


Célia Luiza Petersen Vitello Kalil1; Clarissa Prieto Herman Reinehr2
Received on: 22/06/2020
Approved on: 01/12/2020
Financial support: None
Conflict of interest: None
Study conducted at the Dermatological Clinic Célia Kalil, Porto Alegre (RS), Brazil
Q-switched lasers are widely used for tattoo removal. A 48-year-old-woman with a black tattoo on the left thigh was submitted to ten sessions of Q-switched Nd:YAG 1064nm laser associated with fractional CO2 laser, performed every two months. Six months after treatment end, we observed almost complete tattoo removal, besides improvement in skin texture. Q-switched lasers promote tattoo removal by a photoacoustic phenomenon. The association with fractional ablative lasers is an option for intensely pigmented tattoos or for tattoos with several colors, which are hard to remove.
Keywords: Laser Therapy; Lasers; Tattooing
The search for effective tattoo removal methods that do not result in the formation of unsightly tattoos when removing the pigment requires constant dermatologist improvement to deliver the best possible results. The tattooing art is ancient and consists of injecting pigment particles into the dermis to ensure a permanent tattoo. Approximately 5% of all people who get tattoos will want to remove them at some point in their lives.1 Currently, Q-switched lasers are the most used for tattoo removal.2
A 48-year-old woman underwent consultation due to a black tattoo on her left thigh. The tattoo consisted of a completely black rectangular area, made to correct the skin graft donor area’s coloration. According to the patient, the chosen color should simulate the skin tone of her skin phototype IV. However, the responsible tattoo artist made a mistake in selecting colors and inadvertently used black (Figure 1). The patient also presented scars on her thigh, knee, and right leg due to an accident. We decided to treat the areas with an ablative fractional CO2 laser and Acroma Q-switched laser Nd:YAG 1064nm.
We conducted a total of ten sessions. Before each session, topical and infiltrative anesthesia of the area to be treated with lidocaine 1% combined with vasoconstrictor diluted with saline (1:1) was performed due to the extent of the lesion and not to exceed the maximum dose of topical anesthetic considered safe.
From the first to the tenth session, the Acroma Q-switched Nd:YAG 1064nm laser, Etherea MX platform, Vydence Medical®, was associated (in the first session starting with the Acroma 1064nm laser, 5mm spot size, 900mJ in the first pass and 1200mJ in the second pass; the second session used the 3mm spot size with 600mJ energy, followed by the increase of energy to 900mJ in the third session, and to 1200mJ from the fifth session onwards), to the ablative fractional CO2 laser (Sculptor, Vydence Medical®, 120mm spot size, fractional scanning mode, random, 90mJ energy, 0.3s interval, density 50MTZ/cm², X: 20mm Y: 18mm). From the second to the eighth session, the 800mm spot size was also associated (scanning type brush, interval stacking off, energy 80-100mJ frequency 150Hz, X: 10mm Y: 10mm).
The ablative fractional CO2 laser was applied immediately after the Acroma Q-switched Nd:YAG 1064nm laser. The interval time between sessions was approximately two months, and the treatment started in November 2018.
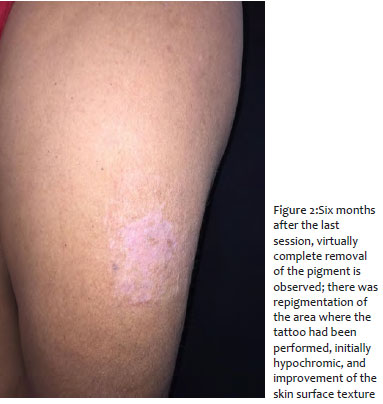
Six months after the last session, we observed practically complete pigment removal (Figure 2). Also, there was repigmentation of the area where the tattoo was performed, initially hypochromic, improvement of the skin surface texture, and thinning of the scars’ thickness. The patient is satisfied with the results achieved.
So far, Q-switched lasers are the primary method available for tattoo removal, as they allow you to target the tattoo pigment and selectively remove it without damaging the surrounding tissue.3,4 The theory of selective photothermolysis, introduced by Anderson and Parrich in 1983, suggests that the interaction between skin and target chromophore allows selective destruction, even through heat, without destruction of adjacent tissues.5 However, for selective photothermolysis to occur, in addition to the appropriate wavelength, the pulse duration time must be shorter than the thermal relaxation time of the target structure.6 Thermal relaxation time (TRT) is the time required for the target structure to lose half the temperature rise at which it was heated by the laser, this time being variable for each chromophore.6 If the laser pulse duration exceeds the thermal relaxation time, damage to adjacent tissues will occur, evolving with burns and scarring.6 The average size of the tattoo pigment is 0.1µm, and the thermal relaxation time is 10ns, so the choice for Q-switched lasers, whose pulse duration is around nanoseconds.6 Depending on the color of the tattoo pigment, different wavelengths are indicated. For black tattoos, the length of 1064nm is the most suitable. Also, it allows greater penetration into the dermis, presenting the least risk of hypochromia and epidermal damage.3
The mode of operation of Q-switched lasers in the treatment of tattoos is through the photoacoustic phenomenon; when reaching the target (pigment contained in tattoos), the laser causes shock waves that make the target vibrate and “explode”, thus occurring the destruction of the pigment.7 The destroyed or altered pigment is then removed by phagocytosis by macrophages.6
The association with fractional ablative lasers is an option for treating tattoos, especially in those with a large amount of pigment, as in the case described, or in tattoos with many colors that are generally difficult to remove, as described in the article by Vanarase and collaborators.8 The study compared the isolated use of Q-switched laser with the use associated with CO2 laser in the ultra-pulsed mode to remove black tattoos. As a result, there was superiority in tattoo removal in the group that associated the two lasers, without increasing the rate of adverse events.8 Also, the association between lasers results in fewer sessions.8
The association between ablative and Q-switched fractional lasers in tattoo removal is an option to be considered in selected cases, given the difficulty in completely removing some of them. Professionals can still use the association only in the final sessions, when the pigment is already sparse, as there is the additional effect of assisting in the tattoo’s healing.
Célia Luiza Petersen Vitello Kalil | 0000-0002-1294-547x Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Clarissa Prieto Herman Reinehr | 0000-0003-1811-4519 Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
1. Klügl I, Hiller K-A, Landthaler M, Bäumler W. Incidence of health problems associated with tattooed skin: a nation-wide survey in German-speaking countries. Dermatology. 2010;221(1):43-50.
2. Kilmer SL, Anderson RR. Clinical use of the Q-switched ruby and the Q-switched Nd:YAG (1064 nm and 532 nm) lasers for treatment of tattoos. J Dermatol Surg Oncol. 1993;19(4):330-8.
3. Henley JK, Ramsey ML. Laser tattoo removal. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020. Available from: http://www.ncbi.nlm.nih.gov/books/NBK442007/
4. Serup J, Bäumler W. Guide to treatment of tattoo complications and tattoo removal. Curr Probl Dermatol. 2017;52:132-8.
5. Anderson RR, Parrish JA. Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science 1983;220(4596):524-7.
6. Brazzini B, Hautmann G, Ghersetich I, Hercogova J, Lotti T. Laser tissue interaction in epidermal pigmented lesions. J Eur Acad Dermatol Venereol 2001;15(5):388-91.
7. Bäumler W. Laser Treatment of tattoos: basic principles. Curr Probl Dermatol. 2017;52:94-104.
8. Vanarase M, Gautam RK, Arora P, Bajaj S, Meena N, Khurana A. Comparison of Q-switched Nd:YAG laser alone versus its combination with ultrapulse CO2 laser for the treatment of black tattoo. J Cosmet Laser Ther 2017;19(5):259-65.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}