


Flávio Barbosa Luz; Lara Assunção Kriger
Received on: 04/11/2020
Approved on: 26/11/2020
Financial support: None
Conflict of interest: None
Study conducted at the Universidade Federal Fluminense, Niterói (RJ), Brazil
INTRODUCTION: Axillary bromhidrosis is a disease of significant psychosocial impact characterized by bad odor in the armpits. The cause of bromhidrosis is multifactorial, and studies indicate that it is related to the bacterial transformation of substances secreted by the apocrine glands. Some cases of bromhidrosis are difficult to control by clinical therapies, and surgical therapies are well indicated. Surgical treatments for the disease aim to remove the axillary sweat glands and range from more aggressive to minimally invasive procedures. This review aims to list and compare all surgical alternatives described in the medical literature.
Keywords: Surgical Procedures, Operative; Sweat Glands; Hyperhidrosis; Apocrine Glands
Axillary bromhidrosis is a common condition that can cause severe social obstacles to the individual.1 Osmidrosis is characterized by the foul odor produced by the bacterial decomposition of the secretion emitted mainly by the apocrine glands. Hyperhidrosis is a condition of excessive sweat linked to the eccrine glands. Bromhidrosis is the sum of hyperhidrosis and osmidosis.1
There are three types of sweat glands: apocrine, eccrine, and apoeccrine.2 Apocrine glands are present in specific areas of the body, such as the armpits, genitalia, scalp, periorbital area, and ear canals. They secrete a small amount of odorless fluid that undergoes bacterial decomposition upon reaching the skin, which makes it odorous. Eccrine glands have their own characteristic. The re-absorbent duct opens directly to the skin surface, and its secretory portion produces a solution rich in NaCl, directly related to axillary hyperhidrosis. Apoeccrine glands become apparent in the 8-14 age range and appear to be closely associated with excessive sweating (hyperhidrosis).1
We collected the scientific articles in the PubMed and Web of Science databases using the terms “axillary bromhidrosis” and “surgery”. We selected articles published between 1972 and 2019 (the oldest ones are related to the surgical technique of axillary skin with the adjacent subcutaneous tissue resection) in English and Spanish.
All abstracts were read, and the articles to be inserted contained relevant information on surgical therapies and bromhidrosis etiopathogenesis. As bromhidrosis’s surgical treatment is very similar to hyperhidrosis, this review also used articles on the latter condition. Some articles were discarded for not bringing any novelty compared to the others already selected.
Axillary bromhidrosis is a common disease, underdiagnosed and undertreated, affecting social interactions too much and reducing patients’ quality of life. According to the conception that clinical treatments usually have satisfactory effects only in mild cases, surgical approaches are of paramount therapeutic importance. Due to the low number of studies that standardize these interventions, the present review aims to list such techniques, reinforcing the positive and negative aspects for a better possibility of therapeutic choice.
Axillary bromhidrosis is a disease with severe psychosocial impacts on the individual, interfering with their daily activities. Patients with more severe symptoms consider it intolerable or almost intolerable. The Dermatology Life Quality Index (DLQI) of patients with axillary hyperhidrosis was analyzed, and the result was compared with other dermatological problems, such as acne, birthmarks, pruritus, psoriasis, and eczema. The results indicated that hyperhidrosis was associated with a lower quality of life when compared to other diseases.3 It is believed that bromhidrosis can often be an even more embarrassing condition when compared to hyperhidrosis, in addition to the frequent overlap between the two entities.
The etiology of bromhidrosis is multifactorial, but the leading causes are its intimate relationship with axillary hyperhidrosis, the composition of the sweat secreted by the apocrine glands, and the degradation of these components by microorganisms present in the axillary skin, in addition to genetic and dietary factors.
The foul odor comes from transforming non-odorous substances secreted by the apocrine, eccrine, and sebaceous glands into volatile and odorous substances. The axillary microbiota consists mainly of gram-positive bacteria of the genera Staphylococcus, Micrococcus, Propionibacterium, and Corynebacterium, which is the primary cause of the foul odor, whose substrate originates from the apocrine glands.4
Volatile fatty acids and thioalcohols are mainly responsible for the foul axillary odor, while steroids, although they contribute, are not so relevant in this process. Medium-chain volatile fatty acids (C6-C10), in particular the trans (E) isomer of 3-methylhex-2-enoic acid (3M2H), have a significant contribution to axillary foul odor. It is linked to the amino acid L-glutamine in the secretion of apocrine glands, and the action of a Corynebacterium enzyme releases it.5 It was later discovered that an ABCC11 gene allele is essential for the secretion of L-glutamine conjugated to E-3M2H.6
The volatile fatty acids that cause the foul axillary odor are short-chain (C2-C5) and medium-chain (C6-C10). Propionibacterium and Staphylococcus ferment glycerol from the hydrolysis of triacylglycerol, and lactic acid present in the skin, transforming them into acetic and propionic acid. Regarding steroids, 16-androstenes, 5a-androstenol, and 5a-androstenone are present in the sweat of the apocrine glands and have already been significantly associated with a foul odor. However, it is known today that axillary bacteria can only produce 16-androstenes from precursors containing C16 with a double bond.4
Laboratory studies have identified four thioalcohols involved in foul axillary odor. These represented two groups of isomers, molecular weight 120-u, and 134-u. The first isomer has an unpleasant smell, comparable to meat or onion, characteristic of the foul axillary odor. The other is a less pronounced odor occasionally related to fruits. The less foul odor of the 134-u isomer was identified as 3-mercaptohexan-1-ol. The odor compared to meat or onion (120-u) was confirmed as 2-methyl-3-mercaptobutan-1-ol. Later, other thioalcohols were also identified, such as 3-mercaptopentan-1-ol (probably equivalent to the least odorous, isomer 120-u), and 3-methyl-3-mercaptohexan-1-ol (molecular weight 148-u), identified and associated with the foul odor. In conclusion, there is vast evidence that, together with medium-chain fatty acids, such as 3M2H and 3-hydroxy-3-methylhexanoic acid, the primary molecules cause axillary odor.4
The starting point for understanding human odor came from the study of cerumen (ear wax), which is a product of the ceruminous apocrine glands. The study investigates the polymorphism of a nucleotide of the ABCC11 gene, which encodes an ATP-driven pump and is responsible for determining the cerumen (the AA genotype corresponds to the dry cerumen and the GA and GG genotype to the wet cerumen, which is dominant over the other). Thus, the study proposed that wet cerumen relates to a strong axillary odor and dry cerumen to a less pronounced aroma.7
The apocrine glands secrete long-chain fatty acids, fatty acids linked to amino acids, sulfur compounds, and hormones, which have too long chains to be volatile. The bacteria (mainly Staphylococcus and Corynebacterium spp.) break down these compounds into smaller ones, which become volatile and have a noticeable odor.8 These bacteria are distributed both on the skin and below the surface, mainly in the glandular structures, hair follicles, and ducts of these glands. It seems to explain why topical treatments of bromhidrosis that interfere with bacterial colonization tend to be ineffective since they only affect bacteria present on the axillary surface, with rapid recolonization, especially of the attachments.
Often, the use of deodorants and antiperspirants by individuals who have bromhidrosis can be harmful since it can increase bacteria’s diversity and select those primarily responsible for the foul odor. It subsequently leads to intense colonization by such bacteria.8 When clinical treatments do not show satisfactory results, there are options for local surgery with the main objective of removing the apocrine.
Local surgeries for axillary hyperhidrosis (also applicable to bromhidrosis) can be divided into three main groups:9
1. Resection of glandular tissue without excision of the skin (only surgical incision to access the subcutaneous glandular tissue);
2. Axillary skin with adjacent subcutaneous tissue resection;
3. Combination of the two methods resulting in a partial resection of the skin associated with the subcutaneous tissue and adjacent tissues excision.
We will approach these three major groups in chronological order.
Axillary skin with adjacent subcutaneous tissue resection
They are more invasive techniques and with higher morbidity and risk of complications.
It is the most radical surgical technique and, consequently, the one with a higher chance of complications, mainly related to healing and arm movement limitation. Based on the cases in which this technique was performed, high rates of complications were observed, such as infection, bleeding, poor healing, and necrosis, the most common being: wound dehiscence, partial necrosis, and prolonged healing with subsequent formation of adhesions.10
A less invasive alternative to this surgical technique consists of an elliptical excision removing the skin and subcutaneous tissue, containing the sweat glands only in the axillary dome. This method decreases sweating caused by the eccrine glands by up to 80%.11
Combination of the two methods resulting in a partial resection of the skin associated with the subcutaneous tissue and adjacent tissues excision
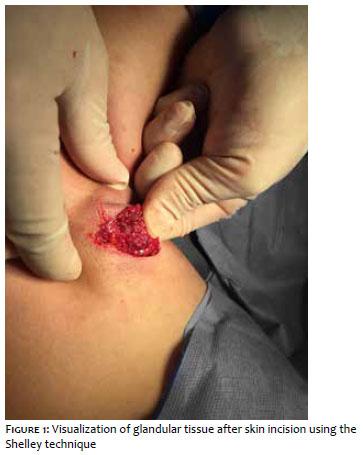
The primary surgical method used to perform this combination of methods is the famous Shelley technique,12 which consists of a central elliptical excision in the armpit until reaching the fat portion. The lesion margins are everted, and the glandular tissue (containing the eccrine and apocrine glands - Figure 1) is removed along with the dermis and subcutaneous tissue using surgical scissors (Figure 2). The wound is closed using subcutaneous sutures attached to the underlying axillary fascia to obliterate spaces with high chances of bruising (it is also possible that the suture is superficial, as preferred by the surgeon). Occlusive dressing is usually left for 24 hours. Due to the higher infection rates of this surgical technique compared to the others, chlorhexidine solution can be applied before and after the procedure, in addition to prophylactic antibiotics, which the surgeon must evaluate according to the needs of each patient.12
It is important to note that there are several variations of the standard technique. For example, a study conducted with 63 patients to assess the surgical procedure’s effectiveness to treat axillary bromhidrosis used a method similar to that described above. Still, the superficial fascia was also dissected and removed. Of the 126 operated armpits, bromhidrosis was eradicated in 112 and markedly reduced in 14, with necrosis in only three operated armpits.13
Another study with 15 patients14 operated the armpits using another technique slightly modified from the Shelley technique. The study delimited the sweat area by examining it in bright light to identify and mark the maximum sweat area’s extent instead of using Minor’s starch-iodine test. An average sweating reduction rate greater than 60% could be achieved.14
Another modification of the Shelley’s method appears with the technique “pinch and turn-over” the exposed flap,15 maneuver that significantly facilitates removing the glands. However, comparing the photos in this article with those by Lawrence et al. (2006), there seems to be no novelty in this technique.
Li et al., in 2015, modified the Shelley technique by making two parallel incisions in each armpit instead of one and excising the apocrine glands preserving the superficial axillary fascia. Its results in 115 patients were very encouraging, suggesting that this may be a surgical procedure with a lower recurrence rate, a significant odor reduction, and fewer complications. No necrosis was reported, 112 patients had eradication of bromhidrosis, and three achieved substantial reduction.16
A study conducted with 396 patients 17 used a technique similar to the Shelley’s, presented that 87.1% of the patients achieved very satisfactory results, 7.8% obtained moderately satisfactory results, and 5.1 % were unsatisfactory due to complications and persistent underarm odor. The complications observed were hematomas, necrosis, infection, wound dehiscence, rippled skin, comedone, cyst, keloid. A possible explanation for the return of the foul odor is that, as the surgery removes only the most superficial tissue of fat and deep dermis, some portion of the apocrine glands may remain in the region and regenerate.17
Resection of glandular tissue without excision of the skin
With the emergence of new minimally invasive therapeutic options, this type of surgery can be subdivided into three: superficial liposuction, aspiration curettage, and simple curettage. The first one predominantly removes the subcutaneous tissue; the other two resects the subcutaneous tissue and deep dermal tissue.
When choosing the best technique to be performed, one must consider the difference between the eccrine glands’ bromhidrosis). The eccrine glands are located more superficially in the dermis, while the apocrine glands extend from the deep dermis to the subcutaneous tissue. As the reticular dermis is composed of dense and irregular connective tissue, removing apocrine glands attached firmly to the deep dermis is technically more complicated than those located in the subcutaneous tissue.18 Therefore, although there is no consensus, histological studies 19,20 demonstrate that the eccrine glands are dominant in the dermis, and most of the apocrine glands are located in the subcutaneous tissue.
1) Aspiration curettage
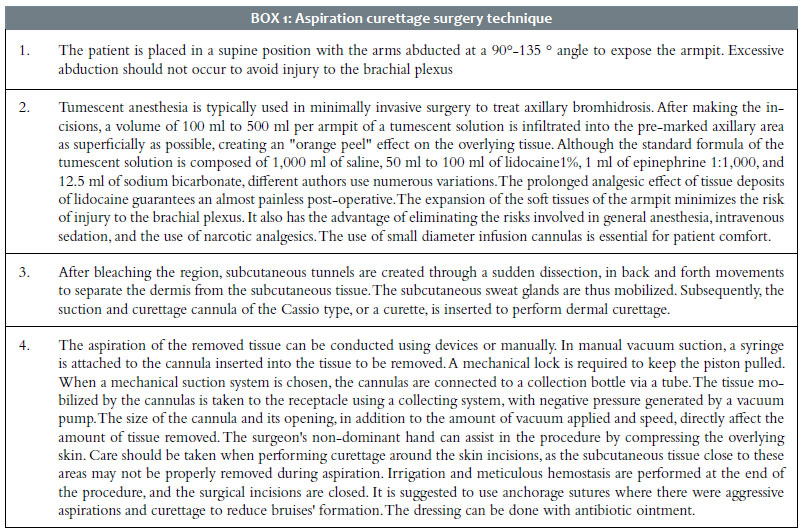
The procedure consists of two main parts: dissection of the dermis from the underlying subcutaneous tissue followed by removing the sweat glands from the dermo-hypodermic junction and the deep dermis. For surgical access, two or three small incisions are made outside the area to be curetted. The surgeon can make the incision, according to their preference, in different locations: superomedial concerning the armpit, in the anterior and distal edges, in the upper internal region of the arm, and the central portion of the armpit.21 Chart 1 describes in detail the technique, according to Rezende et al.21
According to Rezai, aspiration curettage has a sweating recurrence rate of 20% to 40%. However, with the innovation of surgical methods and instruments, the rates have decreased to less than 6%.22
2) Simple curettage
Unlike aspiration curettage, this surgical technique consists of curettage of the axillary region without aspiration. The purpose of this procedure is also the selective removal of the sweat glands. The anesthesia used is usually tumescent.
This technique’s main steps are the surgical incision made through the skin to the subcutaneous tissue. Subsequently, dermal tunneling can be done using a curette for scraping, with back and forth movements. This movement occurs until most of the tissue blocks containing the destroyed sweat glands, adipose tissue, and other skin attachments are eliminated.18
Curettage should be performed both on the superficial layer of the subcutaneous tissue and in the deep dermis to remove the sweat glands (Figure 3) and, inevitably, some other tissues, especially the hair follicles.23
According to Field, 2003, even though patients are informed about increased risks with a more invasive procedure, they prefer to undergo more aggressive surgery expecting a higher chance of curing their condition.24
However, surgeons should be alert to the fact that curettage should be performed in a way that generates the best possible results but with the least amount of complications. 21
The interruption of curettage varies according to the perceptions of each author. However, the main parameters are skin thickness (Figures 4 and 5); skin color (a pale violet - Figure 6); complete elevation of the axillary skin of the subcutaneous tissue; “skin to skin” sliding, demonstrating that there is no more fat adhered to the dermis; palpable hair follicles during the “skin to skin” sliding; sound similar to sipping caused by the cannula; visualization of the curette by transparency (Figure 7); and easy removal of the axillary hair when pulled slightly by the surgeon.21
According to Bechara et al. (2008), the use of cannulas with sharp edges is more effective than other less aggressive or blunt cannulas. According to these authors, combining two types of cannulas can lead to extensive damage to the skin and the dermal vascular plexus.25
3) Superficial liposuction
Usually, the technique consists of two small incisions (3 mm to 4 mm each). Dermal tunneling is performed, and the junction of the dermis with the subcutaneous tissue is aspirated with a cannula. There is the possibility of starting the procedure with a cannula and, after the subcutaneous tissue is very thin, one with an opening more suitable for subdermal scraping, for example, can replace it. A firm handgrip can stabilize the underlying skin and control the depth the cannula reaches. A thin axillary skin wholly separated from the underlying tissue characterizes the end of the procedure.26-28
The main element that leads to bromhidrosis is the bacterial degradation of compounds secreted by the apocrine glands. Also, dietary compounds can contribute to underarm odor, such as tomatoes.29
Also, contradicting the idea that only adults suffer from bromhidrosis, a study diagnosed six-year-old twin sisters with axillary bromhidrosis,30 which brings an interesting discussion about the age group of the disease.
Regarding the treatments, there are conservative ones, such as topical agents and botulinum toxin, which have a temporary effect and need a periodic application, and those that are comparatively more permanent and radical, such as surgical techniques.31
The main objective of bromhidrosis’s surgical treatment is the removal of apocrine glands and some local eccrine glands. Eccrine glands are dominant in the dermis, and apocrine glands are mostly located in the subcutaneous tissue.18 The apocrine glands are composed of the secretory portion and the excretory duct.1 These glandular segments are connected, and part of the secretory portion is firmly attached to the lower portion of the dermis.32
Consequently, it is relevant to consider these sweat glands’ location in the choice and application of the surgical technique. The surgeries developed for the treatment of axillary bromhidrosis are based on the apocrine glands’ site, so eliminating the subcutaneous tissue is effective.33
It is important to emphasize that selecting the surgical method must also be based on individual characteristics, such as the sweat pattern, bromhidrosis severity, reduced degree of the axillary odor and sweating that the patient wants, and their preference regarding the scar and axillary hair loss.32
Regarding surgical methods, superficial liposuction has greater difficulty in eradicating the apocrine glands. It is indicated primarily for patients concerned with the scar and who can tolerate some residual odor and sweating.32
Curettage also proves to be effective because the technique causes mechanical trauma leading to degeneration and necrosis of the apocrine glands during the back and forth movement of the curette, consequently eliminating possible remaining glands.31
However, there is no consensus on which surgery should be employed. Although the most radical surgeries are very effective, some minimally invasive surgeries (such as aspiration and/or curettage) can be therapeutic options as good as the radical ones but with better aesthetic results and fewer complications.9
It is essential to highlight that, despite its high efficacy, the complete resection of the axillary skin with the adjacent subcutaneous tissue excision is considered very aggressive. This method was practically abandoned due to the increased possibility of complications, such as infections, bleeding, necrosis, poor healing or scar contracture, and movement limitation.
Different surgical techniques are described for treating axillary bromhidrosis, with no standardization or consensus on which is the most effective. More radical methods are considered more effective, but there are reports of more frequent complications. Techniques that remove glandular tissue without skin resection have a low complication rate and relevant therapeutic success.
Flávio Barbosa Luz | 0000-0001-5454-8950
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Lara Assunção Kriger | 0000-0003-0537-5402
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; critical revision of the manuscript.
1. Mao G-Y, Yang SL, Zheng JH. Etiology and management of axillary bromidrosis: a brief review. Int J Dermatol. 2008;47(10):1063-8.
2. Sato K, Leidal R, Sato F. Morphology and development of an apoeccrine sweat gland in human axillae. Am J Physiol. 1987;252(1 Pt 2):R166-80.
3. Cetindag IB, Boley TM, Webb KN, Hazelrigg SR. Long-term results and quality-of-life measures in the management of hyperhidrosis. Thorac Surg Clin. 2008;18(2):217-22.
4. James AG, Austin CJ, Cox DS, Taylor D, Calvert R. Microbiological and biochemi-cal origins of human axillary odour. FEMS Microbiol Ecol. 2013;83(3):527-40.
5. Natsch A, Kuhn F, Tiercy JM. Lack of evidence for HLA-linked patterns of odorous carboxylic acids released from glutamine conjugates secreted in the human axilla. J Chem Ecol. 2010;36(8):837-46.
6. Martin A, Saathoff M, Kuhn F, Max H, Terstegen L, Natsch A. A functional ABCC11 allele is essential in the biochemical formation of human axillary odor. J Invest Dermatol. 2010;130(2):529-40.
7. Hamada K, Haruyama S, Yamaguchi T, Yamamoto K, Hiromasa K, Yoshioka M, et al. What determines human body odour? Exp Dermatol. 2014;23(5):316-7.
8. Callewaert C, Lambert J, Van de Wiele T. Towards a bacterial treatment for armpit malodour. Exp Dermatol. 2017;26(5):388-91.
9. Bechara FG, Sand M, Hoffmann K, Boorboor P, Altmeyer P, Stuecker M. Histologi-cal and clinical findings in different surgical strategies for focal axillary hyperhidrosis. Dermatol Surg. 2008;34(8):1001-9; discussion 1009.
10. Bretteville-Jensen G. Radical sweat gland ablation for axillary hyperhidrosis. Br J Plast Surg. 1973;26(2):158-62.
11. Santos GJ, Rivera R, Galindo TA, Ramirez M. Surgical treatment of axillary hype-rhidrosis. Plast Reconstr Surg. 1972;49(5):588.
12. Hussain AB, Holme SA, Kavanagh GM. Shelley procedure in axillary hyperhidro-sis. Clin Exp Dermatol. 2016;41(2):229-31.
13. He J, Wang T, Dong J. Excision of apocrine glands and axillary superficial fascia as a single entity for the treatment of axillary bromhidrosis: a modified surgical trea-tment for bromhidrosis. J Eur Acad Dermatol Venereol. 2012;26(6):704-9.
14. Lawrence CM, Lonsdale Eccles AA. Selective sweat gland removal with minimal skin excision in the treatment of axillary hyperhidrosis: a retrospective clinical and histological review of 15 patients. Br J Dermatol. 2006;155(1):115-8.
15. Lee ET. Shortening of Incision by "Pinch and Turn-Over Technique" in the treatment of axillary osmidrosis. Aesthetic Plast Surg. 2019;43(1):267-77.
16. Li ZR, Sun CW, Zhang JY, Qi YQ, Hu JZ. Excision of apocrine glands with preser-vation of axillary superficial fascia for the treatment of axillary bromhidrosis. Dermatol Surg. 2015;41(5):640-4.
17. Zhao H, Li S, Nabi O, Hu L, Gao X, Luo F. Treatment of axillary bromhidrosis through a mini-incision with subdermal vascular preservation: a retrospective study in 396 patients. Int J Dermatol. 2016;55(8):919-25.
18. Wang R, Yang J, Sun J. A minimally invasive procedure for axillary osmidrosis: subcutaneous curettage combined with trimming through a small incision. Aesthetic Plast Surg. 2015;39(1):106-13.
19. Bisbal J, del Cacho C, Casalots J. Surgical treatment of axillary hyperhidrosis. Ann Plast Surg. 1987;18(5):429-36.
20. Rigg BM. Axillary hyperhidrosis. Plast Reconstr Surg. 1977;59(3):334-42.
21. Rezende RM de, Luz FB, Rezende RM de, Luz FB. Surgical treatment of axillary hyperhidrosis by suction-curettage of sweat glands. An Bras Dermatol. 2014;89(6):940-54.
22. Rezai K. Suction curettage of the sweat glands--an update. Dermatol Surg. 2009;35(7):1126-9.
23. Rompel R, Scholz S. Subcutaneous curettage vs. injection of botulinum toxin A for treatment of axillary hyperhidrosis. J Eur Acad Dermatol Venereol. 2001;15(3):207-11.
24. Field LM. Tumescent axillary liposuction and curretage with axillary scarring: not an important sequela. Dermatol Surg. 2003;29(3):317.
25. Bechara FG, Sand M, Hoffmann K, Altmeyer P. Aggressive shaving after combined liposuction and curettage for axillary hyperhidrosis leads to more complications without further benefit. Dermatol Surg. 2008;34(7):952-3.
26. Perng CK, Yeh FL, Ma H, Lin JT, Hwang CH, Shen BH, et al. Is the treatment of axillary osmidrosis with liposuction better than open surgery? Plast Reconstr Surg. 2004;114(1):93-7.
27. Lillis PJ, Coleman WP. Liposuction for treatment of axillary hyperhidrosis. Dermatol Clin. 1990;8(3):479-82.
28. Ou LF, Yan RS, Chen IC, Tang YW. Treatment of axillary bromhidrosis with su-perficial liposuction. Plast Reconstr Surg. 1998;102(5):1479-85.
29. Stewart JCM. Tomatoes cause under-arm odour. Med Hypotheses. 2014;82(5):518-21.
30. Hasfa S, Schwartz RH. Two 6-Year-Old twin girls with primary axillary bromhidrosis: discussion, differential diagnosis, and management options. Clin Pediatr (Phila). 2007;46(8):743-5.
31. Lee D, Cho SH, Kim YC, Park JH, Lee SS, Park SW. Tumescent liposuction with dermal curettage for treatment of axillary osmidrosis and hyperhidrosis. Dermatol Surg. 2006;32(4):505-11; discussion 511.
32. Park, D. H. Treatment of axillary bromhidrosis with superficial liposuction. Plast Reconstructive Surg. 1998;102(5):1479-85.
33. Van TN, Manh TN, Minh PPT, Minh TT, Huu ND, Cao KP, et al. The effectiveness of local surgical technique in treatment of axillary bromhidrosis. Open Access Maced J Med Sci. 2019;7(2):187-91
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}