


Bruna Santana Alarcon1; Ana Maria Quinteiro Ribeiro1; Jules Rimet Borges1; Luiz Fernando Froes Fleury Jr.1; Juliana de Souza Couto Eckert2
Received on: 26/02/2021
Approved on: 16/03/2021
Financial Support: None
Conflict of Interest: None
Acknowledgement: I thank my colleagues Dra. Nayara Rubia, Dra. Carolina Inka, and Dra. Marcela Barbosa who supported me in data collection
Study conducted at the Department of Tropical Medicine and Dermatology of the Hospital das Clínicas of the Universidade Federal de Goiás, Goiânia (GO), Brazil
INTRODUCTION: Basal cell carcinoma is the most common non-melanoma malignancy in humans. Its superficial variant has specificities that can represent a diagnostic and therapeutic challenge.
OBJECTIVE: To describe the epidemiological profile of patients with superficial basal cell carcinoma (SBCC) treated at a reference service and to correlate, statistically, clinical, dermoscopic, and anatomopathological characteristics.
METHODS: Observational, analytical, cross-sectional study conducted by collecting data from patients with suspected SBCC between November 2019 and October 2020.
RESULTS: In total, we confirmed 25 lesions as SBCC. They were more frequent in women, in the head and neck, and with a diameter of less than 1 cm. We also observed, in clinical characteristics, a predominance of individuals over 60 years old and with phototypes II and III. The anatomopathological examination observed some pigmentation in the lesions evaluated and a predominance of intra-epidermal keratinocytes in lesions with maple leaf-like areas in dermoscopy.
CONCLUSIONS: SBCC can present clinically as a pigmented lesion, affecting more the head and neck regions. Lighter skin phototypes are more likely to have SBCC with pigmented dermoscopic structures. Intra-epidermal keratinocytes possibly correlate with the formation of maple leaf structures.
Keywords: Basal cell carcinoma; Dermoscopy; Epidemiology; Skin Neoplasms; Pathology
Basal cell carcinoma (BCC) is a malignant skin neoplasm derived from the cells of the basal layer of the epidermis and perianexial structures.1 It is part of the group of non-melanoma skin cancer that represents the most common tumors in humans.1,2 Basal cell carcinoma represents 80% of this group, and the superficial variant comprises 10% to 30% of cases of basal cell carcinoma.6 North American studies reveal an increase in basal cell carcinoma incidence of up to 50% in men.4 This finding corresponds to a world trend.4
Superficial basal cell carcinoma presents clinically as a circumscribed and erythematous plaque, with a thin border and hypochromic/ atrophic center.6 It tends to affect more commonly the trunk, legs, and shoulders.6,2 It is suggested that the origin of BCC is related to exposure to intermittent ultraviolet (UV) radiation in childhood and adolescence.3
The main risk factors for developing BCC are: male gender, advanced age, exposure to ultraviolet rays, previous history of other skin cancers, phototherapy, radiotherapy, and Fitzpatrick skin phototype I and II.1, 2
Dermoscopy is an essential tool that helps in differentiating between superficial and non-superficial BCC. This examination also contributes to therapeutic decisions and patient follow-up.5
In the anatomopathological study, BCC presents as an epithelial malignancy composed of nests of basaloid cells.9 These nests in the SBCC are distributed in several lesion foci in close contact but without invasion of the dermis.9 Due to the difficulty in delimiting the lesion and consequent possibility of incomplete excision, the superficial variant presents the highest risk for local recurrence.7,9
A study on the epidemiological profile of dermatological consultations in Brazil shows that non-melanoma skin cancer corresponds to the third reason for seeking dermatological care.8 In the age group above 60 years, BCC represents the first major cause for consultation with the dermatologist (19.3%).8 The authors also observed that the chance of diagnosing non-melanoma skin cancer is higher in public (SUS) than in the private sector.8
National cancer statistics register BCC as non-melanoma skin cancer. This group encompasses all types of BCC and SCC (squamous cell carcinoma). For this reason, the actual frequency of SBCC in the country is uncertain. Pereira et al. (2015) evaluated the regional skin cancer data between 1988 and 2009 in individuals under 40 years old.21 The non-melanoma cancer statistics were individualized between BCC and SCC. It allowed observing an incidence of 1,614 cases of BCC in that period and a predominance in women.
Despite the extensive scientific literature on basal cell carcinoma, specific studies on the superficial variant are scarce. This research aims to describe the epidemiological profile of superficial basal cell carcinoma in reference service and to correlate clinical, dermoscopic, and anatomopathological variables statistically. Studies like this are essential to disseminate and draw the attention of the dermatologist on the subject. Also, it can contribute to the development of prevention strategies, early diagnosis, and better therapeutic results, surgical or not.
It was an observational, analytical, and cross-sectional study. The inclusion criteria were patients with suspected superficial BCC who presented at the referral service from November 2019 to October 2020. These patients underwent incisional biopsy or excision with margin, and the material was sent to the Pathological Anatomy Service of the hospital. We collected data on sex, age, skin color according to Fitzpatrick scale, previous profession, involvement site, lesion size, dermoscopy pattern, melanic pigment presence in the anatomopathological examination from each patient. All lesions were photographed with a digital camera and DermLite DL200 Hybrid® dermatoscope. Two examiners experienced in dermoscopy analyzed the images and filled out a 12-items checklist with structures that could be present in each lesion. The checklist was revised, and the final table was considered as the sum of the structures found by the two examiners.
Lesions not confirmed as SBCC by anatomopathology or those not possible to access were excluded from the study.
The statistical analysis to correlate the different variables was performed using Fisher’s exact test, assuming a significance level of p<0.05 by the statistical software R. The Ethics Committee approved the study under the CAD number 29726520.4.0000.5078, and all patients signed the informed consent term.
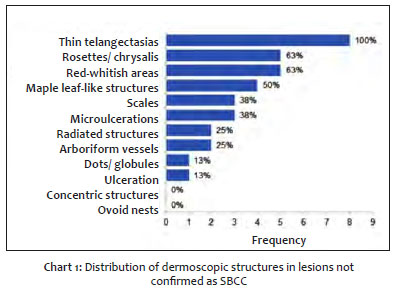
We collected a total of 34 suspicious lesions from 18 patients. Eight were excluded because they were not confirmed as SBCC after the pathology; four were confirmed as actinic keratosis, one as nodular BCC, one as basosquamous carcinoma, one as sclerodermiform BCC, and one as chronic dermatitis. One was excluded from statistical calculations because the sample was lost. Chart 1 describes the frequency of dermoscopic structures in lesions not confirmed as superficial BCC, with fine telangiectasias being the most common structure.
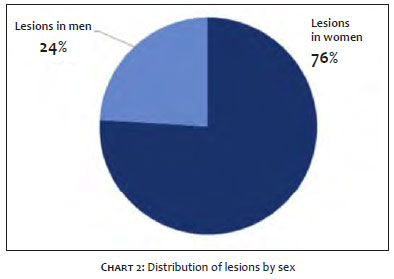
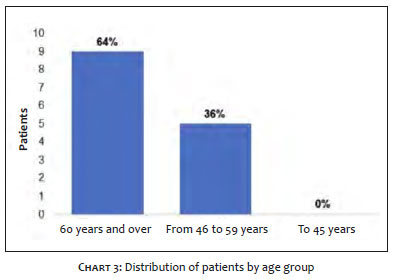
In the final sample, 25 lesions in 14 different patients were confirmed as SBCC. Of these, 19 lesions were in women (76%) and six in men (24%) (Chart 2). The proportion of women to men was 1.8:1. The most frequent age group was over 60 years old (64%), followed by between 45 and 59 years old (36%) (Chart 3). Among women over 60 years old, 85.7% of the lesions were multiple, and 14.5% were single.
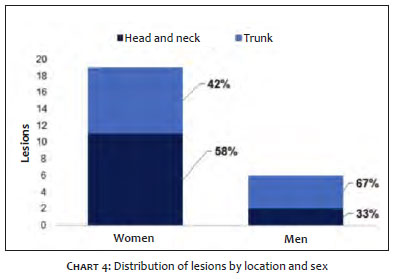
Among women, 11 injuries (57.8%) were located on the head and neck and eight on the trunk (42.2%). Among men, two lesions were on the head and neck (33.3%) and four on the trunk (66.7%). None of the sexes presented lesions in the upper or lower limbs or genital region (Chart 4). Two lesions were located in a non-exposed area (8%) and 23 in a photoexposed area (92%).
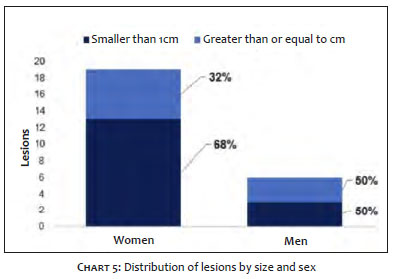
Among women, 13 lesions were <1 cm (68.5%) and six were ≥1 cm (31.5%). Among men, three lesions were <1 cm (50%) and three were ≥1 cm (50%) (Chart 5).
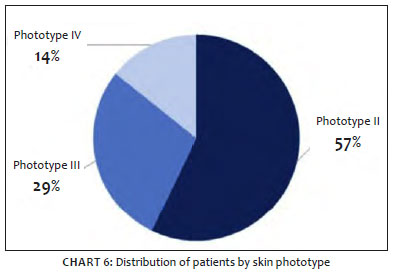
Of the 14 patients who composed the study, eight were skin phototype II (57.1%), four were skin phototype III (28.5%), and two were skin phototype IV (14.4%). No patients were skin phototype I, V, or VI (Chart 6).
Of the total number of patients, seven were rural workers (50%); one, a street vendor (7%); one declared having other professions (7%); and five did not report (36%).
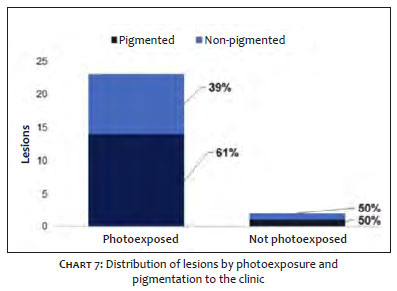
By clinical evaluation, 15 lesions were pigmented (60%) and 10, non-pigmented (40%). Chart 7 shows the distribution of these lesions by photoexposed area.
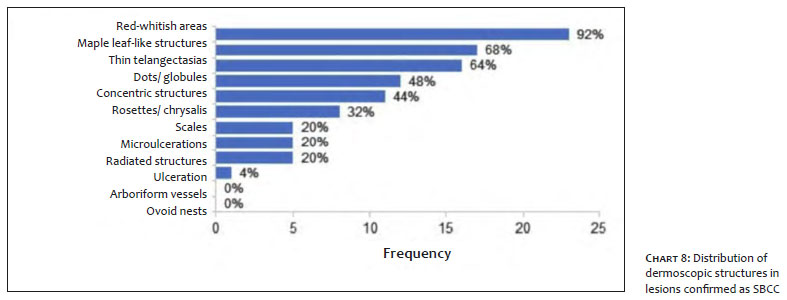
When considering all lesions confirmed as SBCC, the five prevalent patterns in dermoscopy were red-whitish areas without structures (92%), maple leaf-like areas (68%), fine telangiectasias (64%), dots/globules (48%), and concentric structures (44%). Graph 8 shows the frequency distribution of structures in lesions confirmed as SBCC.
Of the 25 confirmed lesions, 17 presented some type of melanin pigment in anatomopathology (intraepidermal keratinocytes with pigment, intradermal or intraepidermal macrophages with pigment - melanophages); five did not present (20%); and in three had no data (12%).
In the present sample, SBCC lesions were more frequent in women, with a predominance of 76% in this group. These results are consistent with those found in the literature.10,11,12 The average age of women was 64.6 years (50-78 years) and for men 66.2 (51-82 years), with no statistically significant difference between them (p=0.40). The literature shows that women tend to be diagnosed younger than men.11,10,19,12,13 Such difference may be justified by the greater concern of women with aesthetic and health issues.10
In the present sample, 64% of the patients were over 60 years old. As shown in the literature, the incidence in the elderly is higher due to ultraviolet radiation, which induces somatic mutations leading to aberrant activation of the Hedgehog pathway and the PTCH1 gene over the years in a cumulative manner.20 Thus, the transformation of keratinocytes occurs when the function of multiple oncogenes is affected, leading to dysregulation of the cell cycle.20
In this survey, 31.6% of women had lesions smaller than 1 cm while, among men, this rate was 50%. The statistical analysis between sex and lesions ≥1 cm showed no statistical association between these variables (p=0.63). It was observed that in women over 60 years old, multiple lesions were predominant. It confirms the importance of seeking physical examination for multiple injuries in women of this age group.
Regarding location, 52% of the lesions were in the head and neck and 48% in the trunk. No injuries on the limbs or genitals were observed. When analyzing the location by sex, women presented a predominance of lesions in the head and neck: 57.9% against 42.1% on the trunk in men. These data differ from existing studies that demonstrate a higher prevalence of SBCC in the trunk.11,19,2,12 The predominance of the head and neck can influence the decision of the therapeutic modality chosen to treat these cases. This location is considered noble, and the impact of an unsightly scar can be significant for the patient. The literature shows that SBCC has the highest recurrence rate and requires greater safety margins in conventional surgery for complete excision. It is because this variant has multiple interconnected tumor nests.14,9,15
It was also observed that, in the photoexposed area, 39% of the lesions were non-pigmented. Although they are not the majority, it is crucial to note that many SBCC lesions can be neglected because they do not have pigment and are more similar to other types of lesions, such as eczema and actinic keratosis. On the other hand, this study demonstrated 60% of pigmented lesions in the clinical presentation, which differs from the classic description of SBCC as a well-defined erythematous plaque.6
This study showed structures consistent with what the scientific literature describes for superficial basal cell carcinoma concerning dermoscopic elements. Wosniak-Rito et al. demonstrated that the presence of maple leaf-like structures associated with fine telangiectasias and the absence of arboriform vessels, ovoid nests, and ulceration have a sensitivity of 81.8% and specificity of 81.9% for the diagnosis of SBCC.5 In this study, the anatomopathological study did not confirm the lesions with arboriform vessels and one with ulceration as SBCC, corroborating the data from the current literature. The prevalent dermoscopic elements in this research sample were, in decreasing order: red-whitish areas without structures, maple leaf-like structure, fine telangiectasias, dots/globules, and concentric structures. These data were in line with what was proposed by Wosniak-Rito et al. Aguilar et al. showed a possible correlation of dots and globules with good response to treatment with imiquimod.16
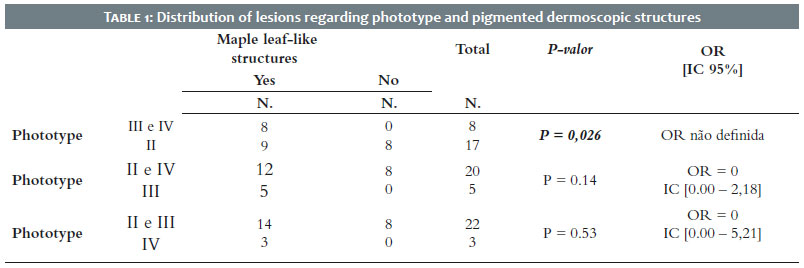
In the statistical analysis between photoexposed area lesions and pigmented dermoscopic structures (maple leaf-like, radiated, and concentric structures, dots and globules),5 there was no statistically significant difference between any of the variables. Therefore, this study didn’t observe any correlation between photoexposure and pigmented dermoscopic structures. It is assumed that this finding derives from the small sample size due to the difficulties imposed by the Covid-19 pandemic that affected the volume of visits to outpatient clinics since March 2020.
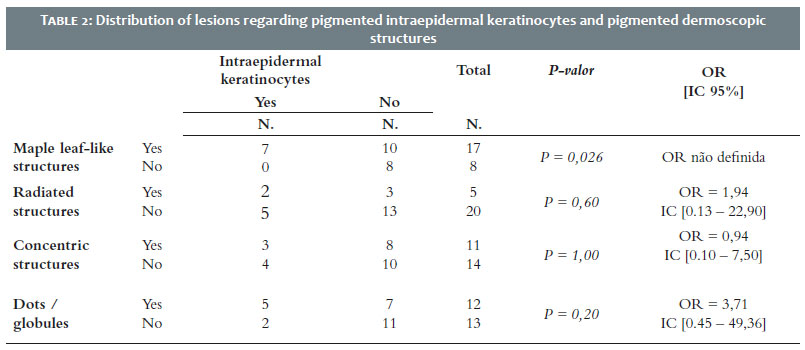
There was a statistically significant correlation between maple leaf-like structures and skin phototype III and IV (p<0.05) as shown in Table 1. The presence of pigmented structures at dermoscopy is likely a property determined by the patient’s intrinsic characteristics, such as high skin phototype, and not due to external factors, such as photoexposure. These data are consistent with the higher incidence of pigmented BCC in non-white individuals.17,2 More studies are needed, however, to establish this correlation. There was no statistically significant correlation for any of the variables in the statistical analysis between the different pigmented dermoscopic structures and the type of melanin pigment present in the anatomopathology.
However, between maple leaf-like structures and intraepidermal keratinocytes with pigment, p=0.057 (Table 2) was obtained, close to the significance level of p<0.05. Yelámos et al. demonstrated that dermoscopic structures are related to tumor nests of basaloid cells at the dermal-epidermal junction.18 Nevertheless, more robust studies with a larger sample can establish a connection between other anatomopathological patterns and dermoscopy, as this study suggests.
Although considered a less aggressive variant, Superficial basal cell carcinoma has an increasing incidence and associated morbidity. This study showed a prevalence of this type of lesion in women and the head and neck. It can influence the choice of appropriate therapy for better clinical and aesthetic responses for patients. In this research, the presence of maple leaf-like structures was related to skin phototypes III and IV. These dermoscopic structures may be correlated with the presence of intraepidermal keratinocytes with pigment. Moreover, this study can be a basis for further prospective research to detail the specific characteristics of superficial basal cell carcinoma.
Bruna Santana Alarcon | 0000-0003-0492-9055
Statistical analysis; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Ana Maria Quinteiro Ribeiro | 0000-0001-9872-0476
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; active participation in research orientation; critical literature review; critical revision of the manuscript.
Jules Rimet Borges | 0000-0002-2215-3281
Approval of the final version of the manuscript; study design and planning; data collection, analysis, and interpretation; active participation in research orientation; critical literature review; critical revision of the manuscript.
Juliana de Souza Couto Eckert | 0000-0001-5104-0406
Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Luiz Fernando Froes Fleury Jr. | 0000-0002-1202-6211
Data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
1. Tanese, K. Diagnosis and management of basal cell carcinoma. Curr Treat Options Oncol. 2019;20(2):13.
2. Chinem VP, Mior HÁ. Epidemiologia do carcinoma basocelular. An Bras Dermatol. 2011;86(2):292-305.
3. Leiter U, Keim U, Garbe C. Epidemiology of skin cancer: update 2019. Adv Exp Med Biol. 2020;1268:123-39.
4. Alter M, Hillen U, Leiter U, Sachse M, Gutzmer R. Current diagnosis and treatment of basal cell carcinoma. J Dtsch Dermatol Ges. 2015;13(9):863-74.
5. Wozniak-Rito A, Zalaudek I, Rudnicka L. Dermoscopy of basal cell carcinoma. Clin Exp Dermatol. 2018;43(3):241-7.
6. Cameron MC, Lee E, Hibler BP, Barker CA, Mori S, Cordova M, et al. Basal cel carcinoma: epidemiology; pathophysiology; clinical and histogical subtypes; and disease associations. J Am Acad Dermatol. 2019;80(2):303-17.
7. Soyer HP, Rigel DS, Wurm EMT. Queratose actínica, carcinoma basocelular e carcinoma de células escamosas. In: Bolognia JL, Jorizzo JL, Schaffer JV, editors. Dermatologia. 3th ed. Rio de Janeiro: Elsevier; 2015. p.1773-94.
8. Sociedade Brasileira de Dermatologia, Miot HA, Penna GO, Ramos AMC, Penna MLF, Schmidt SM, Luz FB, Sousa MAJ, Palma SLL, Sanches Junior JA. Profile of dermatological consultations in Brazil (2018). An Bras Dermatol. 2018;93(6):916-28.
9. Vantuchová Y, Curik R. Histological types of basak cell carcinoma. Scripta medica. 2006;79(5-6):261-70.
10. Mina MA, Picariello A, Fewkes JL. Superficial basal cell carcinomas of the head and neck. Dermatologic Surgery. 2013;38(7):1003-8.
11. Verkouteren JAC, Pardo LM, Uitterlinden AG, Nijsten T. Non-genetic and genetic predictor of a superficial first basal cell carcinoma. J Eur Acad Dermatol Venereol. 2019;33(3):533-40.
12. Chih-Chiang C, Chang-Lin C. Clinical and histopathologic findings of superficial basall cell carcinoma: a comparison with other basal cell carcinoma subtypes. J Chin Med Assoc. 2006;69(8):364-71.
13. Souza CFD, Thomé EP, Menegotto PF, Schimitt JV, Shibue JRT, Tarlé RG. Topografia do carcinoma basocelular e suas correlações com gênero, a idade e o padrão histológico: um estudo retrospective de 1.042 lesões. An Bras Dermatol. 2011;86(2):272-7.
14. Pontes LT, Stelini RF, Cintra ML, Mahalhães RF, Velho PENF, Moraes AM. The importance of superficial basal cell carcinoma in a restrospective study of 139 patients who underwent Mohs micrographic surgery in a Brazilian university hospital. Clinics. 2015;70(11):721-5.
15. Lang Jr PG, McKelvey AC, Nicholson JH. Three-dimensional reconstruction of the superficial multicentric basal cell carcinoma using serial sections and a computer. Am J Dermatopathol. 1987;9(3):198-203.
16. Aguilar JA, Garcés MH, Bayona JIY, Rodríguez MA, Ezquerro IME, Aldecoa-Otalora JS. Dermoscopic signs as predictor of non-responde to imiquimod treatment in superficial basal cell carcinoma. An Sist Sanit Navar. 2019;42(3):303-7.
17. Hougue L, Harvey VM. Basal Cell Carcinoma, Squamous Cell Carcinoma, and Cutaneous melanoma in skin of color patients. Dermatol Clin. 2019;37(4):519-26.
18. Yélamos O, Braun RP, Liopyris K, Wolner ZJ, Kerl K, Gerami P, et al. J Am Acad Dermatol. 2019;80(2):341-63.
19. Pyne JHP, Myint E, Barr EM, Clark SP, David M, Na R, et al. Superficial basal cell carcinoma: a comparison os fuperficial only subtype with superficial combined with other subtypes by age, sex and anatomic site in 3150 cases. J Cutan Pathol. 2017;44(8):677-83.
20. Pellegrini C, Maturo MG, Di Nardo L, Ciciarelli V, Barcía-Rodrigo CG, Fargnoli MC. Undertanding the molecular genetics of basal cell carcinoma. Int J Mol Sci. 2017;18(11):2485.
21. Pereira S, Curado MP, Ribeiro AMQ. Multiple skin neoplasmsin subjects under 40 years of age in Goiania, Brazil. Rev Saude Publica. 2015;49:64.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}