


Juliano Cesar de Barros; Isabella Parente Almeida; Jefferson Alfredo de Barros; Andrés Maurício Lopez Munoz; Carlos D'Apparecida Santos Machado Filho
Received on: 23/08/2020
Approved on: 06/12/2020
Financial support: None
Conflict of interest: None
Study conducted at the Faculdade de Medicina do ABC, São Paulo (SP), Brazil
INTRODUCTION: Vitiligo is an acquired skin dyschromia characterized by the physical and/or functional reduction of melanocytes. We present two surgical proposals for the treatment of vitiligo.
CASE REPORTS: 1) Implant of skin graft diluted in hyaluronic acid gel: We obtained the material through curettage, diluted it in hyaluronic acid gel, and applied it to receptor areas. 2) Epidermal suspension obtained through curettage and diluted in hyaluronic acid gel: After the curettage of the donor area, we treated the material with trypsin-EDTA, centrifuged it, and diluted it in hyaluronic acid gel. The receptor area received the graft.
CONCLUSION: These are safe, easy, and satisfactory surgical procedures for the presented cases.
Keywords: Vitiligo; Keratinocytes; Ambulatory surgical procedures
Vitiligo is an acquired, idiopathic cutaneous dyschromia characterized by physical and functional reduction of melanocytes. The global prevalence is around 0.5% to 1%. Clinically, it presents achromic macules and patches of different sizes and forms.1 Stable vitiligo cases resistant to clinical treatment are candidates for surgical treatment, including non-cultured epidermal suspension grafts treated enzymatically with trypsin 0.25%; thin dermo-epidermal skin grafts; suction blister epidermal grafts (SBEG); total punch grafting; epidermal grafting or in vitro isolation; and culture of melanocytes.2,3
Additionally, Machado (2000)3 demonstrated the feasibility of obtaining material for grafting through simple epidermal curettage of the donor area to be implanted in a recipient area, also curetted. The obtained graft is humidified with physiological saline to obtain a “paste”; it is applied to the recipient area and fixed with an adhesive semi-permeable membrane.
The present article describes two surgical techniques for treating vitiligo, considering variations of the curettage technique used for obtaining the graft from the donor area.
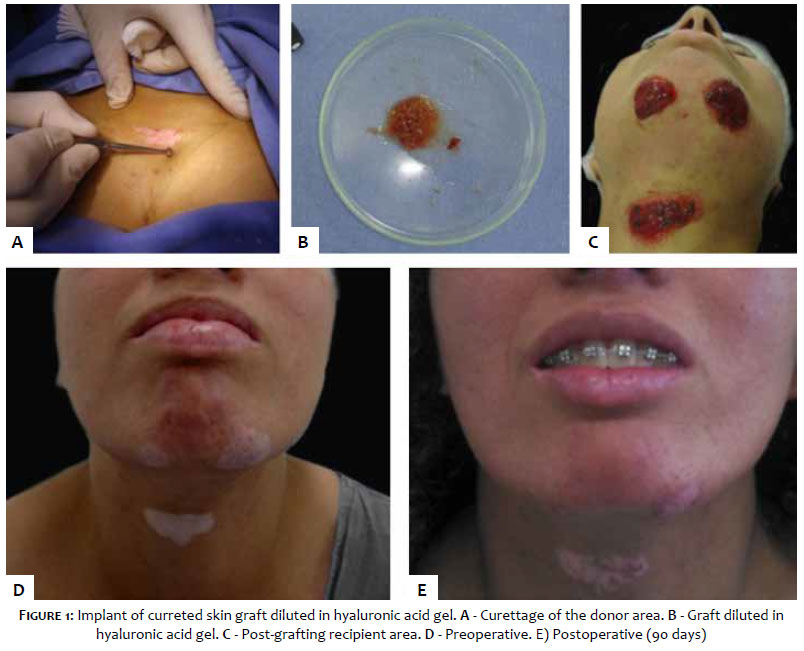
The technique’s characteristic is the dilution of the obtained graft in a gel of hyaluronic acid. This biocompatible and hygroscopic substance provides greater viability and adhesion to the receptor area.4 The curettage of the donor area to the papillary dermis obtains the material (Figure 1A). It is then diluted in 1-2 ml of hyaluronic acid gel at 0.5-2% (Figure 1B) (Figure 1B). The recipient area is also curetted reaching the papillary dermis and obtaining the same size as the donor area. Finally, the graft is applied over the recipient area (Figure 1C) and covered with a dressing of porous membrane of cellulose, maintained in site for seven days. Topical medications and phototherapy are reintroduced 14 days after the procedure. Satisfactory results are observed after 90 days (Figure 1D and 1E).
It corresponds to the association of the techniques curettage grafting and uncultured epidermal suspension methods. Mulekar (2003 and 2005)5,6 and van Geel (2001)2 initially described the use of hyaluronic acid in epidermal suspensions. After curettage of the donor area until the onset of the papillary dermis’s punctate bleeding, the collected graft is exposed to a proteolytic solution (Trypsin EDTA 0.025% - LGC Biotechnology™ - Brazil) and incubated for 20 minutes at 98.6º Fahrenheit. After incubation, a pipette aspirates the trypsin. The sample is then washed with 0,9% saline solution and transferred to a centrifuge tube containing the DMEM culture medium (LGC Biotechnology™ - Brazil). After six minutes of centrifuging at 1500 rpm, the supernatant of epidermal cells is discarded, and the pellet is suspended in 1-2 m of hyaluronic acid gel 0.5-2% (Paulista Center for Pharmaceutical Development™ - Brazil). The suspension concentration, which can vary according to the clinical case of vitiligo, generates a donor to receptor area ratio ranging between 1:10 to 1:20. The recipient area is curetted or dermabrased to the papillary dermis. After applying the epidermal graft, it is occluded with a porous cellulose membrane, which should remain on the site for seven days. The topical medications and phototherapy should be reintroduced after 14 days. Satisfactory results are observed after 90 days and improve 180 days after the procedure (Figures 2A and 2B).
In conclusion, curetting the skin until the papillary dermis is an affordable procedure, easy to perform, which provides a satisfactory sample for grafting. When this technique is associated with hyaluronic acid, it allows greater viability and adherence of the graft to the recipient area. Nowadays, there are not indexed publications of those described techniques, and future studies are necessary for further elucidation and improvement of these treatment modalities.
We thank the patients and the Nursing staff: it would not be possible to conduct this study without them.
Juliano Cesar de Barros | 0000-0003-1494-7118
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Isabella Parente Almeida | 0000-0002-6283-4065
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Jefferson Alfredo de Barros | 0000-0001-5073-0747
Study design and planning; data collection, analysis, and interpretation; active participation in research orientation.
Andrés Maurício Lopez Munoz | 0000-0003-2319-2351
Study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Carlos D'Apparecida Santos Machado Filho | 0000-0003-4362-1563
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; critical literature review; critical revision of the manuscript.
1. Singh C, Parsad D, Kanwar AJ, Dogra S, Kumar R. Comparison between autologous noncultured extracted hair follicle outer root sheath cell suspension and autologous noncultured epidermal cell suspension in the treatment of stable vitiligo: a randomized study. Br J Dermatol. 2013;169(2):287-93.
2. Van Geel N, Ongenae K, Nayaert JM. Surgical techniques for vitiligo: a review. Dermatology. 2001;202(2):162-6.
3. Machado C. (2000). Vitiligo: áreas tratadas por enxertia com raspado cutâneo e estudo da reação de polimerase em cadeia de RNA mensageiro de tirosinase por transcriptase reversa. (Tese de Doutorado). São Paulo: Universidade Federal de São Paulo.
4. Van Geel N, Ongenae K, De Mil M, Nayaert JM. Modified technique of autologous noncultured epidermal cell transplantation for repigmenting vitiligo: a pilot study. Dermatol Surg, 2001;27(10):873-6.
5. Mulekar SV. Melanocyte-keratinocyte cell transplantation for stable vitiligo. Int J Dermatol, 2003;42:132-6.
6. Mulekar SV. Long-term follow-up study of 142 patients with vitiligo vulgaris treated by autologous, noncultured melanocyte-keratinocyte cell transplantation. Int J Dermatol. 2005;44(10):841-5.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}