


Alessandra Jaccottet Piriz1; Elisângela de Quevedo Welter1; Laura Luzzatto2
Received on: 21/01/2020
Approved on: 18/02/2021
Financial support: None
Conflict of interest: None
Study conducted at the Universidade Federal da Fronteira Sul, Passo Fundo (RS), Brazil
Multiple adult xanthogranuloma is a rare and late variant of Juvenile xanthogranuloma, a non-Langerhans cell histiocytosis. It usually corresponds to a single lesion in adults, and the manifestation of multiples lesions is uncommon. We report a case of multiple adult xanthogranuloma, with Isotretinoin therapy failure and optimal response to CO2 Laser treatment in the surgical mode.
Keywords: Histiocytosis non-Langerhans-cell; Lasers gas; Xanthogranuloma juvenile
Xanthogranuloma is a benign and self-limited dermatosis characterized by non-neoplastic proliferation of histiocytes. It has phenotypic features different from Langerhans cells, with CD1a and S100 negative in immunohistochemistry and absence of Birbeck granules (cytoplasmic organelles identical to those of the Langerhans cell) in electron microscopy.1 Juvenile xanthogranuloma, the most common form of non-Langerhans cell histiocytosis, is prevalent in children, presenting as multiple yellowish-brown papules or nodules distributed preferentially in the head and neck region. The appearance in adults is rare, with few cases published since its first description in 1963 by Gartmann and Titsch. It usually manifests as a single lesion and, exceptionally, as multiple lesions, this form being called multiple adult xanthogranuloma.2 Cutaneous involvement is the rule, but extracutaneous manifestations have also been reported.
Possible spontaneous involution may occur. However, treatment with local cryotherapy, lesion excision, carbon dioxide laser (CO2 laser), and oral retinoids5 are potential therapies. We present a case of multiple adult xanthogranuloma without extracutaneous manifestation.
A 37-year-old man, previously healthy, living in an urban area, presented asymptomatic symptoms but progressive papular lesions on the face for 15 days, without any other complaints. He denied external factors related to the onset of the condition.
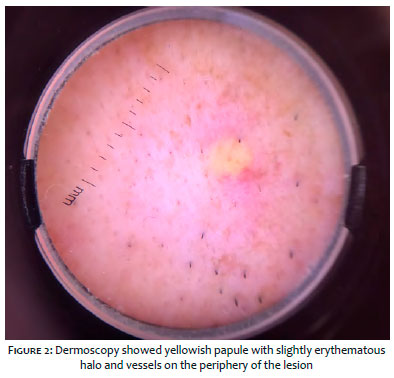
The dermatological examination showed several papules, normochromic to slightly yellow, firm, shiny, and well defined. The papules were diffuse on the face and some on the anterior chest, without central umbilication (Figures 1 and 2). The patient underwent a complete physical examination without adenomegaly or visceromegaly.
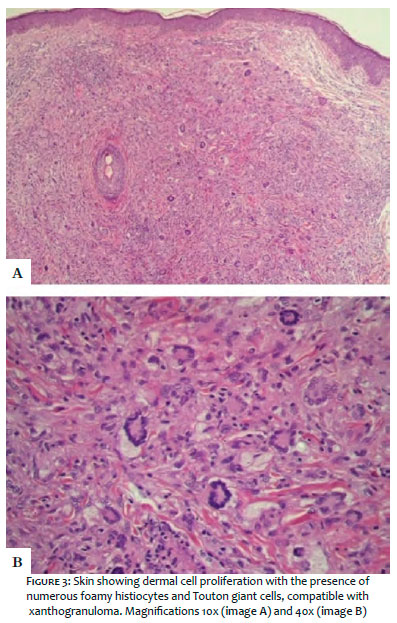
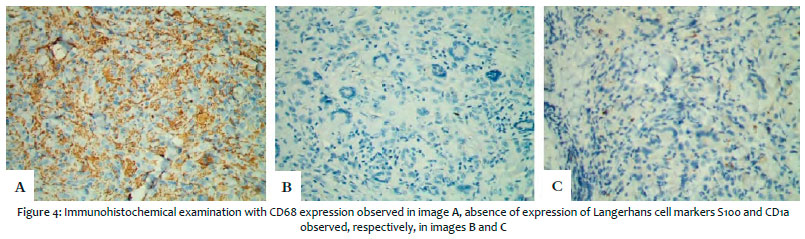
We investigated one of the lesions through excisional biopsy. The anatomopathological examination showed dermal cell proliferation with numerous foamy histiocytes and giant cells (Touton cells). These findings are compatible with xanthogranuloma (Figure 3). Immunohistochemical analysis revealed expression of CD68 (clone PGM1) and absence of expression of Langerhans cell markers S100 (polyclonal) and CD1a (clone 010) (Figure 4).
After assessing the clinical aspect of the patient and the anatomopathological and immunohistochemical findings, we concluded the diagnosis of multiple adult xanthogranuloma. Visceral involvement was assessed, with laboratory tests, chest radiography, ultrasound of the total abdomen, and ophthalmological evaluation, with no evidence of abnormalities.
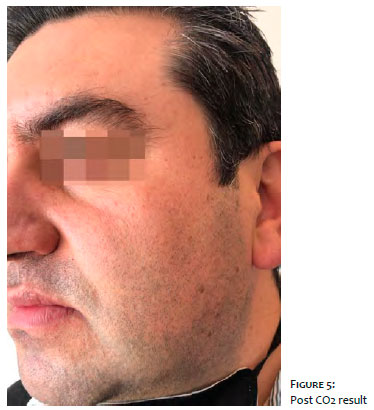
Due to the extent of cutaneous involvement and the patient’s discomfort, we decided to start isotretinoin 20 mg/day. After 30 days, there was an increase in the number of lesions. Thus, the medication was suspended, and CO2 laser sessions were performed in the surgical mode with excellent aesthetic results (Figure 5).
Multiple adult xanthogranuloma is a non-Langerhans cell histiocytosis. It is considered a rare and later manifestation of juvenile xanthogranuloma, occurring most frequently between the third and fourth decades of life,3 and the mean age at diagnosis is 47 years. The disease is slightly more common in men, at a ratio of 1.6/1.4 Clinically, it presents with five or more lesions, characterized by erythematous-yellow, firm, well-defined, asymmetric, and asymptomatic papules affecting predominantly the trunk, followed by the face and, less commonly, in the limbs.4 With the evolution of the condition, the lesions become brownish-yellow and present telangiectasias, which may result in small atrophic scars or hyperpigmentation after resolution.3,5 Differing from the juvenile form, which tends to involve in three to six years, spontaneous involution of the lesion in adults is not common.6
Despite preferentially affecting the skin, the disease can have extracutaneous involvement in 4% of children and 5-10% of adults, and the eyeball is the most frequently affected. Extraocular manifestations, which include liver, spleen, lungs, central nervous system, and hematopoietic tissue,3,5 can cause, for example, thrombocytosis and monoclonal gammopathy. As a dermatological manifestation, there are reports of underlying hematological neoplasia, which may appear before, concomitantly, or after the development of the disease, being considered a cutaneous marker of hematological disease.8 There is a hypothesis that excess gamma globulins in leukemic states could stimulate histiocytic production, resulting in the development of lesions.4 Serum lipid profiles are normal in patients with adult and juvenile xanthogranuloma.7 The etiology of xanthogranuloma is unknown; associations with trauma, infections, and neoplasms have been suggested.8
The tumor presents an accumulation of differentiated histiocytes that express the phenotype of dermal dendrocytes, although studies suggest that the cells of its origin could be plasmacytoid monocytes.7
From the histological point of view, the lesions present a dermal cell infiltrate composed of histiocytes, lymphocytes, eosinophils, and, occasionally, neutrophils. They exhibit a pleomorphic histiocytic infiltrate with a predominance of empty cells without lipids at the beginning. Later foam cells prevail, corresponding to lipid-filled histiocytes,2 together with the appearance of multinucleated giant cells, the Touton cells, in 95% of cases6 (multinucleated xanthomatous giant cells with nuclei arranged in a wreath-like pattern).3 The appearance of histiocytes laden with lipids and giant cells occurs late and is probably a secondary event in response to cytokine production by the lesion histiocyte.7 In the immunohistochemical study, histiocytes differ from Langerhans cells by positive CD68 and HAM56 macrophage cell markers as well as dermal dendrocyte markers (FXIIIa), presenting negative Langerhans cell markers S100 and CD1a. There is also a lack of Birbeck granules inside cells in the ultrastructural study.2 In doubtful cases, the expression of factor XIIIa offers more evidence for the diagnosis of xanthogranuloma.6
Juvenile xanthogranuloma was noted in association with different diseases, such as neurofibromatosis, Niemann-Pick disease, urticaria pigmentosa, and juvenile chronic myelomonocytic leukemia.7 The differential diagnosis is made between diseases classified as Langerhans cell histiocytosis, in addition to molluscum contagiosum, cryptococcosis, lepromatous leprosy, and neurofibromatosis.8
Therapeutic management is conservative, with spontaneous involution being possible but unlikely. Local cryotherapy, surgical excision, carbon dioxide laser (CO2 laser), and oral retinoids are reported, with an emphasis on isotretinoin.5,7 8
Extensive skin involvement, with several lesions, of the adult form of the condition, can cause unsightly discomfort and require treatment to accelerate the improvement of the disease.
Alessandra Jaccottet Piriz 0000-0003-1206-6114
Preparation and writing of the manuscript.
Elisângela de Quevedo Welter | 0000-0002-5544-6419
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Laura Luzzatto | 0000-0002-4193-6943
Critical literature review; critical revision of the manuscript.
1. Azulay RD, Azulay L. Dermatologia. 5 ed. São Paulo: Guanabara-Koogan; 2011.
2. Navajas B, Eguino P, Trébol I, Lasa O, Gardeazábal J, Díaz-Pérez JL. Xantogranuloma múltiple del adulto. Actas Dermosifiliogr. 2005;96(3):171-4.
3. Belga Junior W, Di Chiacchio N, Criado, PR. Tratado de Dermatologia. 2 ed. São Paulo: Atheneu; 2014. p.1209-14.
4. Ederle A, Kim KH, Gardner JM. Eruptive xanthogranuloma in a healthy adult male. J Cutan Pathol. 2017;44(4):385-7.
5. Ramos FS, Ferreira FR, Mandelbaum SH, Gonçalves FR. Xantogranuloma múltiplo do adulto: relato de caso e breve revisão da literatura. SPDV. 2018;76(2):193-6.
6. Saad N, Skowron F, Dalle S, Forestier JY, Balme B, Thomas L. Multiple adult xantho granuloma: case report and literature review. Dermatology. 2006;212(1):73-6.
7. Achar A, Naskar B, Mondal PC, Pal M. Multiple generalized xanthogranuloma in adult: case report and treatment. Indian J Dermatol. 2011;56(2):197-9.
8. Ferreira BR, Cardoso JC, Reis JP, Tellechea Ó. Multiple adult-onset xanthogranuloma, na uncommon diagnosis. An Bras Dermatol. 2017;92(2):294-5.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}