


Karina Bittencourt Medeiros; Guilherme Athanasio Shwetz; Graziela Junges Crescente Rastelli
Received on: 13/07/2020
Approved on: 20/10/2020
Financial support: None
Conflict of interest: None
Study conducted at the Hospital Universitário Evangélico Mackenzie, Curitiba (PR), Brazil.
Acknowledgment: We thank the Dermatology and Pathology Service of Hospital Universitário Evangélico Mackenzie and the patient and his family, who entrusted themselves to our care.
The increase in the incidence of basal cell carcinoma (BCC) affects all age groups, including young patients under twenty years old. Because it is poorly remembered in this group of patients, late diagnosis and treatment of this neoplasia may be more common. Like other age groups, excessive exposure to ultraviolet radiation is the main associated risk factor; however, genetic factors may also be involved in non-syndromic cases. We report a case of BCC on the face of an adolescent treated with Mohs micrographic surgery.
Keywords: Adolescent; Carcinoma, Basal Cell; Epidemiology; Mohs Surgery; Solar Radiation
Basal cell carcinoma (BCC) is the most common malignancy in humans, and its incidence is increasing in recent decades. In Brazil, non-melanoma skin cancer represents 30% of all registered malignant tumors, with an estimate of approximately 176 thousand new cases for 2020.1 Despite the low mortality rates, the tumor may present local invasive behavior and relapse after treatment, causing significant morbidity. Exposure to ultraviolet radiation represents the leading environmental risk factor associated with its genesis. Other factors are also related, such as light skin phototypes, advanced age, family history of skin carcinomas, and immunosuppression, in addition to behavioral aspects, such as a professional activity that requires frequent exposure to the sun, rural activity, and sunburn in youth.2,3,4
This article reports a case of basal cell carcinoma in an adolescent, emphasizing the importance of its diagnosis at an early age.
A 16-year-old man reported a progressive facial lesion for two years. He had previously treated the lesion as nodular acne using topical medications. The patient had no personal history of continuous sun exposure and did not report previous intense acute exposure. He also did not have a family history of skin cancer.
The patient was skin phototype II, and the physical examination showed a 1.5 cm diameter pearly plaque in the left malar region, infiltrated, well delimited, and ulcerated (Figure 1). Dermoscopy revealed arboriform vessels on the lesion’s entire surface, shiny white structures, and ulceration (Figure 2). We also observed grade II acne on the face. The patient did not present any other clinical alterations, such as palmoplantar pitting, breast hypertelorism, changes in the thoracic diameter, and frontal bone prominence. Skull tomography and panoramic radiography of the face, dental arch, ribs, and thorax showed no changes.
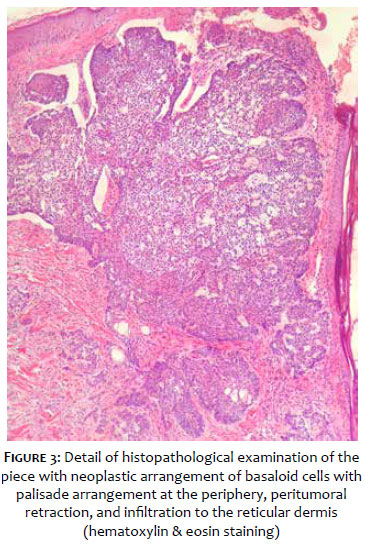
The skin biopsy proved it to be basal cell carcinoma, solid nodular subtype, with an infiltrative growth pattern invading the deep reticular dermis (Figure 3). The patient underwent surgical excision by Mohs micrographic surgery, with free margins in the first stage and closure by a sliding flap (Figure 4), with good evolution and good aesthetic result after six months of evolution (Figure 5).
There is a consensus that BCC incidence is increasing, both in the elderly and in young non-syndromic patients. Individuals under 40 years already account for more than 5% of diagnoses,2 and the hypotheses for this phenomenon are not elucidated.
Greater cumulative exposure to ultraviolet radiation, time available for leisure, unprotected sun exposure, culture of tanning, ozone depletion (2% in the last 20 years), ethnic heritage, and skin phototype (phototypes I and II, for example) are probably the factors that most contribute to the BCC increased incidence.2,3,4
Young patients have more lesions on the trunk, superficial subtype, which are more associated with this type of exposure.5 The habit of sunbathing is linked to five times higher risk of developing BCCs in the trunk.2,5 The reported patient had a lesion on the face, solid nodular subtype, different from the young people’s profile described in the literature.
Genetic factors are associated with the disease’s appearance in young people, especially among syndromic cases, such as xeroderma pigmentosum and basal cell nevus syndrome. Sporadic cases also originate from genetic changes. The literature describes that between 30% and 75% of sporadic cases are associated with the patched hedgehog gene mutation. However, other genetic alterations are also described.4,5
There is a theory that the sebum layer would act as a barrier to ultraviolet rays protecting the skin and preventing the appearance of BCC. Thus, oily and acne-prone skin would present higher protection and a lower incidence of BCC.6 This theory does not fit our case, as the reported patient had oily skin and acne, which may have confused the general practitioner and the patient, delaying the diagnosis.
Men are more affected than women in a 2:1 ratio and with a higher number of lesions, probably due to greater sun exposure.4
The increase in the incidence of this cancer in the younger population can represent growth in all age groups, especially its occurrence in the future older adults, as individuals with a history of BCC are at increased risk of another tumor’s appearance. In five years, approximately 40% of patients will have another BCC lesion.7
As it is increasingly common, it is essential to advance this diagnosis in younger age groups. It would help to avoid delays in diagnosis, such as what happened to our patient who treated the facial lesion for two years as acne. It is crucial to institute preventive sun protection care from early childhood, as they are essential to reduce the future risk of developing BCC.
Karina Bittencourt Medeiros | 0000-0001-8202-6711
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Guilherme Athanasio Shwetz | 0000-0003-2157-6116
Approval of the final version of the manuscript; active participation in research orientation; critical revision of the manuscript.
Graziela Junges Crescente Rastelli | 0000-0002-4235-1410
Data collection, analysis, and interpretation; active participation in research orientation.
1. Inca.gov.br [Internet]. Câncer de pele não melanoma - 2018 [Accessed in 15 de março de 2020]. Available from: http://www2.inca.gov.br/wps/wcm/connect/tiposdecancer/site/home/pele_nao_melanoma.
2. Miot HA, Chinem VP. Epidemiologia do carcinoma basocelular. An Bras Dermatol. 2011;86(2):292-305.
3. Rubin AI, Chen EH, Ratner D. Basal-Cell Carcinoma. N Engl J Med. 2005;353(21):2262-9.
4. Roewert-Huber J, Lange-Asschenfeldt B, Stockfleth E, Kerl H . Epidemiology and aetiology of basal cell carcinoma. Br J Dermatol. 2007;157(2):47-51.
5. Lovatt TJ, Lear JT, Bastrilles J, Wong C, Griffiths CE, Samarasinghe V. et al. Associations between ultraviolet radiation, basal cell carcinoma site and histology, host characteristics, and rate of development of further tumors. J Am Acad Dermatol. 2005;52(3):468-73.
6. Friedman-Birnbaum R, Linn S, Eidlitz-Markus T, Harth Y, Cohen E. Seborrheic skin and acne vulgaris as protective factors against the development of basal cell epithelioma. Dermatologica. 1991;183(3):160-3.
7. Wehner MR, Linos E, Parvataneni R, Stuart SE, Boscardin WJ, Chren MM. Timing of subsequent new tumors in patients who present with basal cell carcinoma or cutaneous squamous cell carcinoma. JAMA Dermatol. 2015;151(4):382-8.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}