


Gustavo Vieira Gualberto; Cassio Ferreira Guimarães; Luisa Coutinho Teixeira; Marina Rodrigues Costa Lages; Guilherme Henrique Silveira Teixeira
Received on: 30/08/2020
Approved on: 06/12/2020
Financial support: None
Conflict of interest: None
Study conducted at the Santa Casa de Misericórdia de Belo Horizonte, Belo Horizonte (MG), Brazil
Blue nail dyschromia has several differential diagnoses. Lesion growth, associated nail dystrophy, and nail extension require evaluation for surgical excision. We report the case of a 27-year-old woman presenting a bluish, semicircular stain, occupying about 50% of the lunula. The patient presented no changes in the overlying lamina, small alteration of the distal nail portion, localized onychoschizia-type layers, and no previous trauma or bleeding history. We performed partial avulsion of the plaque and shave biopsy, evidencing an intensely pigmented lesion. Histopathological examination was compatible with blue nevus. In this case, the nevus should be located in the sub-matricial position, thus not interfering with the nail plate color.
Keywords: Nevus, Blue; Nail diseases; Surgical procedures, Minor; Ambulatory surgical procedures; Nevus, pigmented; Skin neoplasms
Blue nail dyschromia has a wide variety of differential diagnoses, including mainly malignant and benign vascular and melanocytic lesions. Although most of these lesions are benign and have a good prognosis, the presence of lesion growth, associated nail dystrophy, and periungual extension require evaluation for surgical excision.1
Blue nevus of the nail apparatus is a rare entity, with at least 11 cases described in the literature so far. It was first described in 1984 in a 4-year-old child with Klippel-Trenaunay syndrome who had a periungual nodule with satellite lesions on the back of the corresponding hallux and inguinal lymphadenopathy. An examination later showed a blue nevus composed of benign lymph node extension of the nevus component. Sub-matrix presentation (without striated melanonychia) is even rarer.
A 27-year-old woman sought medical consultation complaining of a dark spot in the lunula region of the right first digit for seven years, asymptomatic. Initially, the patient reported that she noticed the spot only when she moved the cuticle away. She observed progressive lesion growth, becoming more evident even without the cuticle removal. The patient also reported a small change of the distal portion of the nail, with localized onychoschizia. She denied a previous history of trauma or bleeding. The physical examination revealed a bluish semicircular macula, occupying approximately 50% of the lunula, without altering the overlying nail plate. Dermoscopy showed a homogeneous bluish background without longitudinal lines (Figure 1). There were no periungual changes, signs of trauma, or axillary lymphadenopathy. The patient reported no previous personal or family history of melanoma.
Due to the inaccurate report of lesion growth and its extension, the nail plate was surgically removed proximally to the nail bed halfway in the longitudinal direction. It evidenced an intensely pigmented, blackened, semicircular, well-delimited lesion with approximately 7 mm in its largest diameter (Figure 2). We opted for the pigmented lesion’s shave excision biopsy to preserve the aesthetic aspect (Figure 3).
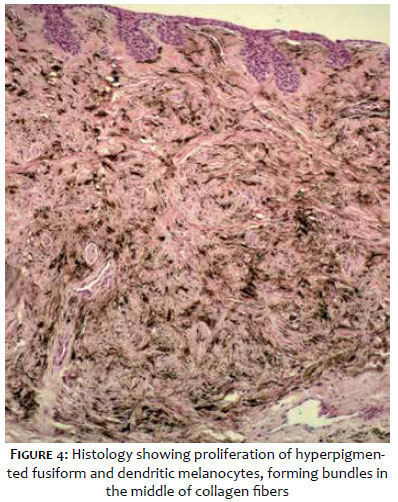
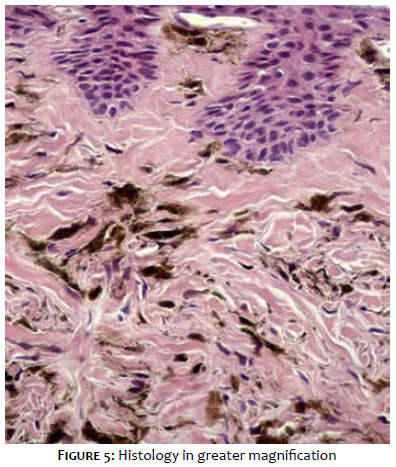
The microscopy observed hyperpigmented spindle and dendritic melanocytes’ proliferation, forming bundles amid collagen fibers and sometimes permeating neural threads and some melanophages. These findings are consistent with blue nevus (Figures 4 and 5). The tissue studied showed no signs of malignancy.
Blue nevus represents a benign proliferation of dermal melanocytes with active melanin production, unlike intradermal nevi and common compound nevi, which produces little or no melanin. The literature suggests that its pathogenesis arises from the interruption of neural crest cell migration in the dermis on the way to the epidermis during embryogenesis. The bluish color of the lesion occurs by preferential absorption of long wavelengths of light by melanin in the dermis, while the skin reflects short wavelengths of the blue spectrum, a phenomenon called the Tyndall Effect.2
Blue nevi can be acquired or congenital and affect preferentially young women. They usually occur on the skin and are rarely reported on extracutaneous sites such as orbital and conjunctival region, oral cavity, esophagus, lymph nodes, vagina, penis, and prostate.3
The blue nevi of the nail apparatus may originate from the matrix, the bed, or the deep periungual dermis. Because they are dermal structures, they usually present as longitudinal melanonychia-like lesions. Pigment-producing nevus cells can incorporate melanin into the nail matrix, leading to a nail-streak formation with brown stripes. The literature suggests that in the case here reported, the nevus would be in a sub-matrix position. Thus, it would not interfere with the lamina’s color and present only as a subungual stain, without longitudinal melanonychia. The bluish color of the lesion is due to the Tyndall effect observed on the translucent nail plate.
The surgical approach of a pigmented lesion in the subungual apparatus is essential to rule out possible differential malignant diagnoses, especially melanoma and its metastatic form. Also, there are reports of malignant transformation of cellular blue nevus. However, the choice of operative conduct must be cautious, as it may lead to permanent dystrophy and functional limitation of the affected digit. In this scenario, one should consider the personal history, the clinical aspect of the lesion, and its dermoscopy. It is also recommended to evaluate any periungual lesions present.
The definition of non-conservative conduct is also based on observing aspects that suggest malignant behavior. Some of them are the presence of longitudinal melanonychia with a thickness higher than 5 mm, irregularities in color, increased thickness of the band distally to proximal, involvement of the first finger, dystrophy of the blade, and periungual pigmentation. Another evidence of malignancy to be highlighted is the report of recent lesion growth.4
Regarding the biopsy technique, removing the lesion only in its periphery should be avoided since the concentration of atypical cells in melanoma is predominant in the central portion of the neoplasia. With complete excision of the lesion, it is uncommon to resort to it. Thus, when clinical recurrence is observed, it is necessary to consider the possibility of malignant transformation, which is a rare event.5
In the presence of a pigmented lesion in the subungual apparatus, the propaedeutic is often based on a clinical-pathological correlation. However, there are factors to be considered to avoid unnecessary intervention resulting in aesthetic and functional impairment.
Gustavo Vieira Gualberto | 0000-0001-5349-2449
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Cassio Ferreira Guimarães | 0000-0002-4328-8994
Preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Luisa Coutinho Teixeira | 0000-0003-4281-1170
Preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review; critical revision of the manuscript.
Marina Rodrigues Costa Lages | 0000-0001-9956-7733
Preparation and writing of the manuscript.
Guilherme Henrique Silveira Teixeira | 0000-0003-0740-6153
Preparation and writing of the manuscript.
1. Gershtenson PC, Krunic A, Chen H, Konanahallj M, Worobec S. Subungual and periungual congenital blue naevus. Australas J Dermatol. 2009;50:144-7.
2. Zembowicz A, Mihm MC. Dermal dendritic melanocytic proliferations: an update. Histopathology. 2004;45:433-51.
3. Murali R, McCarthy SW, Scolyer RA. Blue nevi and related lesions: a review highlighting atypical and newly described variants, distinguishing features and diagnostic pitfalls. Adv Anat Pathol. 2009;16:365-82.
4. Ronger S, Touzet S, Ligeron C, et al. Dermoscopic examination of nail pigmentation. Arch Dermatol. 2002;138:1327-33.
5. Murali R, McCarthy SW, Scolyer RA. Blue nevi and related lesions: a review highlighting atypical and newly described variants, distinguishing features and diagnostic pitfalls. Adv Anat Pathol. 2009;16(6):365-82.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}