


Bárbara de Oliveira Martins; Juliana Câmara Mariz; Laura Franco Belga; Marcella Leal Novello D'Elia; Carlos Baptista Barcaui
Received on: 26/08/2020
Approved on: 04/03/2021
Financial support: None
Conflict of interest: None
Study conducted at the Department of Dermatology of the Pedro Ernesto University Hospital, Universidade do Estado do Rio de Janeiro, Rio de Janeiro (RJ), Brazil
Basal cell carcinoma is the most common type of nonmelanoma skin cancer, and the nose is the most common site. The treatment of choice, surgical excision, may cause nasal defects, which may be challenging for surgeons for maintaining functionality and aesthetics. When planning the reconstruction, one should carefully consider the nose’s anatomical features and the patient’s individual characteristics. We report four cases of nasal defects due to surgical excision of basal cell carcinoma approached with different closure techniques (primary closure, flap, graft, and second-intention healing), achieving equally satisfactory esthetic and functional results..
Keywords: Carcinoma Basal Cell; Nose; Reconstruction; Surgical Flaps; Skin Transplantation
Non-melanoma skin cancer is the most common neoplasm in the world, and basal cell carcinoma (BCC) is the most frequent (75%), followed by squamous cell carcinoma (SCC) (20%) and melanoma (5%).1 Head and neck are the most affected regions, most commonly the nose due to cumulative sun exposure. 2
When approaching malignant lesions on the face, the primary objective is to perform surgery with free oncological margins to excise the tumor completely – the gold standard treatment. Secondary endpoints are maintenance of functionality and obtaining a good aesthetic result.1,2
However, the resulting surgical defect is close to orifices in the head and neck. Thus, resection with safety margins and reconstruction constitutes a significant challenge, demanding knowledge, experience, and creativity on the surgeon’s part, and often requiring flaps and grafts.1
Case 1 - A 63-year-old man presented a papular lesion in the right nasal wing. The lesion was excised and closed by secondary intention (Figure 1).
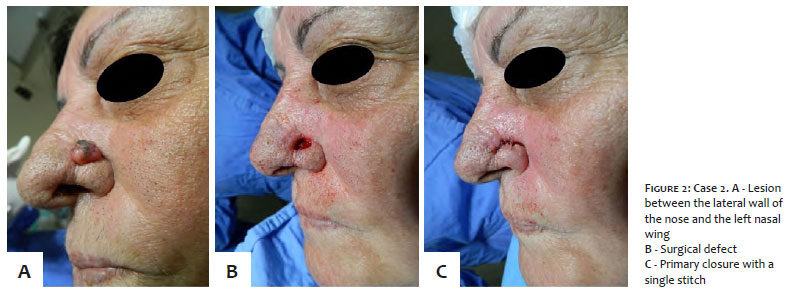
Case 2 - A 64-year-old woman exhibited a nodular lesion with an ulceration area between the lateral wall of the nose and the left nasal wing. The lesion was excised and closed by primary intention (Figure 2).
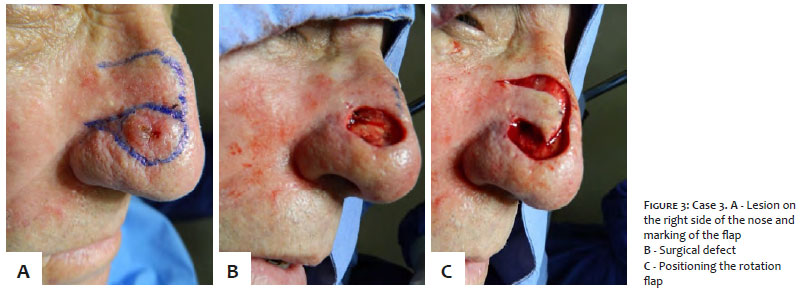
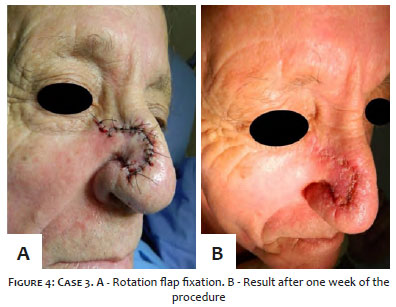
Case 3 - A 70-year-old man had an ulcerated nodular lesion on the right side of the nose. The patient underwent excision and reconstruction with a rotation flap (Figures 3 and 4).
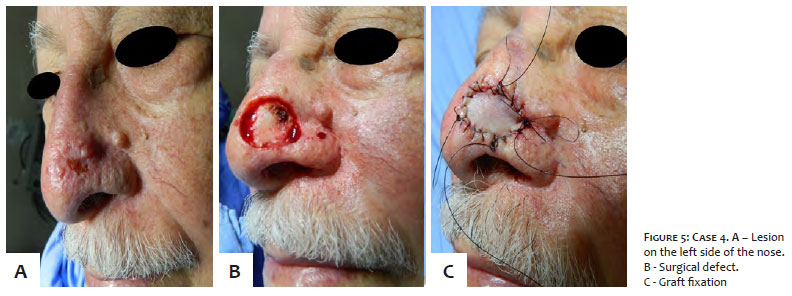
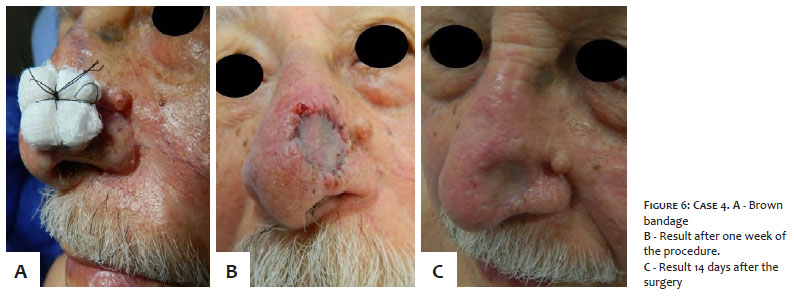
Case 4 - A 91-year-old man presented an ulcerated nodular lesion on the left side of the nose. The patient underwent excision and skin graft using the infraclavicular region as donor area (Figures 5 and 6).
All cases were clinically suggestive of BCC, and an experienced professional confirmed the diagnosis through dermoscopy. Local anesthesia was applied with an anesthetic solution, and the lesions were excised with 4 mm surgical margins delimited by dermoscopy. The suture, when performed, used 5-0 nylon. The procedures had no complications in the intra and postoperative periods.
The nose plays an essential role in facial aesthetics.3 It is the facial structure most exposed to the sun and, therefore, the most affected by BCC. BCC is a malignant neoplasm of follicle germ cells, with no precursor lesions described. Its risk factors include exposure to ultraviolet radiation, light skin phototypes, positive family history, childhood ephelides, immunosuppression, exposure to arsenic, scarring, and hereditary diseases.
Mortality from BCC is less than 0.1% - with a cure rate greater than 90% when excised - and metastases are rare.4
The general principles of skin defect reconstruction encompass characteristics, comorbidities, patient preferences (which must be well established in the preoperative consultation), location, and dimensions of the defect.5,6 Other aspects that deserve attention are the use of anticoagulants and smoking due to the negative impact on the healing process.5
Regardless of the lesion’s location or size, the entire face must be prepared at the time of surgery, providing the surgeon with a good view and access if the incision needs to be enlarged.5 According to the National Comprehensive Cancer Network (NCCN), the therapeutic plan must be established based on the BCC risk stratification. The criteria include the lesion’s location and size, margins definition, whether the lesion is primary or recurrent, immunosuppression presence, previous treatment with radiotherapy at the lesion site, histological subtype, and perineural involvement. Regarding surgical excision, NCCN recommends 4 mm margins for lesions considered to have a low risk; and resorting to Mohs surgery for lesions at high risk. In the case of techniques without a complete assessment of the tumor margins, guidelines advise identifying the BCC subclinical extension, establishing wide margins, evaluating the lesion in the postoperative period, and performing primary or late closure of the surgical defect. Radiotherapy appears as an option for patients who are not candidates for surgery. Systemic therapy - Vismodegib and Sonidegib - is indicated for high-risk cases, such as locally advanced disease where radiotherapy or curative surgery is not viable.7
Concerning lesions excised in the nasal region, options for repairing the surgical defect involve healing by secondary intention, primary closure, flaps, and skin graft.6 Secondary healing is underutilized.5,8 However, it has numerous advantages, including excellent aesthetic results – the best ones observed in concave areas of the nose, more superficial lesions, and injuries smaller than 2 cm.5
Also, it is helpful for patients who would not tolerate the reconstructive procedure.5 Healed wounds continue to improve their appearance over time.8
Primary closure is commonly used for defects up to 1 cm.2,9 Higher nose regions, non-sebaceous, are more favorable to the technique due to greater mobility. Comprehensive dissection is crucial to approach the margins under minimal tension, in addition to the internal suture, which also reduces the pressure in the wound closure. Primary closure is widely used due to its simplicity, fewer complications, and lower costs.2 However, the skin of the lower third of the nose has limited mobility and, therefore, the use of primary closure is restricted to minor defects.2
Regarding flaps, there are three basic types of tissue movement: transposition, advancement, and rotation.6 The rotation flap can reconstruct defects of 1 cm to 2 cm in the nasal dorsum and tip.2,10
It consists of rotating the adjacent tissue around an axis to close the primary defect.6 The rotation flap presents the best outcomes. It recruits an integument adjacent to the defect, with similar clinical (texture, thickness, color) and histological (dermal thickness, pilosebaceous gland density) properties. Thus, it satisfies the Millard principle, according to which “the closest skin is the best skin”, or the Gillies analogy, which advocates replacing a tissue by an equivalent coming from neighboring donor sites.11
Among the flaps, it is worth mentioning the interpolation ones: the paramedian forehead flap (Indian), with great applicability for broad and deep nasal defects in the distal region of the nose,12,13,14 as well as the nasolabial interpolation, excellent option for nasal wing reconstruction. Despite the need for two or more operative times, the final aesthetic and functional results are satisfactory.14
If not correctly designed, the flap can cause anatomical distortions. They are contraindicated if the neoplasm is not entirely excised due to the risk of tumor recurrence under the flap.6
Relative contraindications include the risk of bleeding and aspects that may predispose to poor wound healing.6,15
The skin graft is not considered an ideal substitute for nasal skin, especially for thick and sebaceous skin of the nasal tip, wing, lower sidewalls, or dorsum.2 However, it is a quick and straightforward solution in patients at high surgical risk or in lesions with a high probability of recurrence.16 It recruits tissue at a distance, favoring the occurrence of dyschromia, difference in skin thickness, and irregularity in its surface, in addition to the possibility of retraction, leading to less symmetrical and unsightly results.12,16 The most used donor areas are the supraclavicular and retroauricular.16
Reconstructions of surgical defects in the nose are complex due to its unique anatomical contours, besides this structure’s functional and aesthetic importance.
The choice of reconstructive modality will depend on the location, size and depth of the surgical defect, in addition to the surgeon’s experience. Although there are several forms of nasal defects reconstruction, it is up to the surgeon to decide which approach brings the best aesthetic and functional results, with individual treatment being the best choice.
This study encompasses four cases of defects located in similar topographies, each one approached with different closure techniques, according to the local characteristics of the patient’s skin, culminating in satisfactory functional and aesthetic results.
Bárbara de Oliveira Martins | 0000-0002-6650-1719
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Juliana Câmara Mariz | 0000-0002-7292-1648
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; critical literature review.
Laura Franco Belga | 0000-0002-8355-4185
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Marcella Leal Novello D'Elia | 0000-0002-3575-5732
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript
Carlos Baptista Barcaui | 0000-0002-3303-3656
Approval of the final version of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
1. Freitas CAF, Santos AN, Bittner GC, Sanabria BD, Levenhagen MMMD, Hans-Filho G. Nonmelanoma skin cancer at critical facial sites: results and strategies of the surgical treatment of 102 patients. J Skin Cancer. 2019;2019:4798510.
2. Salgarelli AC, Bellini P, Multinu A, Magnoni C, Francomano M, Fantini F, et al. Reconstruction of nasal skin cancer defects with local flaps. J Skin Cancer. 2011;2011:181093.
3. Patel RG. Nasal anatomy and function. Facial Plast Surg. 2017;33(1):3-8.
4. Montagna E, Lopes OS. Bases moleculares do carcinoma basocelular. An Bras Dermatol. 2017;92(4):518-21.
5. Rogers-Vizena CR, Lalonde DH, Menick FJ, Bentz ML. Surgical treatment and reconstruction of nonmelanoma facial skin cancers. Plast Reconstr Surg. 2015;135(5):895e-908e.
6. Prohaska J, Cook C. Rotation Flaps. [Updated 2020 Feb 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482371/
7. National Comprehensive Cancer Network. Basal Cell Skin Cancer (Version 1.2020). Available from: https://www.nccn.org/professionals/physician_gls/pdf/nmsc.pdf. Accessed May 23,2020.
8. Liu KY, Silvestri B, Marquez J, Huston TL. Secondary intention healing after mohs surgical excision as an alternative to surgical repair: evaluation of wound characteristics and esthetic outcomes. Ann Plast Surg. 2020;85(S1 Suppl 1):S28-S32.
9. Han DH, Mangoba DC, Lee DY, Jin HR. Reconstruction of nasal alar defects in asian patients. Arch Facial Plast Surg. 2012;14(5):312-17.
10. Rohrich RJ, Griffin JR, Ansari M, Beran SJ, Potter JK. Nasal reconstruction--beyond aesthetic subunits: a 15-year review of 1334 cases. Plast Reconstr Surg. 2004;114(6):1405-19.
11. Grandpierre X, Sartre JY, Duteille F. Reconstruction des pertes de substance superficielles du carrefour des sous-unités de la pointe, de l'aile et de la face latérale du nez : étude sur 36 patients [Reconstruction of superficial defects from the crossroad of nasal subunits, tip, alar lobule and lateral side wall: Study of 36 patients]. Ann Chir Plast Esthet. 2016;61(4):248-56.
12. Ramsey ML, Ellison CA, Al Aboud AM. Interpolated Flaps. [Updated 2020 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470521/
13. Reckley LK, Peck JJ, Roof SB. Flap Basics III. Facial Plast Surg Clin North Am. 2017;25(3):337-46.
14. Sakai RL, Tavares LCV, Komatsu CA, Faiwichow L. Retalho nasogeniano de interpolação na reconstrução da asa nasal após ressecção de tumores cutâneos. Rev Bras Cir Plást. 2018;33(2):217-21.
15. Starkman SJ, Williams CT, Sherris DA. Flap Basics I: rotation and transposition flaps. Facial Plast Surg Clin North Am. 2017;25(3):313-21.
16. Sbalchiero JC, Gregorio TCR, Leitão L, Leal PRA, Dibe MJA. Nasal tip reconstruction in cutaneous malignancies. Rev Bras Cir Plást 2005;20(1):12-6.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}