


João Felipe Rossival-Preto1; Ingrid Stresser-Gioppo2; Flávia Fajardo1; Marina Carrara-Camilo-Barbosa1; Ivander Bastazini-Junior1
Submitted on: 30/05/2021
Approved on: 18/08/2021
Financial support: None
Conflict of interest: None
How to cite this article: Rossival-Preto JF, Stresser-Gioppo I, Fajardo F, Carrara-Camilo-Barbosa M, Bastazini-Junior I. Pemphigus vegetans: surgical approach as a complementary treatment. Surg Cosmet Dermatol. 2022;14:e20220058
Pemphigus vegetans is considered a rare clinical variant of Pemphigus vulgaris and is associated with recurrent lesions that can evolve into extensive vegetative plaques that are difficult to resolve. Surgery may be an alternative in the complementary treatment of lesions resistant to classical therapy. There is a shortage of literature that shows the surgical technique and the postoperative results of the approach to pemphigus vegetans, making the communication of this case relevant. We present the case of a patient with the Hallopeau type of pemphigus vegetans successfully treated with tangential exeresis followed by secondary intention healing of large retroauricular projections.
Keywords: Pemphigus; Dermatologic surgical procedures; Treatment outcome
Pemphigus is a group of diseases that manifest with blistering lesions on the skin and/or mucosa and differ among them according to their clinical, histopathological, and etiological characteristics.1 Pemphigus vegetans is a clinical variant of pemphigus vulgaris considered the rarest, representing about 1% to 2% of all cases of pemphigus.2
The literature describes two subtypes of pemphigus vegetans: the Hallopeau, a mild form that, at first, is characterized by pustular lesions that erupt, fuse, and gradually evolve into vegetative erosions that expand centrifugally; and Neumann’s, a more recalcitrant type, which usually starts with vesicles and blisters similar to pemphigus vulgaris, but they erupt and form vegetative exudative masses and hypertrophic erosions.1,3
The treatment of pemphigus vegetans is similar to that of pemphigus vulgaris and includes the remission-inducing phase of the lesions and the maintenance phase. It is often prolonged, lasting, on average, five to 10 years. Some lesions, however, may be refractory to the initial treatment, requiring another type of procedure for their resolution,1,4 such as surgical approach.
We report the case of a 62-year-old man who was initially followed up in the Dermatology Department due to pemphigus vulgaris. The lesions later evolved with retroauricular and forehead pustules that culminated in the local appearance of vegetating, papillomatous, well-defined, and irregular plaques, in addition to erosive lesions in seborrheic areas on the back and thorax. Considering the clinic, the results of the biopsies for anatomopathological study, and the direct immunofluorescence exam with a deposit of intercellular IgG in the epidermis, we defined the diagnosis of pemphigus vegetans, Hallopeau subtype. Remission of lesion activity was achieved with the use of dexamethasone and dapsone (remaining stable with a reduced and continuous dose of dexamethasone 0.75 mg every other day and dapsone 100 mg daily). However, residual vegetative plaques persisted. We tried adjuvant therapy with serial triamcinolone acetonide injections, with some improvement of the lesions on the forehead, but no regression of the retroauricular plaques. Noting the refractoriness of the vegetating plaques with the therapy, the stability of the lesions, and the patient’s frustration with the disfiguring appearance in the retroauricular region, we chose a surgical approach (Figure 1).
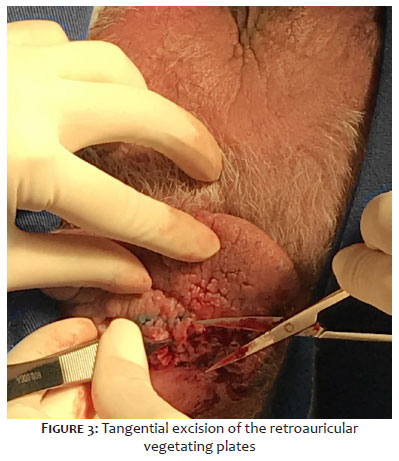
We performed tangential excision followed by electrocoagulation of the base of the lesions under local anesthesia and healing by secondary intention (Figures 2, 3, and 4). The patient had a good evolution, with no recurrence of the lesions (Figure 5).
Classically, the use of systemic corticosteroids is recommended to treat pemphigus vulgaris and, consequently, pemphigus vegetans. Immunomodulatory, immunosuppressive, or immunobiological drugs can be used to mitigate the adverse events of corticosteroid therapy and contribute to controlling the recalcitrant lesions. After controlling the activity of the condition, periodic reassessment and treatment are maintained with the minimum dosage of medications necessary to keep the inactive disease until, if possible, they are weaned.
However, hypertrophic vegetations of pemphigus vegetans may persist, and the use of extracorporeal photopheresis and carbon dioxide laser as effective alternatives are recommended. More recently, the literature has described skin grafting as an option. Intralesional corticosteroid infiltration is also mentioned, although suggested for more localized forms.2
The literature does not explore much the surgical approach of the lesions. A search in the PubMed database using the terms “Pemphigus Vegetans Surgery”, without adding filters, found 35 results, but no studies with perioperative images of the surgical approach to vegetating lesions. More studies focusing on the surgical technique and postoperative outcomes are needed for this treatment modality to gain more space in the clinical practice of dermatologists who treat pemphigus vegetans.
Surgery for this type of lesion involves complications due to the disease itself and the prolonged use of corticosteroids, such as delayed wound healing and risk of infection.5 It is proposed to meet the criterion of stable disease and vegetating lesions that do not regress with other treatments. Also, a good postoperative follow-up is necessary.
The authors advocate that surgery should be more widely used as a form of treatment for cases with aesthetic and functional impairment, given the impact it can have on patients’ quality of life and well-being. The procedure can be performed under local anesthesia, followed by healing by secondary intention, with satisfactory aesthetic results. Compared to other modalities described for unsightly lesions, such as CO2 laser and grafting, it is a lower-cost therapy, widely available, with a postoperative period well tolerated by the patient.
We concluded that surgery proved to be a safe and viable option for managing refractory disfiguring lesions, extending to those that may generate functional impairment.
João Felipe Rossival-Preto 0000-0002-7883-1555
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Ingrid Stresser-Gioppo 0000-0001-9520-7888
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Flávia Fajardo 0000-0002-8239-8440
Data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Marina Carrara-Camilo-Barbosa 0000-0001-8906-0242
Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Ivander Bastazini-Junior 0000-0003-0300-1263
Approval of the final version of the manuscript; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Porro AM, Seque CA, Ferreira MCC, Enokihara MMSS. Pemphigus vulgaris. An Bras Dermatol. 2019;94(3):264–78.
2. Zaraa I, Sellami A, Bouguerra C, Sellami MK, Chelly I, Zitouna M, et al. Pemphigus vegetans: a clinical, histological, immunopathological and prognostic study. J Eur Acad Dermatol Venereol. 2011;25(10):1160-7.
3. Ruocco V, Ruocco E, Caccavale S, Gambardella A, Lo Schiavo A. Pemphigus vegetans of the folds (intertriginous areas). Clin Dermatol. 2015;33(4):471-6.
4. Son YM, Kang HK, Yun JH, Roh JY, Lee JR. The neumann type of pemphigus vegetans treated with combination of dapsone and steroid. Ann Dermatol. 2011;23(Suppl 3):S310-3.
5. Motomura H, Tsuruta D, Yamanaka K, Imanishi H, Harada T, Ishii M. The use of test skin grafting in pemphigus vegetans. J Plast Reconstr Aesthet Surg. 2009;62(11):e506-8.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}