


Adma Silva de Lima1; Marina Gubert2; Thaise Lyra2; Carolina Fissmer Sardagna2
Financial support: None
Conflict of interest: None
Submitted on: 04/04/2021
Approved on: 09/11/2021
How to cite this article: Lima AS, Gubert M, Lyra T, Sardagna CF. Muscle contraction patterns and their associations in the upper third of the face: a clinical and epidemiological study. Surg Cosmet Dermatol. 2022;14:e20220024
INTRODUCTION: The use of botulinum toxin has become one the essential cosmetic procedures performed in the world.
OBJECTIVE: To identify patterns of muscle contraction of the forehead, glabellar complex, and orbicularis oculi muscle in patients from southern Brazil, establishing their epidemiology and possible associations between them.
METHODS: One hundred and one patients who sought treatment with botulinum toxin for the forehead, glabella, and periocular lines between 2012 and 2016 were included. Analyzes were made using digital photographs taken during a medical consultation before applying the products., The subjects received with different brands of botulinum toxin, according to the patients’ or the doctors’ preference
RESULTS: The most common contraction patterns were complete frontal, glabellar in converging arrows, and complete periocular. Women represented 94.1% of patients. Most patients were between 31 and 50 years old, with an average of 44.57 years. More frequent patterns in each area were more frequently associated.
CONCLUSIONS: The study shows the main muscle contraction patterns of the upper third of the face in 101 patients, as well as their clinical characteristics, comparing them with previously published articles. Studies on muscle contraction patterns can assist in the safer and more rational use of the products available, avoiding waste and complications.
Keywords: Muscle contraction; Skin aging; Face; Facial muscles; Botulinum toxins type A
Botulinum toxin (BT) for therapeutic and aesthetic purposes has constantly increased in recent decades. It has become one of the most critical aesthetic procedures performed in many countries. Obtained from Clostridium botulinum, a bacterium known to cause botulism, this toxin has seven subtypes, of which type A is the most potent.1–3 BT acts by blocking the release of acetylcholine from the presynaptic terminal of the neuromuscular junction, preventing muscle contraction.3
Different authors have described population patterns of glabellar, periocular, and forehead contractions in recent years.4-7 The description of these patterns contributed to a better understanding of the local anatomy, guiding the rational use of available products, avoiding complications resulting from inadequate applications or dosages, and, finally, optimizing the use in the indicated areas.
The primary objective of this study was to identify the contraction patterns of the forehead, glabellar complex, and orbicularis oculi muscle in a population of patients in southern Brazil. The secondary objectives were to assess possible associations between different contraction patterns and establish an epidemiological profile of this population.
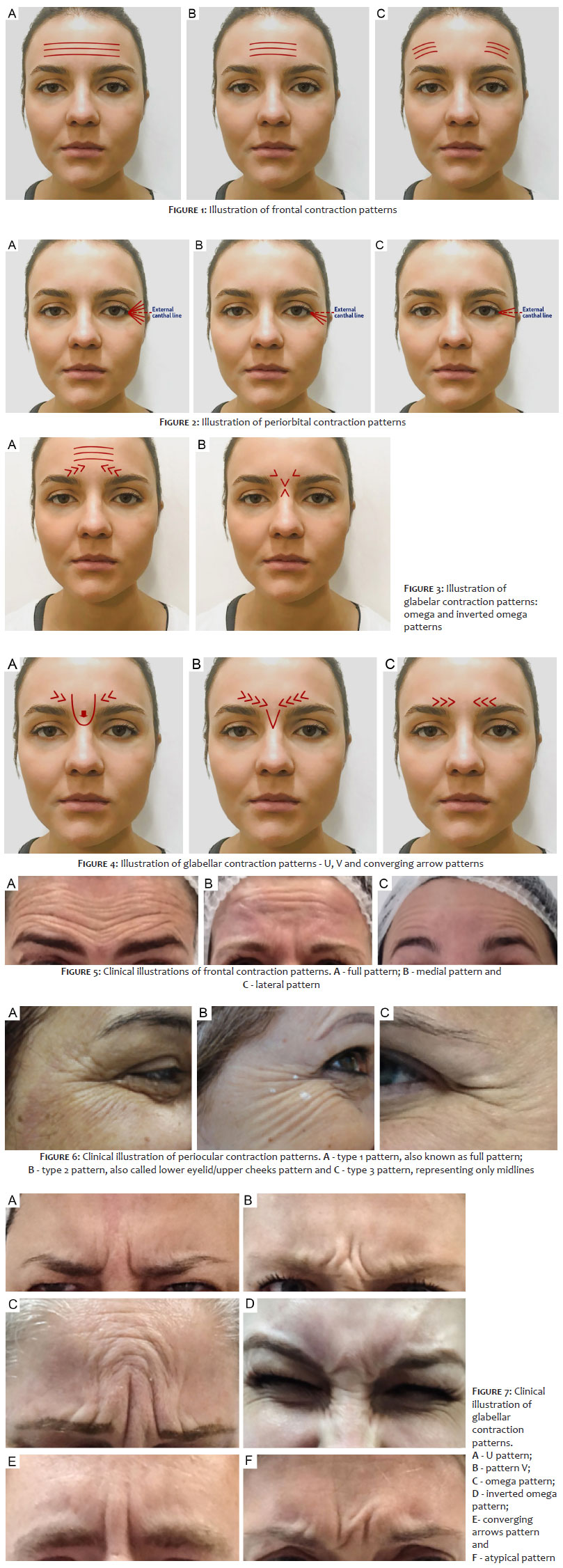
The contraction patterns of muscles located in the upper third of the face – including the frontal muscle, the glabellar region (corrugator supercilii, depressor supercilii, and procerus muscles), and the orbicularis oculi muscle – were evaluated in the present study. The classification patterns described by Trindade et al. for glabellar lines,4,5 Braz et al. for the frontal muscle,6 and Tamura et al.7 for lateral periocular rhytids were applied (Figures 1-7).
Patients who sought medical evaluation to apply botulinum toxin between 2012-2016 for men and 2015-2016 for women were included. All analyzes were performed using digital photographs taken during the medical consultation before product application. . Patients were treated with Botox® (Allergan, Dublin, Ireland), Dysport® (Galderma, Lausanne, Switzerland) or Xeomin® (Merz, Frankfurt, Germany) according to their preferences or those of the physician. The same researcher evaluated all patients.
Data were organized into descriptive graphs containing absolute frequencies, relative frequencies, means, standard deviations (SD), and 95% confidence interval (CI) estimates. The independent chi-square test was used to associate the qualitative variables, while the proportion test was chosen to compare the independent proportions. In all cases, statistical significance was considered if p<0.05.
Data analysis was performed using Microsoft Excel 2016 software and SPSS version 21 software. This study followed the ethical standards based on the Declaration of Helsinki 2000.
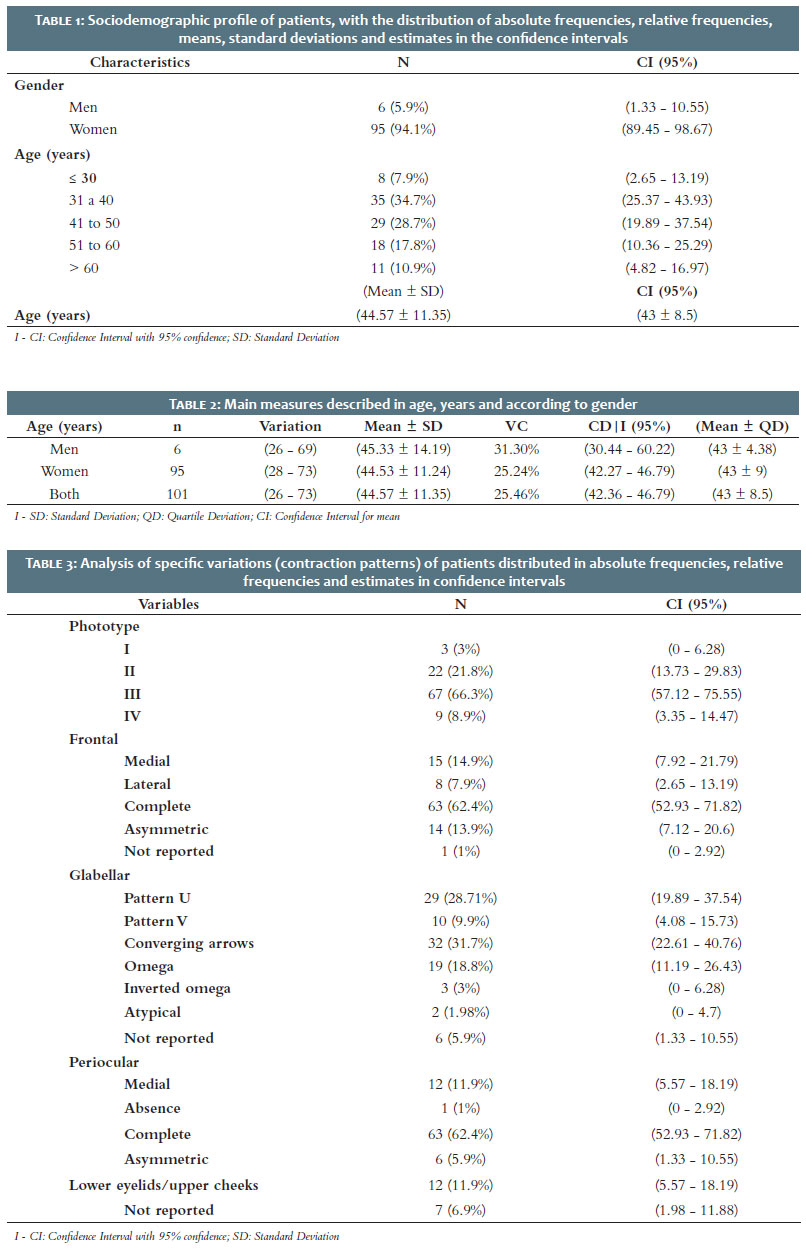
Tables 1 to 3 represent the univariate analysis of the characteristics assessed in absolute frequency, relative frequency, means, and standard deviations. They also present estimate proportions and the mean at 95% confidence intervals.
Men accounted for 5.9% of the studied patients, while women accounted for 94.1%. For men, the mean age was 45.33 ± 14.19, ranging between 26 and 69 years. Regarding women, the mean age was 44.53 ± 11.24, ranging between 28 and 73 years. The global mean age was 44.57 years, with a median of 43 years, a minimum of 26 years, and a maximum of 73 years.
Concerning the age group, most patients (63.24%) were between 31 and 50 years old, and 34.7% of subjects in this study were between 31 and 40 years.
According to the Fitzpatrick skin phototype scale, 66.3% of patients were skin phototype III, followed by skin phototype II (21.8%), skin phototype IV (8.9%), and skin phototype I (3%). No patients were skin phototypes V and VI.
We assessed frontal muscle contraction patterns in 100 patients. The complete pattern was the most common, in 62.4% of cases, followed by medial in 14.9%, asymmetric in 13.9%, and lateral in 7.9% of cases.
The glabellar contraction patterns were evaluated in 95 patients. The most frequent was the converging arrow pattern, found in 31.7% of cases, followed by the U pattern in 28.71% of cases. The omega pattern corresponded to 18.8% of the cases, the V pattern to 9.9%, and the inverted omega to 3% of cases. Two patients were considered atypical.
The complete pattern was the most common in the periocular region, present in 62.4% of cases, followed by the medial and lower/upper eyelids patterns, 11.9% of each case. The asymmetric pattern was found in 5.9% of patients.
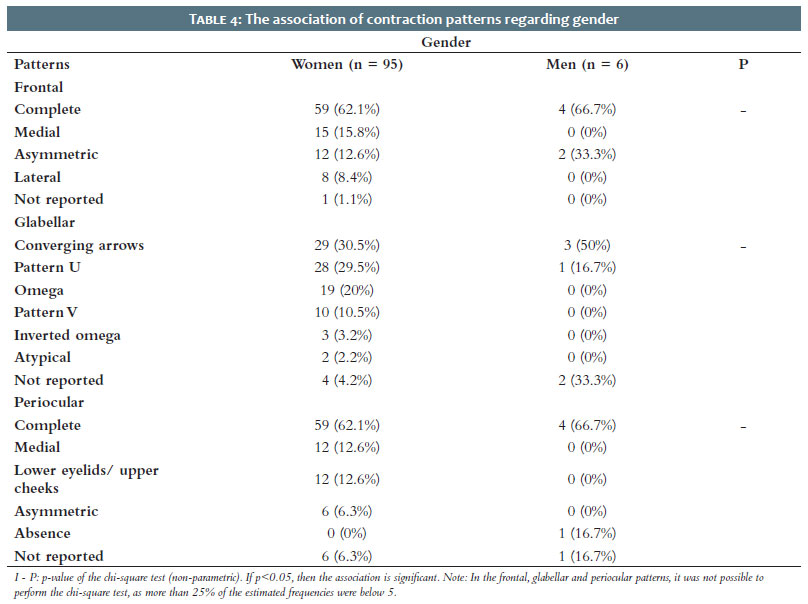
The most frequently found contraction patterns in both genders were the complete frontal, glabellar in converging arrows, and complete periocular patterns. However, it was not possible to use the chi-square test to assess associations between contraction patterns and gender because more than 25% of the expected frequencies were below 5.
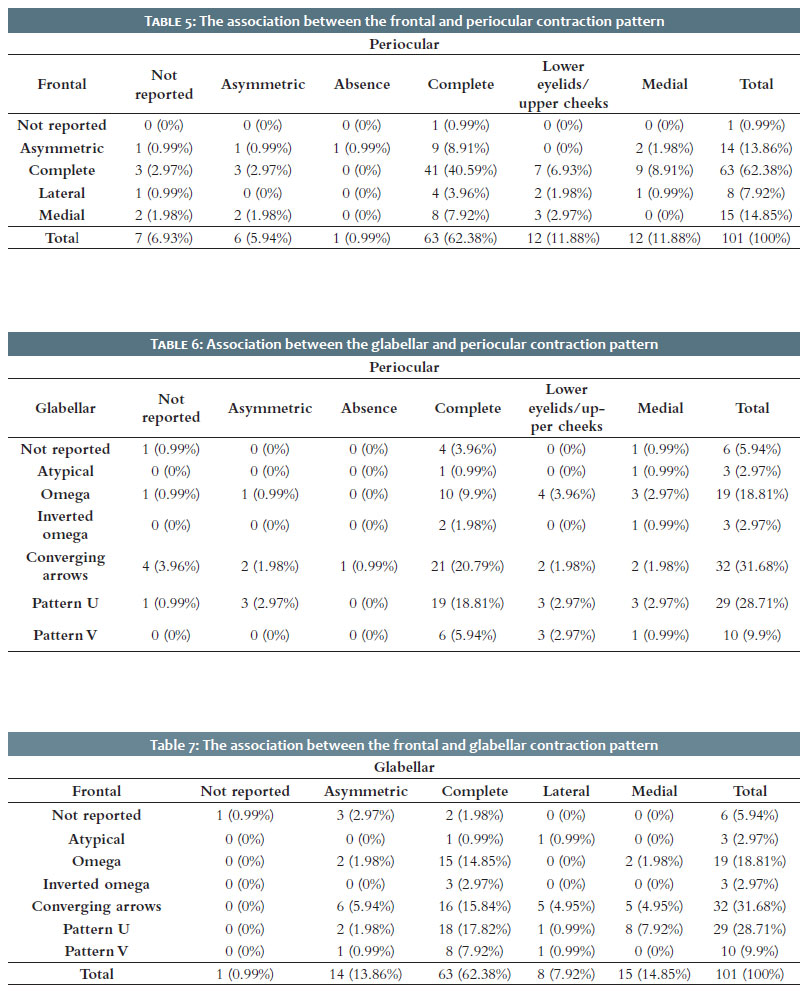
Table 4 depicts these data. Tables 5 to 7 show the associations between the different facial areas and their corresponding muscle contraction patterns.
When associating the patterns of the frontal and periocular regions, the complete frontal pattern and the complete periocular pattern occurred in 41 patients (40.59%). According to the proportion test, this association was statistically significant, with p<0.05.
Comparing the frequencies between the periocular and glabellar patterns, the glabellar converging arrows pattern and the periocular complete pattern were present in 21 patients (20.79%), the glabellar and the periocular complete U pattern occurred in 19 patients (18.81%), and the glabellar omega and the periocular complete patterns were observed in 10 patients (9.9%). According to the proportion test, the glabellar omega, converging arrows, and U patterns were associated with the periocular complete, with p<0.05.
Regarding the associations between the glabellar and frontal patterns, the omega pattern, with 15 patients (14.85%), converging arrows, with 16 patients (15.84%), and U pattern, with 18 patients (17.82%), were associated with the complete frontal pattern according to the proportion test, with p<0.05.
Considering the age group, patients between 31 and 50 years more commonly presented complete muscle contraction patterns in the frontal muscle, converging arrows and U patterns in the glabella, and the complete pattern in the periocular region.
Although the aesthetic use of botulinum toxin started more than 30 years ago, only recently the assessment of muscle contraction patterns in the upper third of the face has been standardized. Previously, the application patterns varied from the use of pre-established injection points to the application based on the muscular contraction of each patient, empirically. Although a standardized approach may be helpful, or even necessary, for purposes of comparative studies, the use of preset injection points may not be suitable for all cases, as a treatment with preset injection points can generate irregular results, with an artificial appearance, or even maintain areas of muscle contraction, not reaching the desired goal with the treatment. Today, the focus of cosmiatrics is to achieve a face that looks beautiful but as natural as possible. Thus, the more individualized a therapy, the better the results obtained.
Regarding the clinical profile of the patients, women predominantly comprised the study. The most common skin phototype was III. The prevalent age group was between 30 and 50, with an overall mean age of 44.57 years, similar to comparative studies.5
The muscles of the glabella region – corrugator supercilii, depressor supercilii, and procerus – generate the lowering of the eyebrow when they are contracted. In this action, the medial fibers of the orbicularis oculi muscle also participate. Paralysis of these muscles leads to reduction or erasure of the vertical and horizontal lines in the glabella.1–3
The frontal muscle is the only one responsible for raising the eyebrow. Generally, several injection points are needed for proper treatment. In patients with a complete contraction pattern, the muscle should be treated in multiple areas on the forehead. In contrast, patients with a medial or lateral contraction pattern may need focal treatment in regions with greater hyperkinesia to avoid eyebrow ptosis. In addition, the medial fibers are generally more robust and therefore require larger doses of the product.3 Correct treatment of the glabellar and frontal muscles is essential to maintain the correct position of the eyebrow.
The orbicularis oculi muscle is a sphincter whose function is to occlude the eye. While the contraction of the medial portion helps while lowering the eyebrow, the lateral portion, when contracted, leads to periocular rhytids. In the present article, patients were classified according to the patterns of rhytids they presented when asked to smile and categorized according to a classification system developed by Thamura et al.7 However, other authors also studied periocular lines and found slightly different results. Kane8 standardized a classification for periocular wrinkles in Caucasian women in a study conducted in 2003. He described four main patterns: periocular complete pattern, lower eyelid/upper cheeks, upper eyelid pattern, and central or lateral corner of the eye pattern. Patients were evaluated through smiling and squinting. In the present study, the rhytids pattern was observed by asking the patient to smile. It is probably why the upper eyelid pattern was not observed in the present study.
The most common contraction patterns in both sexes were the complete frontal, glabellar converging arrows, and periocular complete patterns. These data corroborate previous studies published by Braz et al. for frontal muscle contraction, and by Tamura et al. Regarding the lateral portion of the orbicularis oculi muscle contraction, in the glabellar complex, the converging arrows patterns were the most commonly found in this group, followed by the U and omega patterns. In previous studies published by Trindade et al., the V and U patterns were more frequently followed by the convergent arrow pattern. A study in the Chinese population, conducted by Jiang et al.,9 with more than 400 patients, focused on glabellar contraction patterns and found a classification compatible with the Chinese population, also reporting the converging arrows pattern as the most common.
Despite being studied and classified separately, the glabella, forehead, and periocular region muscles have interrelated fibers, and muscle contraction can influence the borderline muscles contraction to a greater or lesser extent.7
For example, the fibers of the orbital part of the orbicularis oculi muscle communicate with the fibers of the frontal muscle.7 It is not uncommon to ask patients to close their eyes tightly so that we can observe not only the orbicularis oculi muscle contraction, but to a greater or lesser degree, depending on the patient, the involuntary contraction of other muscle fibers located in the forehead, glabella, and even the nasal muscles. These data support the need to treat the entire upper third of the face in a single session, aiming at better results when compared to the treatment of isolated muscle groups. It is because interconnected muscle fibers that have not been appropriately addressed can lead to maintenance of muscle contraction in a specific area, resulting in the persistence of rhytids during movement.
Due to the interposition of muscle fibers and considering the influence of borderline fibers contraction, in this study, we assessed the associations between the different patterns of muscle contraction to verify their relationships and frequency. According to the proportion test, there was a statistically significant association between the periocular complete and frontal complete patterns; between the omega, converging arrows, U patterns for the periocular complete pattern; and the omega, converging arrows, and U patterns for the frontal complete pattern. This study confirmed that the most common patterns were associated with higher frequency.
Gender differences can also affect muscle strength. Due to this factor, it is common for men to have greater difficulty and resistance to treating muscles with botulinum toxin when compared to women. However, in the present study, due to the low number of male patients in the studied population, the correlation of contraction patterns and gender was not feasible.
Regarding the age group, patients between 31 and 50 years of age most commonly showed the complete muscle contraction pattern in the frontal muscle, the converging arrows and U-shaped patterns in the glabella area, and the complete pattern in the periocular region. Therefore, these were the patterns most frequently found in the age group that most sought this treatment.
Aesthetic treatments can improve the appearance and cosmetics and contribute to an increase in quality of life, as previously shown. It is, therefore, of paramount importance to understand the kinetics of the muscles involved in the formation of wrinkles to improve care and achieve the best results in patient treatment.10
The limitations of this study are its retrospective nature, the fact that it is based on clinical photography, and the low number of men studied. The small number of male patients can be observed in other comparative studies,5-7 because, as mentioned above, men tend to seek treatment with botulinum toxin less often than women. Prospective studies in different global populations are needed to better understand these muscle contraction patterns.
The present study shows the main muscle contraction patterns in the upper third of the face in a population of patients in southern Brazil and their clinical characteristics. It compares them to other Brazilian and worldwide studies. It also shows current associations between contractions types in different muscle groups and discusses their likely causes. The study of the contraction pattern aims to provide more accurate and safe treatments, in addition to the rational product use in the most indicated areas and with stronger muscle contraction.
Adma Silva de Lima 0000-0001-9240-4464
Statistical analysis; approval of the final version of the manuscript; study design and planning; active participation in research orientation.
Marina Gubert 0000-0002-9293-5019
Preparation and writing of the manuscript.
Thaise Lyra 0000-0002-7125-9576
Preparation and writing of the manuscript.
Carolina Fissmer Sardagna 0000-0002-2394-494X
Preparation and writing of the manuscript.
1. Giordano CN, Matarasso SL, Ozog DM. Injectable and topical neurotoxins in dermatology: indications, adverse events, and controversies. J Am Acad Dermatol. 2017;76(6):1013-24.
2. Giordano CN, Matarasso SL, Ozog DM. Injectable and topical neurotoxins in dermatology: basic science, anatomy, and therapeutic agents. J Am Acad Dermatol. 2017;76(6):1027-42.
3. Huang W, Foster JA, Rogachefsky AS. Pharmacology of botulinum toxin. J Am Acad Dermatol. 2000;43(2):250-9.
4. Almeida ART, Costa Marques ERM, Banegas R, Kadunc BV. Glabellar contraction patterns: a tool to optimize botulinum toxin treatment. Derm Surg. 2012;38(9):1506-15.
5. Almeida ART, Marques ERMC, Kanduc BV. Rugas Glabelares: estudo piloto dos padrões de contração. Surg Cosmet Dermatol. 2010;2(1):23-8.
6. Braz AV, Sakuma TH. Estudo piloto dos padrões de contração do músculo frontal. Surg Cosmet Dermatol. 2010;2(3):191-4.
7. Tamura B, Odo OY. Classification of periorbital wrinkles and treatment with botulinum toxin type. Surg Cosm Dermatol. 2011;3(2):129-34.
8. Kane MA. Classification of crow's feet patterns among caucasian women: the key to individualizing treatment. Plast Reconstr Surg. 2003;112(5 Suppl):33S-9S.
9. Jiang H, Zhou J, Chen S. Different glabellar contraction patterns in chinese and efficacy of botulinum toxin type A for treating glabellar lines: a pilot study. Dermatol Surg. 2017;43(5):692–7.
10. Ribeiro F, Steiner D. Quality of life before and after cosmetic procedures on the face: a cross-sectional study in a public service. J Cosmet Dermatol. 2018;17(5):688-92.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}