


Rafael Everton Assunção Ribeiro da Costa1; Fergus Tomás Rocha de Oliveira1; Eugênio de Sá Coutinho Neto2; Carlos Eduardo Coelho de Sá3
Submitted on: 12/08/2021
Approved on: 27/08/2021
Financial support: None
Conflict of interest: None
How to cite this article: Costa REAR, Oliveira FTR, Coutinho Neto ES, Sá CEC. Primary cutaneous adenoid cystic carcinoma in the scalp with pulmonary metastases: a case report. Surg Cosmet Dermatol. 2022;14:e20220085.
Primary cutaneous adenoid cystic carcinoma (PCACC) is a rare tumor with an estimated incidence rate of 0.23 cases/1,000,000 people per year. A 60-year-old man presented a scalp lesion in 2017. Initially, it was not possible to perform a histopathologic diagnosis. In 2018, surgical biopsy and immunohistochemistry of the local skin recurrence indicated a diagnosis of PCACC (treatment was surgery and radiotherapy). In 2020, a new local tumor recurred and was surgically resected. The patient had systemic metastases (pulmonary metastases) and underwent chemotherapy. Currently, the pulmonary metastases are stable. The PCACC has progressed to pachymeninges.
Keywords: Carcinoma adenoid cystic; Scalp; Neoplasm metastasis; Skin neoplasms
Adenoid cystic carcinoma (ACC) is a rare cancer that commonly originates from the salivary glands and may also arise from lacrimal, sweat, and Bartholin glands. Although its clinical course is slow, there is a tendency for an early invasion of blood vessels and peripheral nerves, which causes a high rate of local recurrence and metastases, especially to the lungs, bones, and liver, resulting in a worse prognosis.1
Primary cutaneous adenoid cystic carcinoma (PCACC) is an extremely rare type of ACC. A 30-year epidemiological study of PCACC estimated an incidence rate of 0.23 cases per million people per year.2 A recent survey of PCACC cases showed a total of only 114 cases reported in the English-language literature.3 PCACC presents a lower degree of malignancy among ACCs, and the occurrence of metastases is very infrequent, despite the high incidence of local recurrence.4
Given the rarity of metastatic PCACC and the scarcity of literature on the subject, this study aims to describe a case of PCACC in the scalp with lung metastases.
In April 2017, a 60-year-old man arrived at the Service with a small lesion on the scalp (<1.0 cm). The lesion presented a rough surface and a light brown color, located in the region corresponding to the posterior part of the sagittal suture, with bilateral involvement of the temporal bones. The surgical resection, biopsy, and anatomopathological study indicated it was a neoplasm with characteristics of malignancy, without the possibility of histopathologic diagnosis.
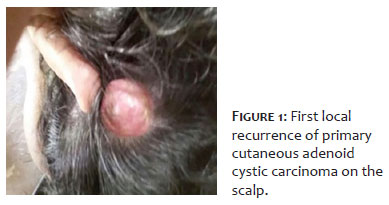
The patient presented an erythematous-violaceous nodule, with fibroelastic consistency, measuring 1.2 cm on the scalp, compatible with local recurrence of the primary lesion, in March 2018 (Figure 1). Magnetic resonance imaging (MRI) indicated a lobulated diplopic lesion with heterogeneous enhancement in the posterior portion of the sagittal suture, partially involving the superior sagittal sinus and with intra and extracranial extension.
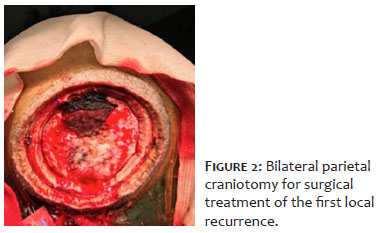
We decided to perform a bilateral parietal craniotomy. Figure 2 shows the surgical field after the removal of the parietal bones. Biopsy and anatomopathological study were performed, in addition to immunohistochemistry, and the results were compatible with PCACC in the scalp, with bone infiltration (p63 and CD117 positive). The patient was referred for adjuvant radiotherapy for three months (total dose of 50 Gy in 20 applications) and periodic clinical follow-up.
In March 2020, the patient presented a new lesion on the scalp. MRI showed signs of surgical manipulation characterized by bilateral median and paramedian parietal craniotomy and an extra-axial expansive lesion, with intense uptake by homogeneous contrast in the right parietal region, underlying the craniotomy. It suggested a recurrence of 2.1 cm, promoting an impression on the right parietal lobe without changing its sign. Brain parenchyma showed preserved morphology and signal intensity. A new bilateral parietal craniotomy was performed in July 2020, with no indication for radiotherapy due to the high risk of brain parenchyma necrosis.
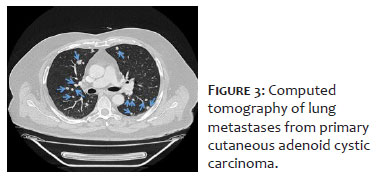
In November 2020, chest computed tomography showed multiple irregular pulmonary nodules in both lungs, the largest measuring 1.1 cm, and 1.3 cm, compatible with neoplastic metastases. Figure 3 depicts the most eminent nodules.
In January 2021, adjuvant chemotherapy with cisplatin and 5-fluorouracil was started, with some adverse events (headache, nausea, and vomiting). Currently, the lung metastases are stable, and the patient is on a chemotherapy pause. However, there was a progression from PCACC to pachymeninges. The case was sent to the Neurosurgery team to study the possibility of a new craniotomy.
The Research Ethics Committee of the State University of Piauí, Teresina (PI), Brazil, approved the present study under CAAE n. 44847121.1.0000.5209. All precepts contained in resolution 466/12 of the National Health Council and international documents were respected.
There are few conclusive studies in the literature on PCACC’s clinicopathological aspects and survival due to its rarity, and there is still no consensus on a standard treatment to be adopted in these cases.
Behbahani et al. published perhaps the more extensive study on PCACC in 2020, including 201 patients diagnosed between 2004 and 2016.5,6
The survival analysis performed by Behbahani et al. showed an overall 5-year and 10-year survival rate of 87.0% and 76.0%, respectively. The same study also showed a mean age at diagnosis of 57.7 years and a higher occurrence of PCACC in women (57.7% of the 201 cases). Also, the primary tumor site was the ear (58.2%), followed by the scalp/neck (25.9%). Most cases were localized tumors (65.8%).6
In addition to PCACC rarity, the patient in this study presented a series of discrepancies regarding what is expected in a case of this nature. First, PCACC is far less common in men, occurring less frequently on the scalp. Furthermore, PCACC tends to have a much less aggressive course than other types of ACC, showing good overall survival rates with a predominance of localized cases.1-6
Regarding treatment, although there is still no consensus, the chief modality adopted is local surgical resection, and radiotherapy is also widely used.6 In this case, we performed surgical resection and radiotherapy. However, there were local recurrences and, later, systemic recurrence (pulmonary metastases). The patient underwent chemotherapy achieving stability of the metastatic neoplastic disease in the lungs. However, PCACC continued to progress locally, affecting pachymeninges.
A 60-year-old man presented a rare case of PCACC on the scalp, with a very aggressive course. Surgical treatment was performed in combination with radiotherapy, with a 4-year follow-up. However, the patient had local recurrences and lung metastases and underwent chemotherapy. Currently, the patient has stable metastatic neoplastic disease in the lungs, but PCACC has progressed locally to pachymeninges.
We thank the Macroregional Hospital of Caxias Dr. Everaldo Ferreira Aragão for the institutional support.
Rafael Everton Assunção Ribeiro da Costa 0000-0002-0798-890X
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Fergus Tomás Rocha de Oliveira 0000-0001-6869-9709
Approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Eugênio de Sá Coutinho Neto 0000-0002-0806-3933
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Carlos Eduardo Coelho de Sá 0000-0002-9610-8010
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Andreasen S. Molecular features of adenoid cystic carcinoma with an emphasis on micro RNA expression. APMIS. 2018;126(Suppl 140):7-57.
2. Dores GM, Huycke MM, Devesa SS, Garcia CA. Primary cutaneous adenoid cystic carcinoma in the United States: incidence, survival, and associated cancers, 1976 to 2005. J Am Acad Dermatol. 2010;63(1):71-8.
3. Prieto-Granada CN, Zhang L, Antonescu CR, Henneberry JM, Messina JL. Primary cutaneous adenoid cystic carcinoma with MYB aberrations: report of three cases and comprehensive review of the literature. J Cutan Pathol. 2017;44(2):201-9.
4. Morrison AO, Gardner JM, Goldsmith SM, Parker DC. Primary cutaneous adenoid cystic carcinoma of the scalp with p16 expression: a case report and review of the literature. Am J Dermatopathol. 2014;36(9):e163-6.
5. Yumeen S, Mirza FN, Mirza HN, Ko CJ, Cohen JM. Primary cutaneous adenoid cystic carcinoma: characterizing US demographics, clinical course, and prognostic factors. J Am Acad Dermatol. 2021;85(1):245-7.
6. Behbahani S, Wassef DW, Povolotskiy R, Pinto J, Joseph N, Paskhover B. Analysis of characteristics and survival of primary cutaneous adenoid cystic carcinoma of the head and neck. Ann Otol Rhinol Laryngol. 2021;130(1):12-7.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}