


Karina Bittencourt Medeiros1; Deborah Skusa de Torre1; Juliana Merheb Jordão1; Ana Carolina Petes Nogueira2; Thaís Thumé3
Received on: 05/05/2020
Approved on: 15/11/2020
Financial support: None
Conflict of interest: None
Acknowledgement: We thank the patients who trust our treatment and the residents who strive for better patient care and to learn more and more
Study conducted at the Faculdade Evangélica Mackenzie do Paraná, Curitiba (PR), Brazil
Necrobiosis Lipoidica (NL) is a granulomatous dermatosis, mainly affecting people with diabetes due to collagen degeneration. Although there are different treatments, all have little response. Among the options, the Intense Pulsed Light (IPL) and the Laser Erbium-YAG enhance the production and remodeling of the collagen treating the atrophy, besides reducing the erythema by the coagulation of blood vessels. We report a case of a 24-year-old woman with type I Diabetes Mellitus who underwent NL treatment on her left forearm in seven sessions with the association of IPL and 2940 nm Erbium-YAG laser. We observed improvement in central atrophy and erythema.
Keywords: Necrobiosis lipoidica; Diabetes mellitus; Lasers; Laser therapy; Intense pulsed light therapy; Collagen
Necrobiosis Lipoidica (NL) is a relatively rare chronic granulomatous disease that affects more adults, women, and diabetic patients.1,2 It may occur associated with autoimmune thyroiditis, obesity, dyslipidemia, systemic arterial hypertension, rheumatoid arthritis, sarcoidosis, and inflammatory bowel disease.2 Its etiology is unknown and may be the result of hypoxia due to microangiopathy and abnormal glucose metabolism by fibroblasts, resulting in collagen degeneration.1, 2
Clinically, it manifests as a circumscribed oval plaque, with an erythematous raised border and an atrophic center with telangiectasia on the surface. It is typically located in the pre-tibial region,1,3 but can also be found on the face, trunk, and extremities.3 There is a possibility of ulceration related to overweight, hypertension, or trauma. 1,2,3
Histopathological examination shows collagen disorganization and degeneration, with T cells’ inflammatory infiltration in the dermis and hypodermis.3
NL therapy usually consists of topical, intralesional, or oral corticosteroids. But there are several other therapeutic options such as topical retinoid and calcineurin inhibitor, PUVA, fumaric acid esters, antimalarials, anti-TNF-alpha, cyclosporine,1,2 pentoxifylline, intravenous immunoglobulin, skin graft, acetylsalicylic acid, dipyridamole, hyperbaric oxygen therapy, nicotinamide, benzoyl peroxide, photodynamic therapy, thalidomide, bovine collagen, clofazimine,1 and mycophenolate mofetil.3
Intense pulsed light (IPL) treatment is based on its ability to increase collagen production (types I and III), reorganize it, and coagulate the blood vessel,3 improving the lesion’s texture, and erythema. The treatment with fractional ablative lasers, which use water as their absorbing chromophore, would have a more selective action, with remodeling and increased collagen fibers production (types I and III) reducing the atrophy.
Although treatments with different types of laser and IPL appear to be promising in approaching NL, the pulsed dye laser (PDL) has case reports with conflicting results.4 A study reports a case of NL successfully treated with IPL after 13 sessions.3 The literature does not describe the treatment with Erbium-YAG 2940nm laser.
This paper reports a case of NL treated with IPL and Erbium-YAG 2940nm laser in a patient with long-term diabetes mellitus.
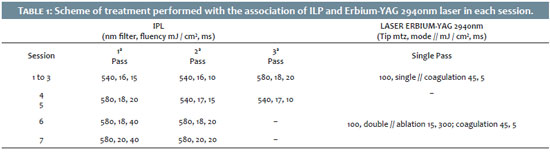
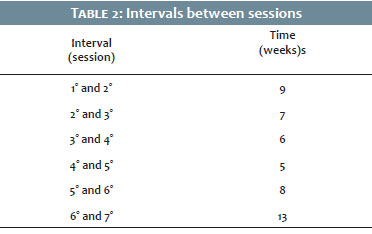
A 24-year-old woman with type I diabetes mellitus presented an oval, atrophic, yellowish plaque, with raised edges, telangiectasia, and slight flaking for two years. The lesion had 4.5 cm in diameter on the left forearm (Figure 1). The patient used injectable insulin glargine and aspart. After a clinical diagnosis of Necrobiosis Lipoidica (NL), she started the treatment with clobetasol propionate cream daily on the lesions’ edges. After 45 days of unsuccessful treatment, we proposed a combined treatment of IPL and Erbium-YAG 2940nm laser (Etherea® Platform).Table 1 shows the parameters used, and Table 2 describes the intervals between sessions.
The distal half was treated with IPL, and the proximal half with IPL and Erbium-YAG 2940nm laser in the first three sessions. Subsequently, the same treatment was instituted throughout the lesion.
The improvement in erythema was progressive, already noticed after the first session. After observing that there was no significant clinical difference between the portions of the lesion in the fourth session, we chose to conduct only IPL. The entire lesion was treated with IPL associated with Erbium-YAG 2940nm laser from the fifth session onwards. There was an improvement in central atrophy, less visible vessels, decreased thickness and erythema of the border (Figure 2), in addition to no further progression of the lesion. The patient is undergoing clinical follow-up.
NL remains a poorly understood disease, and conclusions about treatment have weak scientific evidence. Most cases use high-potency topical corticosteroids, and our patient received them in monotherapy at diagnosis and as adjunctive therapy in the fourth and fifth sessions. Nonetheless, it can aggravate atrophy and telangiectasia.
In addition to traditional treatments, IPL and different types of laser can be used, aiming to decrease inflammatory activity and improve atrophy and telangiectasia.
Two cases already used the pulsed dye laser to treat NL, without success in a few sessions,1,4 but with a good response regarding the reduction of symptoms and the lesion’s size in six sessions.4 It indicates that in NL, the treatment can be more prolonged, with more sessions, to obtain better results.
The fractional ablative Erbium-YAG 2940nm laser stimulates the production of organized type I, III and VII collagen, and elastin, with increased tropoelastin.5 These changes would be responsible for the improvement in skin texture, in addition to the reorganization of collagen. These facts may be responsible for the improvement of the patient’s atrophy. There are no cases described with this type of treatment.
It is believed that IPL promotes a reduction in telangiectasia through its action on hemoglobin, anti-inflammatory and antiproliferative activity,6 acting in the production and organization of collagen fibers.3
The association of IPL and Erbium-YAG 2940nm laser allows clinical improvement with fewer sessions compared to the use of IPL alone. The production and reorganization of collagen improve the atrophy, moving the vessels away from the dermis in relation to the epidermis. In contrast, tropoelastin enhances the elasticity of the skin (which was aimed at using the combined technologies). IPL also acts by coagulating more superficial vessels, thus reducing erythema. We described an unprecedented case of NL treatment with associated use of IPL and Erbium-YAG 2940nm laser, with a moderate response after seven sessions, which remained six months after the end of the treatment.
Karina Bittencourt Medeiros | 0000-0001-8202-6711 Preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Ana Carolina Petes Nogueira | 0000-0001-5766-3815 Preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Thaís Thumé3 | 0000-0002-3282-0527 Preparation and writing of the manuscript; critical literature review.
Deborah Skusa de Torre | 0000-0002-4586-0237 Study design and planning.
Juliana Merheb Jordão | 0000-0002-8403-2784 Approval of the final version of the manuscript; study design and planning; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Feily A, Mehraban S. Treatment modalities of necrobiosis lipoidica: a concise systematic review. Dermatol Reports. 2015;7(2):5749.
2. Erfurt-Berge C, Dissemond J, Schwede K, Seitz AT, Al Ghazal P, Wollina U, et al. Updated results of 100 patients on clinical features and therapeutic options in necrobiosis lipoidica in a retrospective multicentre study. Eur J Dermatol. 2015;25(6):595-601.
3. Cunha MG, Rezende FC, Cunha ALG, Machado Filho CDA. Necrobiosis lipoidica treated with intense pulsed light. J Surg Dermatol 2016;2(1):39-42.
4. Bergqvist E, Bergqvist G. The long-term effect of pulsed dye laser on necrobiosis lipoidica: a case study. J Cosmet Laser Ther. 2019;21(1):17-8.
5. El-Domyati M, Abd-El-Raheem T, Abdel-Wahab H, Medhat W, Hosam W, El-Fakahany H, et al. Fractional versus ablative erbium:yttrium-aluminum-garnet laser resurfacing for facial rejuvenation: an objective evaluation. J Am Acad Dermatol. 2013;68(1):103-12
6. Kalil CLPV, Reinehr CPH, Milman LdM. Luz intensa pulsada: revisão das indicações clínicas. Surg Cosmet Dermatol 2017;9(1):9-17.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}