


Mariana Bergman1; Mariana das Neves Melo1; Antônio Gomes Neto1; Diogo Hiroshi Mizumoto1; Amílcar Castro de Mattos2,3
Received on: 25/03/2020
Approved on: 24/01/2021
Financial support: None
Conflict of interest: None
Acknowledgments: We thank Dr. André Luiz Simião, coordinator of the Department of Dermatology at the Pontifícia Universidade Católica de Campina (service accredited by the Brazilian Society of Dermatology) and the Melanoma Outpatient Clinic, to whom the authors express their respect and gratitude
Study conducted at the Pontifícia Universidade Católica de Campinas, Campinas (SP), Brazil
Patients with giant congenital melanocytic nevus are at higher risk of developing melanoma. After the first diagnosis of melanoma, there is also a higher incidence of subsequent melanomas in the same patient. However, the ideal therapy for this type of nevus is still controversial. We report the case of a patient with giant congenital nevus associated with multiple synchronous melanomas and the proposed treatment.
Keywords: Melanoma; Nevi and melanomas; Neoplasms
Melanocytic nevi are benign proliferations of melanocytic cells with distribution in nests in the epidermis, inside the dermis, or other tissues.1,2 The melanocytic nevus present at birth is defined as congenital. Some authors also include melanocytic nevi that appear up to six months of life, during the first year, or up to two years of age in this classification.1,3 Congenital nevi also differ from acquired ones by histology. In general, they have more varied architecture and morphology, and their nevus cells spread to the deeper layers of the skin, including the subcutaneous tissue.4,5,6,7 The occurrence of nevus cells within nerves, blood vessels, and sebaceous glands is the most specific finding for this distinction.5,8
The giant congenital melanocytic nevus (GCMN) is defined as a congenital melanocytic lesion that reaches at least 20 cm in diameter in adulthood.9,10 One of the biggest concerns involving patients with GCMN is the possibility of the appearance of melanoma. Currently, the literature has already proven the increased risk of these individuals developing the tumor.4,10,11
The malignant melanoma incidence has been growing significantly in recent years.12,13 The reasons for this increase are not proven, but it is known that exposure to sunlight, ultraviolet irradiation, genetic factors, and early detection are essential elements.13 It is also known that patients with melanoma have a higher risk of developing another one, which is called multiple primary melanoma.14
A 48-year-old man, white, presented giant congenital nevus in the right upper limb (RUL). He complained of asymptomatic blackened lesions on the nevus two years ago. Dermatological examination revealed a brown stain affecting the entire RUL, with increased local body hair, overlaid with blackish papules with irregular borders (Figures 1 and 2).
The patient had a history of excision of two lesions on the RUL two years earlier, with an anatomopathology of superficial extensive (Breslow thickness of 1 mm) and nodular (Breslow thickness of 0.2 mm) melanoma. At the time, no margin enlargement or sentinel lymph node research was performed. The patient denied other personal or family background relevant to the case.
Due to the presence of two suspected melanocytic lesions in the RUL (Figures 3 and 4) at the first consultation, the diagnostic hypothesis of melanoma with in-transit metastases was suggested. Thus we opted for an excisional biopsy, with a 2 mm margin, of the two lesions. Then, we conducted the margins enlargement of previously removed lesions lesion in an external service, requesting the staging exams (chest CT, abdominal US, and sentinel lymph node biopsy). The anatomopathological features of the two lesions showed malignant melanoma with an in situ pattern (Figures 5 and 6), and the staging exams showed no signs of neoplastic involvement.
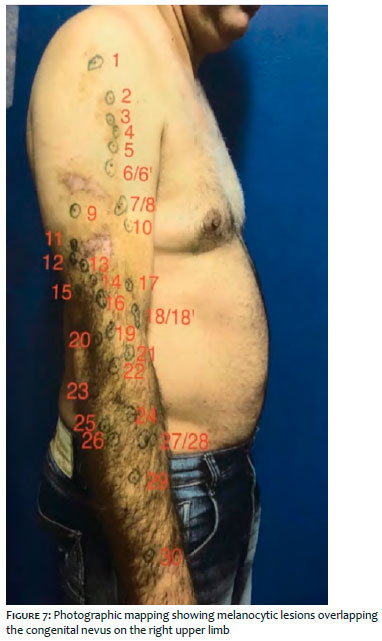
Six months later, three new suspicious melanocytic lesions were identified in the RUL. The anatomopathology revealed malignant melanoma in situ without ulceration. After three more months, due to many new suspicious lesions, photographic mapping and excisional biopsy of all lesions on the nevus were indicated (Figure 7). In total, we performed 30 excisional biopsies: two of them revealed melanoma in situ, Clark's level I, without ulceration. Enlargement of the margins and rigorous clinical follow-up in conjunction with the Oncology and Plastic Surgery teams were conducted.
There is a growth in multiple melanoma frequency associated with the increasing number of primary melanoma cases. Currently, the more prolonged survival of patients with melanoma contributes to this fact. In addition, the risk of a second melanoma is higher than the occurrence of secondary metastases from the first in patients with thin melanoma, a fact consistent with the case reported.15 Authors calculate that melanoma patients have a 900-fold higher risk of developing another melanoma than the general population of developing a first melanoma.14
There is also a higher prevalence of multiple melanoma in men, as in the case described.14
It is necessary to establish criteria to differentiate between a possible second melanoma, epidermotropic metastasis (cutaneous metastasis with epidermis involvement), or residual tumor to characterize multiple melanoma.13,16 Several clinical and anatomopathological elements are used for this diagnostic distinction: macro and microscopical different aspect among tumors; clinical and histological evidence of normal skin between synchronous lesions; presence of junctional alteration; and intraepidermal nests of malignant cytology cells demonstrating epidermal rise and spread.16
Despite the significant evidence showing that individuals with GCMN have an increased risk of developing melanoma, the exact incidence is still controversial. The low prevalence of GCMN and the scarcity of prospective comparative studies contribute to this fact.17
Some studies estimate that the malignancy rate is between 5% and 10%.4 It is believed that this higher incidence is related both to the high number of melanocytic cells and to the biological behavior different from the melanocytes present in the GCMN, citing as an example the structural chromosomal changes in the malignant process of these lesions.5,10
The development of melanoma in a patient with GCMN has a particularly poor prognosis. There are some justifications for this unfavorable evolution. The often rough or nodular surface of the GCMN can make early detection difficult.18 Also, the malignant transformations of small or medium congenital melanocytic nevi (CMN) begin more superficially at the dermal-epidermal junction, thus quickly showing the appearance of the lesion. However, in GCMN, melanoma usually develops in the deep dermis, making its detection harder and later.10,19 The large extent of GCMN is another factor that may contribute to this severity due to the greater likelihood that multiple channels will conduct its lymphatic drainage.18
The therapeutic approach of the GCMN is controversial and still represents a challenge. The therapy must consider several factors such as patient’s age, the size and location of the lesion, the possible functional impairments resulting from invasive procedures, and the presence of lesions suspicions on the nevus. The prophylactic surgical nevus excision has limitations regarding the uncertainties on its effectiveness as prevention for the neoplasia development since up to 50% of melanomas in patients with GCMN do not necessarily occur on the nevus. Also, there are technical difficulties in the execution and psychological impact associated with scars.20
Some authors defend the prophylactic excision of lesions that are more heterogeneous, thick, rough, or, for some other reason, challenging to follow clinically.19 This was the option in the case described due to the high risk of the patient because of the GCMN presence and previous evidence of melanoma.
In contrast to most of the cases described in the literature, the evolution was favorable in the case reported, possibly due to regular monitoring in a specialized service, easy visualization of clinical changes in the congenital nevus described due to the brownish color, and orientation to the patient regarding the risks and severity of the condition. The patient was encouraged to periodically self-examine the skin, observing changes in the nevus’ color, shape, or surface. These facts made the early detection and treatment possible, leading to the excision of the suspicious lesions and preventing neoplasia from having greater involvement.
Mariana Bergman | 0000-0002-7406-6788
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Mariana das Neves Melo | 0000-0002-4398-4877
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Antônio Gomes Neto | 0000-0003-1746-9828
Data collection, analysis, and interpretation; critical literature review.
Amílcar Castro de Mattos | 0000-0002-8547-3530
Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Diogo Hiroshi Mizumoto | 0000-0002-4979-3959
Data collection, analysis, and interpretation; critical literature review.
1. Grichnik JM, Rhodes AR, Sober AJ. Benign neoplasias and hyperplasias of melanocytes. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Lefell DJ, editors. Fitzpatrick's Dermatology in General Medicine. 7th ed. New York: McGraw-Hill; 2008. p. 1099-122.
2. Kincannon J, Boutzale C. The physiology of pigmented nevi. Pediatrics. 1999;104(4 Pt 2):1042-5.
3. Kaplan EN. The risk of malignancy in large congenital nevi. Plast Reconstr Surg. 1974;53(4):421-8.
4. Zaal L, Mooi W, Sillevis Smitt J, van der Horst C. Classification of congenital melanocytic naevi and malignant transformation: a review of the literature. Br J Plast Surg. 2004;57(8):707-19.
5. Mark GJ, Mihm MC, Liteplo MG, Reed RJ, Clark WH. Congenital melanocytic nevi of the small and garment type. Clinical, histologic, and ultrastructural studies. Hum Pathol. 1973;4(3):395-418.
6. Barnhill RL, Chastain MA, Jerdan MS, Lebbé C, Janin A, Lugassy C. Angiotropic neonatal congenital melanocytic nevus: how extravascular migration of melanocytes may explain the development of congenital nevi. Am J Dermatopathol. 2010;32(5):495-9.
7. Zaal LH, Mooi WJ, Klip H, van der Horst CM. Risk of malignant transformation of congenital melanocytic nevi: a retrospective nationwide study from The Netherlands. Plast Reconstr Surg. 2005;116(7):1902-9.
8. Rhodes AR, Silverman RA, Harrist TJ, Melski JW. A histologic comparison of congenital and acquired nevomelanocytic nevi. Arch Dermatol. 1985;121(10):1266-73.
9. Krengel S, Hauschild A, Schäfer T. Melanoma risk in congenital melanocytic naevi: a systematic review. Br J Dermatol. 2006;155(1):1-8
10. Viana ACL, Gontijo B, Bittencourt FV. Nevo melanocítico congênito gigante. An Bras Dermatol, 2013;88(6):863-78.
11. Ka VS, Dusza SW, Halpern AC, Marghoob AA. The association between large congenital melanocytic naevi and cutaneous melanoma: preliminary findings from an Internet-based registry of 379 patients. Melanoma Res. 2005;15(1):61-7.
12. Friedman RJ. Rigel DS, Silverman MK, Kopf AW, Vossaert KA. Malignant melanoma in the 1990s: the continued importance of early detection and the tole of physician examination and self examination of the skin. Ca Cancer J Clin 1991;41(4):201-6.
13. Lopes MMF, Oliveira RSF, Calvis LA, Teshirogi EY, Yojo LM, Bandiera D, Tovo LFR. Melanoma primário múltiplo. An Bras Dermatol. 1996;72(1):56-9.
14. Veronesi U, Cascinelli N, Bufalino R. Evaluation of the risk of multiple primaries in malignant cutaneous melanoma. Tumori. 1976;62(1):127-30.
15. Slingluff CL, Vollmer RT, Seigler HF. Multiple primary melanoma: incidence and risk factor in 283 patients. Surgery 1993;113(3):330-9
16. Viana, ACL, Goulart EMA, Gontijo B, Bittencourt FV. A prospective study of patients with large congenital melanocytic nevi and the risk of melanoma. An. Bras. Dermatol, 2017;92(2):200-5.
17. Beardmore GL, Davis NC. Multiple primary cutaneous melanomas. Arch Dermatol 1975:111(5):603-9.
18. Trozak DJ, Rowland WD, Hu F. Metastatic malignant melanoma in prepubertal children. Pediatrics. 1975;55:191-204.
19. Marghoob AA, Agero AL, Benvenuto-Andrade C, Dusza SW. Large congenital melanocytic nevi, risk of cutaneous melanoma, and prophylactic surgery. J Am Acad Dermatol. 2006;54(5):868-70.
20. DeDavid M, Orlow SJ, Provost N, Marghoob AA, Rao BK, Huang CL, et al. A study of large congenital melanocytic nevi and associated malignant melanomas: review of cases in the New York University Registry and the world literature. J Am Acad Dermatol. 1997;36(3 Pt 1):409-16.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}