half. She described a history of previous aesthetic procedures: malar filling with polymethylmethacrylate (PMMA), brand not mentioned, in 2014, and filling of the orbicularis fossa with hyaluronic acid (HA-Emervel Touch® Galderma Brasil, São Paulo, Brasil) 1 ml, in 2018. All procedures occurred with no acute reactions. The patient had no joint pain, respiratory changes, lymphadenopathy, gastrointestinal, cardiological, ophthalmological, or neurological changes.
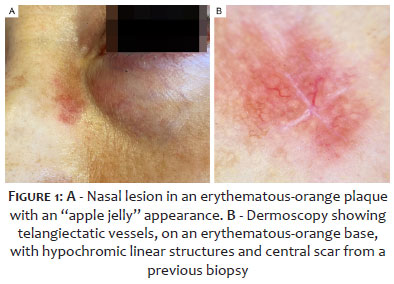
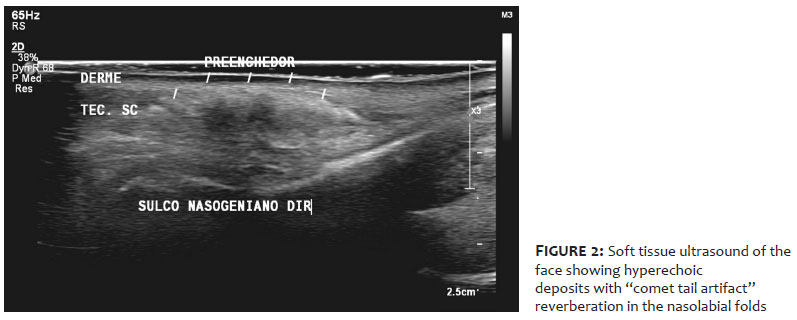
Dermatological examination revealed a well-defined erythematous plaque with an orange background, regular borders, and thin linear vessels at dermoscopy (Figure 1). Complementary investigation showed negative serological markers for rheumatological and infectious diseases. Chest tomography revealed normal parenchyma, with no typical lymph node enlargement. Soft tissue ultrasound revealed hyperechoic deposits with “mini-comet-tail” reverberation artifacts in the region of the nasolabial folds, extending from the height of the mid-nasal third to the labial commissures, suggestive of PMMA deposits in the dermis (Figure 2).
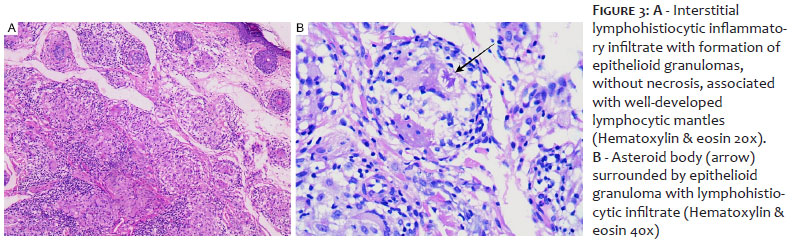
The histopathology of the skin biopsy showed a chronic inflammatory process with the formation of epithelioid pattern granulomas and the presence of multinucleated giant cells in the superficial and deep dermis. There was no evidence of necrosis (Figure 3) and negative AFB, thus confirming the diagnosis of CS.
The application of cutaneous fillers can lead to early and self-limited complications, such as hematomas, edema, and erythema, or late complications, such as the Tyndall effect, surface irregularities, hypersensitivity reactions, or even granulomatous lesions, as CS.6 Among the late complications, CS has occasionally been reported after trauma, cutaneous surgery, and aesthetic procedures, such as venipuncture and injections of fillers, a condition described in the case.7
Although sarcoid-like lesions do not necessarily occur at puncture sites, but also appear in other locations, it is postulated that cutaneous trauma could evidence underlying systemic sarcoidosis and trigger CS in predisposed individuals.1,4 However, other factors may be involved. Etiologic factors have also been associated with CS, such as exposure to insecticides, metals, fungi, drugs, and infection by microorganisms such as Mycobacterium tuberculosis and Herpes simplex virus,1 the latter was also present in the history of this patient, who had recurrent oral herpes.
CS can present several clinical forms, which include spots, papules, lupus pernio, infiltrations in tattoos, or previous scars, as well as psoriasiform, lichenoid, ichthyosiform, and verrucous lesions.1,7 Regarding the plaques, the presentation seen in this case, they tend to reveal diameters smaller than or equal to 1 cm, colorations ranging from red, violet, brown, or even hypopigmentation, affecting extremities, areas of trauma, or the central region of the face, as in the patient.7
It is believed that the pathogenesis of CS is associated with an abnormal immune response to different antigens, of a Th1 pattern, with the involvement of mediators such as interferon-gamma and tumor necrosis factor (TNF), resulting in the formation of non-caseating granulomas.7 Given the morphology similar to other dermatoses, CS is frequently diagnosed through skin biopsies, which should exclude other causes of granulomatous reactions, including foreign body granulomas.8 The histopathology of sarcoidosis reveals epithelioid, non-caseating, well-delimited granulomas of circular shape, located in the dermis.1
Due to their long permanence in tissues, non-biodegradable fillers have been more related to late adverse events, and PMMA is a significant culprit.4 On the other hand, PMMA is a synthetic, biocompatible polymer with antigenic potential, formerly widely used to correct nasolabial folds and glabellar and frontal rhytids.5,9 However, due to late complications related to its use – allergic reactions, formation of foreign body granulomas, and subcutaneous nodules – PMMA has been falling into disuse.9
The occurrence of adverse events with HA reveals lower incidence rates – about 0.05% to 0.15% of cases.1 Biodegradable fillers, such as HA, are less prone to late complications due to their higher biocompatibility and lower immunogenicity.1,6
In this case, it is not possible to say that any of the fillers acted as the primary agent of the sarcoid lesion. However, they may have worked as triggers.
Also, the appearance of CS in the patient’s nasal wall was observed seven years after the application of PMMA and three years after the application of HA. According to Tholken et al., the prolonged time between application and the clinical presentation of the lesions proves to be a positive predictive factor for the diagnosis of isolated CS.1
The therapeutic approach to CS is diverse. In localized forms, topical medications such as corticosteroids (clobetasol, halobetasol, betamethasone), calcineurin inhibitors (tacrolimus and pimecrolimus), retinoids are used, in addition to intralesional corticosteroids (triamcinolone).7 Alternative topical therapeutic options include photodynamic therapy, phototherapy, laser, and surgical excision of lesions. Most treatments show relevant results about two to three months after starting the medications.7 In our patient , we chose topical therapy with mometasone and tacrolimus due to the limited extent of the lesion, achieving significant improvement after six months.
Severe and relapsing cases may require systemic therapy, which includes the use of antimalarials, tetracycline antibiotics, pentoxifylline, apremilast, and retinoids.2,7 Immunobiologicals, such as TNF inhibitors, specifically adalimumab and infliximab, have shown important responses in chronic, recalcitrant, and severe forms of CS, including ulcerative sarcoid lesions, lupus pernio, and forms unresponsive to systemic corticosteroid therapy.7
This case report presents an alert for the emergence of late reactions to cutaneous fillers regarding early identification and prompt treatment establishment. We highlight the importance of differential diagnosis of CS with other dermatoses, given its varied clinical presentations and the appearance of cutaneous sarcoid-like lesions in places that were not necessarily the application sites. Furthermore, the histopathological differentiation between sarcoid granulomas and other granulomatous diseases must be performed, especially foreign body granulomas, often associated with the use of fillers. As seen in the case and reported in the literature, the response to the available therapeutic options has been positive, showing no serious evolution of the conditions.
Iago Gonçalves Ferreira 0000-0002-4695-1982
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Gustavo Bottene Ribolli 0000-0001-7302-6461
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Luyze Homem de Jesus 0000-0002-4200-7310
Author’s contribution: Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Fabiane Cristina Lersch 0000-0003-3590-4344
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Mariele Bevilaqua 0000-0001-5689-1162
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Thölken KFM, Brenner FM, Werner B, Peretti MC, Azevedo LM. Clinical manifestation of systemic sarcoidosis after cutaneous filling. Surg Cosmet Dermatol. 2017;9(4):331–3.
2. Gharavi N, Diehl J, Soriano T. Cutaneous sarcoidosis successfully treated with intralesional 5-Fluorouracil. Dermatol Surg. 2015;41(9):1082-5.
3. Alijotas-Reig J, Fernández-Figueras MT, Puig L. Inflammatory, immune-mediated adverse reactions related to soft tissue dermal fillers. Semin Arthritis Rheum. 2013;43(2):241-58.
4. Broly M, Marie J, Picard C, Demoures A, Raimbault C, Beylot-Barry M, et al. Management of granulomatous foreign body reaction to fillers with methotrexate. J Eur Acad Dermatol Venereol. 2020;34(4):817-20.
5. Friedmann DP, Kurian A, Fitzpatrick RE. Delayed granulomatous reactions to facial cosmetic injections of polymethylmethacrylate microspheres and liquid injectable silicone: a case series. J Cosmet Laser Ther. 2016;18(3):170-3.
6. Lee SK, Kim SM, Cho SH, Lee JD, Kim HS. Adverse reactions to injectable soft tissue fillers: memorable cases and their clinico-pathological overview. J Cosmet Laser Ther. 2015;17(2):102-8.
7. Wanat KA, Rosenbach M. Cutaneous sarcoidosis. Clin Chest Med. 2015;36(4):685-702.
8. Sidwell RU, McL Johnson N, Francis N, Bunker CB. Cutaneous sarcoidal granulomas developing after Artecoll facial cosmetic filler in a patient with newly diagnosed systemic sarcoidosis. Clin Exp Dermatol. 2006;31(2):208-11.
9. Park TH, Seo SW, Kim JK, Chang CH. Clinical experience with polymethylmethacrylate microsphere filler complications. Aesthetic Plast Surg. 2012;36(2):421-6
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}