


Flavia de Oliveira Valentim; Anna Carolina Miola; Hélio Amante Miot
Submitted on: 21/09/2021
Approved on: 16/11/2021
Financial support: None
Conflict of interest: None
How to cite this article: Valentim FO, Miola AC, Miot HA. Low-grade fibromyxoid sarcoma: important differential diagnosis in acral tumor lesions. Surg Cosmet Dermatol. 2022;14:e20220094
Low-grade fibromyxoid sarcoma (LGFS) is a rare, indolent spindle cell sarcoma with a risk of recurrence and metastasis. We report the case of a 34-year-old man with a tumor in his thumb that had recurred after excision eight years ago, with slow and progressive growth. The pathological examination was suggestive of SFBG, and we proceeded with the disarticulation of the phalanx. The patient remains in follow-up, with no evidence of metastases. Although rare, it is essential to recognize the diagnosis of an LGFS with its potential risk of recurrences and metastases, especially as a differential diagnosis of acral soft tissue tumors.
Keywords: Dermatology; Neoplasms; Sarcoma
Low-grade fibromyxoid sarcoma (LGFS) is a rare, slow-growing spindle cell sarcoma that tends to affect young adults and is common in the trunk and proximal extremities.1 Despite an indolent clinical course, LGFS can progress to local recurrence and metastasis, most commonly to the lungs.2 We report a rare case of LGFS in the thumb and its treatment.
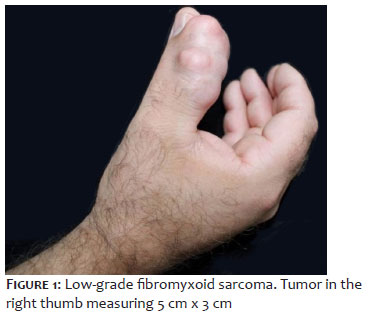
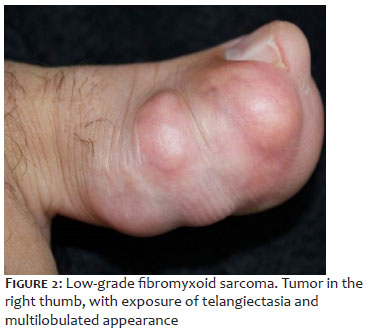
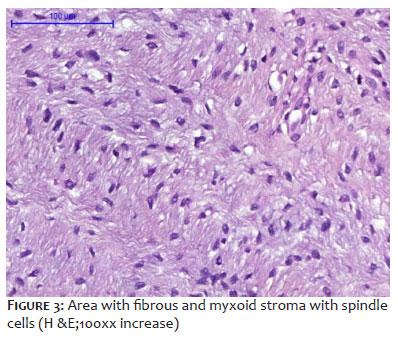
A 34-year-old male farmer with no comorbidities presented a slow-growing, painless, 5-cm-diameter tumor, which was excised at the beginning of the condition but had local recurrence after eight years. Dermatological examination revealed a hardened, adherent tumor with a multilobulated appearance and visible telangiectasias on the right thumb (Figures 1 and 2). The biopsy revealed spindle cell mesenchymal neoplasm with cytological atypia, but without relevant mitotic activity or necrosis, distributed in collagenous and myxoid areas in the dermis (Figure 3), suggesting the diagnosis of LGFS. Magnetic resonance imaging (MRI) detected a mass measuring approximately 5 cm x 3 cm, well delimited, lobulated, proximal to the long flexor tendon. We conducted a wide resection with disarticulation at the level of the metacarpophalangeal joint. Pathological examination confirmed the diagnosis of low-grade fibromyxoid sarcoma with free margins. The patient did not present metastases or recurrence after six months of follow-up.
Low-grade fibromyxoid sarcoma (LGFS) is a rare, slow-growing spindle cell sarcoma that affects young adults.1 Despite its indolent clinical course, LGFS is a distinct variant of fibrosarcoma,1 and it can progress to local recurrence and metastasis, particularly in the long term.2 Most cases of LGFS have been shown to harbor a common t(7;16) (q34;p11) translocation, producing a gene called FUS/GREB3L2, which is characteristic of LGFS but with uncertain significance.3 Clinically, it is a deep, painless, well-defined mass, more common in the trunk or lower limbs.
It has been reported in numerous anatomical sites, such as the head, neck, heart, and kidney.1,4,5 However, the acral location is atypical. In a review, it was possible to find 24 cases of acral LGFS, two of them involving a phalanx or nail.6
Diagnostic confirmation requires an incisional biopsy, and anatomopathological examination shows alternating myxoid areas with fibrous sites and slightly pleomorphic cells, low or moderate cellularity, and absence of mitotic figures or necrosis. Fine needle aspiration, in turn, can make diagnosis challenging, as the findings overlap with other myxoid lesions.7,8 Immunohistochemistry can be positive for vimentin and other markers, such as Bcl-2, EMA, and CD99, but without specificity.1 Magnetic resonance imaging (MRI) can determine the surgical area and assess local infiltration and/or metastasis without pathognomonic findings.9 The common differential diagnoses are desmoid fibromatosis, nodular fasciitis, perineurioma, neurofibroma, myxoma, and ossifying fibromyxoid tumor.1
Treatment consists of complete excision of the lesion, which can be challenging depending on the location. There is no need for adjuvant therapy. However, there is a risk of recurrence or metastasis,6 characteristics that justify long-term follow-up.
LGFS in acral sites is uncommon and may delay diagnosis and proper management. It is essential to recognize and include LGFS in the differential diagnosis of tumors involving acral areas due to its ability to progress to late recurrences and metastases.
Flavia de Oliveira Valentim 0000-0002-1600-3519
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Anna Carolina Miola 0000-0001-8926-734X
Approval of the final version of the manuscript; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Hélio Amante Miot 0000-0002-2596-9294
Approval of the final version of the manuscript; study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Mohamed M, Fisher C, Thway K. Low-grade fibromyxoid sarcoma: clinical, morphologic and genetic features. Ann Diagn Pathol. 2017;28:60–7.
2. Evans HL. Low-grade fibromyxoid sarcoma: a clinicopathologic study of 33 cases with long-term follow-up. Am J Surg Pathol. 2011;35(10):1450-62.
3. Reid R, Silva MV, Paterson L, Ryan E, Fisher C. Low-grade fibromyxoid sarcoma and hyalinizing spindle cell tumor with giant rosettes share a common t(7;16)(q34;p11) translocation. Am J Surg Pathol 2003;27:1229–36.
4. Mendoza AS, O'Leary MP, Peng SK, Petrie BA, Li AI, French SW. Lowgrade fibromyxoid sarcoma of the sigmoid colon. Exp Mol Pathol 2015;98(2):300-3.
5. Chen N, Gong J, Nie L, et al. Primary intracranial low-grade fibromyxoid sarcoma with FUS gene rearrangement. Neuropathology. 2015;35(4):348-53.
6. Saab-Chalhoub MW, Al-Rohil RN. Low-grade fibromyxoid sarcoma of acral sites: case report and literature review. J Cutan Pathol. 2019;46(4):271–6.
7. Domanski HA, Mertens F, Panagopoulos I, Åkerman M. Low-grade fibromyxoid sarcoma is difficult to diagnose by fine needle aspiration cytology: a cytomorphological study of eight cases. Cytopathology. 2009;20(5):304–14.
8. Evans HL. Low-grade fibromyxoid sarcoma: a clinicopathologic study of 33 cases with long-term follow-up. Am J Surg Pathol. 2011;35(10):1450-62.
9. Chetverikova E, Kasenõmm P. Low-Grade fibromyxoid sarcoma of the lateral skull base: presentation of two cases. Case Rep Otolaryngol. 2019:7917040.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}