


José Antônio Jabur da Cunha1; Lívia Zyman1; Flavia Nunes Maruyama2; Caroline Andrade Rocha2
Received on: 02/01/2019
Approved on: 13/02/2020
Financial support: None
Conflict of interest: None
Study conducted at the Santa Casa de Misericórdia of São Paulo, São Paulo (SP), Brazil
The reconstruction of deep surgical defects of the nasal tip and wing of the nose often presents a challenge to the surgeon. In these cases, full-thickness skin grafting is widely used, but it often results in sinking or graft depression. We present a surgical technique that is easy to perform and reproducible; nonetheless still very little diffused in Brazil: the “Drumhead” graft. This method performs the grafting of a rigid plastic suspension together with the full-thickness skin graft. Thus, this technique constitutes another tool for the dermatological surgeon to prevent irregularities of undesirable contours, graft depression, and nasal vestibule collapse.
Keywords: Nose; Nose neoplasms; Skin neoplasms; Skin transplantation
Skin cancer is the most common malignancy in Brazil, representing 25% of malignant tumors, with about 130,000 new cases per year.1 Basal cell carcinoma (BCC) is the most common skin cancer (70%), followed by squamous cell carcinoma (25%) and melanoma, with approximately 4% of cases.1,2 Approximately 80% of all BCCs occur on the face, of which 25% to 30% are located in the nose. 2,3 This fact gives considerable morbidity to these tumors.
Skin cancer treatment is primarily surgical, with frequent localized defects in the nose resulting from the cutaneous tumor excision in this region in the dermatologic surgeon practice. Located in the center of the face, with three-dimensional anatomy and cosmetic and functional relevance, the nose often represents a challenge to the dermatologic surgeon involved in the surgical removal of facial tumors of the face. Its free margins (nasal wing and tip) may suffer distortions that lead to unsightly results. These results highlight its high cosmetic importance.3
Practically, we can subdivide the nose anatomical regions into nasal tip and dorsum. These two regions have different characteristics that are relevant when choosing the reconstruction method. The nasal dorsum is supported on a firm structure (nasal bone), presenting thinner, more mobile, and elastic skin. In contrast, the nasal tip is sustained on a mobile framework (nasal cartilages), which has thick, sebaceous, inelastic, and little mobile skin.4
Several methods can be used to reconstruct surgical defects in the nose, such as closure by secondary intention, primary suture, flaps, and grafts. Primary closure is preferable whenever possible, but it is more used to reconstruct surgical defects located on the nasal dorsum. The little distensibility of the nasal tip’s skin associated with the mobile cartilaginous framework often leads to distortions of the nasal tip and wing, presenting undesirable results.4
Flaps are more challenging to perform and, when properly used, can present optimal aesthetic results. On the other hand, its oncological safety in nasal tumors is questioned, presenting a high risk of local recurrence when surgical margins are not assessed before reconstruction. Thus, from an oncological point of view, it is recommended to evaluate the surgical margins before a reconstruction using a flap or graft.4
Full-thickness skin graft (FTSG) is a versatile technique, easy to perform, and with high oncological safety.5 However, its lower aesthetic quality is known since it can lead to discrepancies in the color and texture of the grafted skin compared to the adjacent skin of the nasal region. Also, in deepest surgical defects of the nasal tip and wing, where the skin is usually quite thick and oily, the method can result in graft sinking with marked contours and unsightly results.6
We present a surgical technique that is easy to perform, reproducible, and still little disseminated in Brazil.
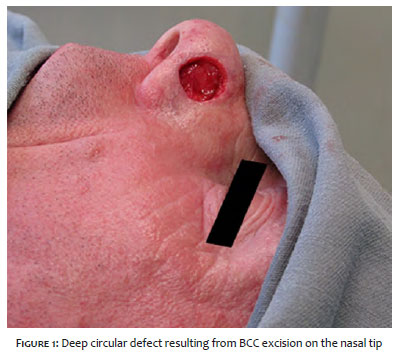
A 58-year-old man with a diagnosis of BCC located on the left nasal tip received an indication of surgical excision of the lesion placed in a thick and sebaceous skin. The lesion removal resulted in a circular, deep defect, measuring 15 mm in its largest diameter (Figure 1). We decided to perform the drumhead graft.
Technique: First, the FTSG donor site must be chosen. In this case, we opted for the pre-auricular region because it has some photodamage and good correspondence with the receiving area. Using the suture’s envelope, a mold of the recipient site was made, marking the donor site.
Then, the donor skin was removed in the subdermal plane using Joseph skin hook and curved iris scissors. Once removed, the tissue was defatted, trimmed, and preserved in 0.9% saline. Unlike the usual procedure, in this case, the FTSG was undersized to be placed over the deep surgical defect as if it were the “drumhead”. Then, it was sutured to the recipient site with 5-0 nylon suture with simple stitches (Figure 2).
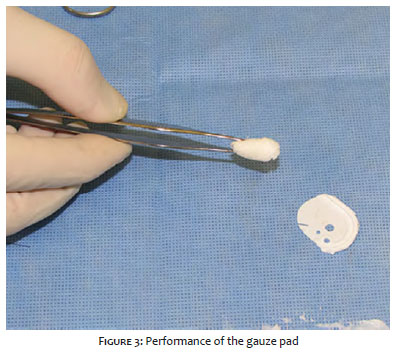
The patient received a gauze pad (Figure 3) and stitches (poliglecaprone - Monocryl 4-0) crossing the entire nostril width, starting at the graft, leaving the nasal cavity, and returning to the graft surface, forming a loop.
The gauze pad was placed in the intranasal region, directly below the graft recipient site, with a generous amount of antibiotic ointment. The intranasal suture loop was pulled out of the nose to keep the gauze pad firm in the nasal vestibule (Figure 4).
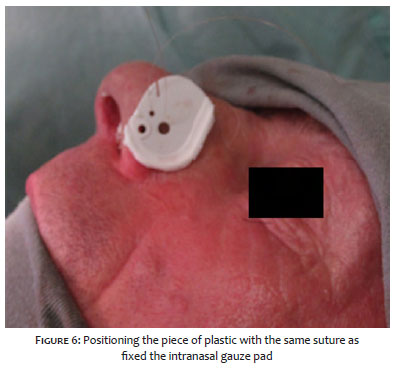
In the next step, we used a piece of rigid plastic from the poliglecaprone packaging (Monocryl 4-0), which was cut and placed directly on the graft. Care was taken to leave the edges rounded so they wouldn't traumatize the patient's skin (Figure 5). The support was attached to the same stitch fixing the intranasal gauze pad (Figure 6).
This rigid support had the function of supporting the intranasal gauze pad, which, in turn, pulled the graft bed, so it came into contact with the grafted skin.
The rigid plastic support and the full-thickness skin graft were soaked with antibiotic ointment and covered with gauze. The intranasal support remained for seven days to prevent any collapse or depression of the nasal vestibule.6 On the 7th postoperative day, the plastic support and intranasal gauze were removed, and on the 13th day, the suture was removed (Figure 7).
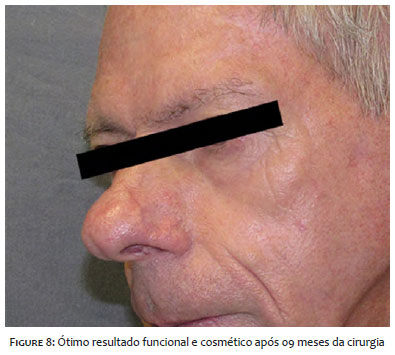
The patient evolved without any complications, such as surgical site infection, seroma formation, hematoma, or graft loss, in the postoperative period. He developed with good cosmetic results and was followed up until nine months after the operation when he was referred to the outpatient clinic of origin (Figure 8).
The FTSG is effective in repairing nasal defects but often unsuitable for deep surgical defects in the lower third of the nose, requiring the use of complementary techniques to prevent deformities.6
In reconstructions of this type of lesion with FTSG, the dermatologic surgeon usually tends to oversize the graft so that it can “cover” the entire bottom of the bed, ensuring graft contact with the bed and, consequently, its viability. In these cases, a dressing is sutured to the graft (Brown’s dressing) with the function to push it against the bed.
These two steps are fundamental to the graft take, but they are also responsible for the graft “sinking” in the postoperative period, with loss of the nasal contour.
The drumhead technique adapts these two steps since it undersize the graft and, instead of pushing it against the bottom, it pulls the bed against the graft. The wound bed contact with the grafted skin allows neovascularization and graft survival, in addition to preventing hematoma,5 seroma formation, and, mainly, internal collapse of the nasal vestibule or any graft depression.
We conclude that the drumhead graft method is a relatively simple and reproducible technique. Through it, we were able to unite the aesthetic qualities of the flaps with the oncological safety and execution simplicity of the grafts in the reconstruction of deep surgical defects in the region of the nasal tip and wing, preserving its functionality and cosmetics.
José Antônio Jabur da Cunha | 0000-0002-5780-0653
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Lívia Zyman | 0000-0003-1782-3778
Approval of the final version of the manuscript; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Flavia Nunes Maruyama | 0000-0003-0876-0824
Study design and planning; preparation and writing of the manuscript; critical revision of the manuscript.
Caroline Andrade Rocha | 0000-0002-0116-8548
Preparation and writing of the manuscript.
1. Souza Filho MV, Kobig RN, Barros PB, Dibe MJA, Leal PRA. Reconstrução nasal: análise de 253 casos realizados no Instituto Nacional de Câncer. Rev Bras Cancerol. 2002;48(2):239-45.
2. Wollina U, Bennewitz A, Langner D. Basal cell carcinoma of the outer nose: overview on surgical techniques and analysis of 312 patients. J Cutan Aesthet Surg. 2014;7(3):143-50.
3. Moura BB, Signore FL, Buzzo TE, Watanabe LP, Fischler R, Freitas JOGD. Reconstrução nasal: análise de série de casos. Rev Bras Cir Plást. 2016;31(3):368-72.
4. Bradley KD, Wentzell JM. The "Drumhead" graft repair of deep nasal alar defects. Dermatol Surg. 2007;33(1):17-22.
5. Meyers S, Rohrer T, Grande D. Use of dermal grafts in reconstructing deep nasal defects and shaping the ala nasi. Dermatol Surg. 2001;27(3):300-5.
6. Adams DC, Ramsey ML. Grafts in dermatologic surgery: review and update on full-and split-thickness skin grafts, free cartilage grafts, and composite grafts. Dermatol Surg. 2005;31(8 Pt 2):1055-67.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}