


Rogerio Nabor Kondo; Gabriela Bernardi Maia; Leticia Amstalde Bertoncini
Financial support: None
Conflict of interest: None
Submitted on: 07/05/2021
Approved on: 23/08/2021
How to cite this article: Kondo RN, Maia GB, Bertoncini LA, Silva ST. Snail flap as an option to reconstruct a nasal defect: a series of two cases. Surg Cosmet Dermatol. 2022;14:e20220043
Basal cell carcinoma (BCC) is the most common skin cancer. When located in the nasal region, reconstructing the defect resulting from its exeresis can become very challenging for the dermatological surgeon. The snail flap (SF) technique can be used to correct defects, mainly on the nose’s lateral wall, but we use it in a modified way to close the nasal wing injury. In both cases, the results were satisfactory, cosmetically and functionally.
Keywords: Carcinoma basal cell; Surgical flaps; Nose
Basal cell carcinoma (BCC) is the most common type of skin cancer.1 Sometimes, complete excision of this type of tumor requires a flap to close the resulting defect, especially those larger than 10 mm.1,2 Reconstructions in the nasal region are challenging for dermatological surgeons due to their local characteristics, such as rigid structure and little mobility.3
The snail flap (SF) is a rotation flap in which part of the pedicle makes a folding movement over itself, resembling a snail shell. It is generally used to correct circular defects in the lower nasal wall, where the adjacent skin above and laterally to the defect is used to provide higher mobility to the flap.4
We report two cases who underwent reconstruction with SF after excision of nasal BCC: one patient had a lesion in the nose’s lower lateral wall (where the flap is most often used), and the other presented a lesion in the nasal wing (where it’s rarely performed). Both had a satisfactory aesthetic result. This study aims to exemplify the SF and demonstrate an option of the technique to correct defects in the nasal wing, with easy execution and a good level of patient satisfaction.
Two patients with BCC in the nasal region were treated:
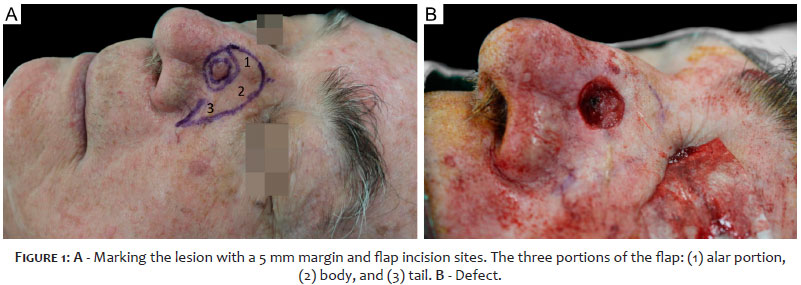
Patient 1: A 80-year-old man, skin phototype III, from Londrina (PR), presented a pearly plaque, 12 mm x 9 mm, on the lower left lateral dorsum of the nasal region, compatible with BCC by biopsy. The lesion was excised with safety margins of 5 mm. The resulting defect was 17 mm in the longest axis, and RC was chosen (Figures 1, 2, and 3).
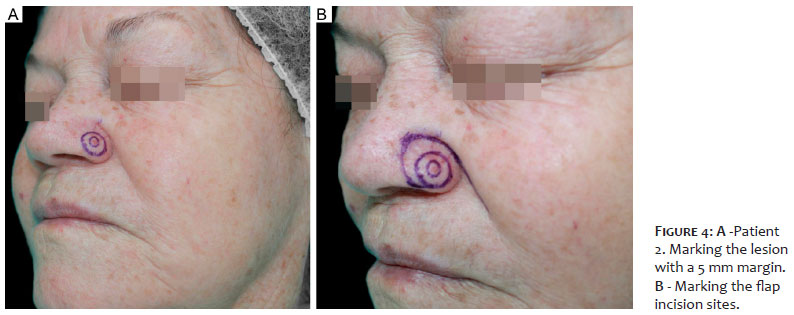
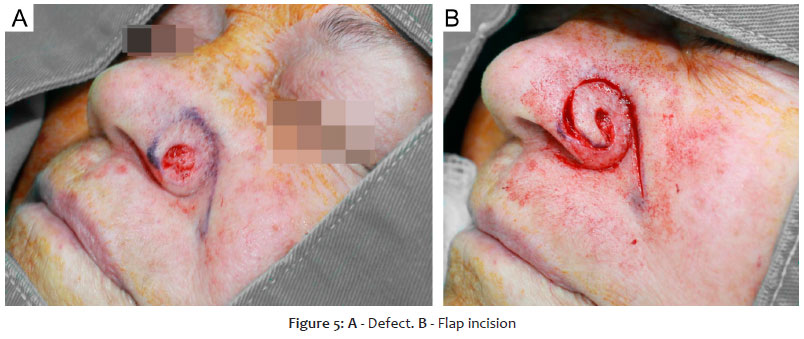
Patient 2: A 73-year-old woman, skin phototype III, from Londrina (PR), presented an erythematous plaque, 6 mm x 5 mm, in the nasal wing to the left of the nasal region, compatible with BCC by biopsy. The lesion was excised with safety margins of 5 mm. The resulting defect was 11 mm in the longest axis, and RC was chosen (Figures 4, 5, and 6).
Description of the technique used for Patient 1: (Figures 1 and 2):
A) Patient in horizontal supine position;
B) Marking with methylene blue or surgical pen of the lesion with a 5 mm margin and flap incision sites: an arch starting from the defect in its upper portion and extending to the homolateral nasogenian groove. From there, a retrograde incision (back-cut) was performed. This flap had three portions: (1) alar, (2) body, and (3) the tail (Figure 1A).
C) Antisepsis with topical 10% polyvinyl iodine;
D) Placement of surgical drapes:
E) Infiltrative anesthesia with 2% lidocaine and vasoconstrictor;
F) Lesion incision using blade 15 and round block excision of the piece;
G) Hemostasis;
H) Flap incision, starting from the defect, making an arc in its upper position, passing through the malar region to the nasogenian groove (as previously marked). From that point, a retrograde incision was made;
I) Flap detachment;
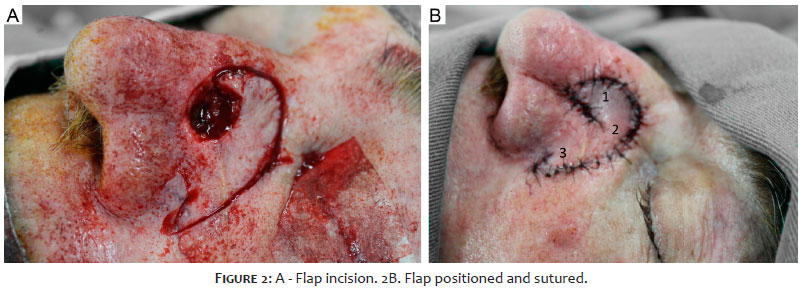
J) Positioning the flap and other sutures with 5.0 mononylon, using single stitches. The alar portion folds over itself (with a “curled” aspect), resembling a snail shell (Figures 2A and 2B);
K) Local cleaning with saline;
L) Occlusive dressing.
Description of the technique used for Patient 2 (Figures 4, 5 6A):
The differences between the techniques of patients 1 and 2 are in items b, h, and j (the sequences described above: a, c, d, e, f, g, i, k, and l of the two techniques remained the same).
B) Marking with methylene blue or surgical pen of the lesion with a 5 mm margin and incision sites of the flap: an arch starting from the lower region of the defect, outlining it in a spiral until the homolateral nasogenian groove in a retrograde incision (Figures 4 and 5);
H) Flap incision, starting from the lower region of the defect, making a spiral arch up to the nasogenian groove (as previously marked);
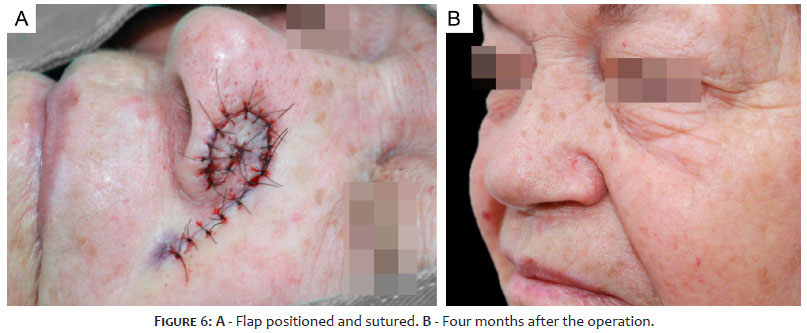
J) Positioning the flap and other sutures with 5.0 mononylon, using single stitches. The portion proximal to the defect folds over itself (with a “curled” aspect), resembling a snail shell (Figures 4B, 5B and 6A).
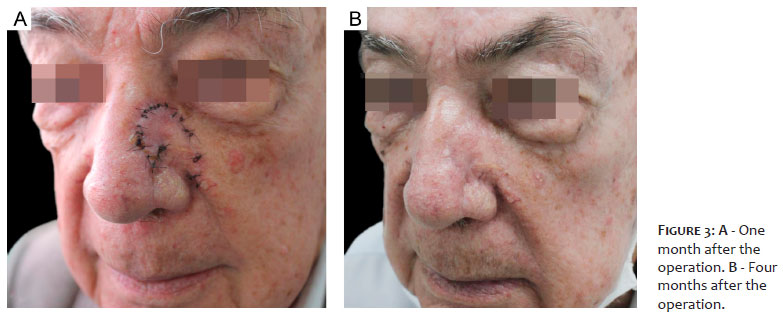
Patient 1: The patient evolved uneventfully in the first postoperative days. There was good healing and accommodation, with a satisfactory aesthetic result in the late postoperative period (Figure 3B).
Patient 2: The patient evolved uneventfully in the immediate postoperative period. There was good healing and accommodation, with a satisfactory aesthetic result in the late postoperative period (Figures 6A and 6B).
SF is a rotation flap technique, but it can also be considered an “island” flap as it maintains vascularization in its central region. It is used to correct circular defects in the lower nasal wall, and it is considered a good alternative for nasolabial interpolation since it can be performed in a single surgical time.4
FS is neither exclusive to the nasal wall nor restricted to the nose area. When applying a flap that folds over itself, resembling a snail shell, it is an SF. Christopoulos et al. described an SF technique for reconstructing scalp defects,5 and Aksu et al. used it for the external auditory canal.6
In the case of patient 1, we performed the classic SF. We incised an arch that started from the upper region of the defect to the homolateral nasogenian sulcus, and, from that point on, we made a backward cut incision. This flap had three portions: (1) alar, (2) body, and (3) tail. The alar portion reconstructed the alar region of the defect and was the same size as that area. The flap’s body and tail were the same size as the vertical dimension of the entire defect and covered the old position of the alar portion4 (Figures 1A and 2B).
In the case of patient 2, we applied the modified SF to the nasal wing defect. The beginning of the flap incision was in the lower region, making an arch almost parallel to the defect for better accommodation, so there was no lifting of the nasal wing. Not only the end of the flap fold over itself, but nearly half of it spiraled (Figures 5B and 6A)
The reason why SF is rarely used in the nasal wing region may be due to other existing techniques (grafting, advancement island flaps, transposition). In addition, if the SF is made in the same proportions and incisions as its classic model (that is, without being modified), it can cause local deformities, such as lifting the nasal ala.
In addition to the nasal wall (patient 1), another location where SF could be applied would be the nasal ala (patient 2). The technique for this last location differs from the first in that it uses practically half of the flap (not just the end) to fold over itself. For better results, the present authors advise not to perform surgical defects larger than 15 mm, due to the risk of alar nasal anatomical distortion.
SF can be a good option for resolving defects in the lateral wall and nasal wing regions.
Rogerio Nabor Kondo 0000-0003-1848-3314
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Gabriela Bernardi Maia 0000-0002-3730-8207
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Leticia Amstalde Bertoncini 0000-0002-4687-8332
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Suellen Tormina da Silva 0000-0003-1175-0571
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
1. Kondo RN, Gon AS, Pontello Junior R. Recurrence rate of basal cell carcinoma in patients submitted to skin flaps or grafts. An Bras Dermatol. 2019;94(4):442-5.
2. Kondo RN, Pontello Junior R. A-T flap for the reconstruction of an operative wound in the malar region. Surg Cosmet Dermatol. 2015;7(3):272-4.
3. Nicolacópulos T, Kondo RN. Retalho A-T para reconstrução de ferida operatória na ponta nasal. Cosmet Dermatol. 2018;10(2):165-7.
4. Brodland DG. Flaps. In: Bolognia JL, Jorizzo JL, RapiniRP, editors. Dermatology. 4th ed. New York: Elsevier; 2018. p.2496-2516.
5. Christopoulos G, Deraje V, Mbaidjol Z, Kannan RY. The "Snail Flap": A rotation flap in scalp reconstruction. Plast Reconstr Surg Glob Open. 2020;8(1):e2599.
6. Aksu AE, Uzun H, Calis M, Safak T. Reconstruction of external auditory canal with a laterocervical twisted (snail) flap. J Craniofac Surg. 2013;24(3):e224-6.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}