


Renan Rangel Bonamigo; Laura Luzzatto; Sindy Natália Balconi; Isadora da Luz Silva; Ana Cláudia Dal Magro
Received on: 24/03/2020
Approved on: 13/11/2020
Financial support: None
Conflict of interest: None
Study conducted on Santa Casa de Misericórdia de Porto Alegre, Porto Alegre (RS), Brazil
Squamous cell carcinoma (SCC) represents the second most common type of skin cancer. SCC originates from the atypical proliferation of the cells of the epidermis's spinous layer and is more frequent in men over 50 years of age, with a low skin phototype and history of sun exposure. We describe the case of a 61-year-old man, previously healthy, with a lesion presenting fast and exuberant growth on the face. The anatomopathological and immunohistochemical exams confirmed the diagnosis of moderately differentiated SCC.
Keywords: Carcinoma, Squamous Cell; Neoplasms, Squamous Cell; Skin Neoplasms
Non-melanoma skin cancer is the most common type of cancer in the world and Brazil. Squamous cell carcinoma (SCC) is the second most frequent subtype. While most patients present a good prognosis, some cases may have worse outcomes.1 Recent epidemiological data have shown an increase in its incidence worldwide, which impacts public health.2 Thus, early diagnosis and treatment are essential. We present an unusual case of moderately differentiated SCC, with a fast and exuberantly aggressive local evolution in a patient without evidence of immunosuppression.
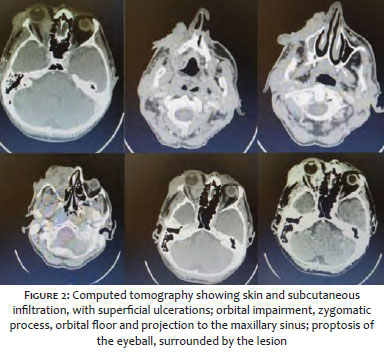
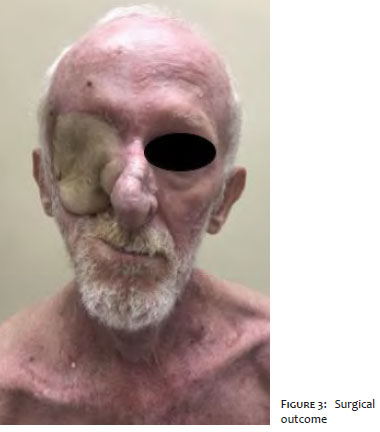
A 61-year-old man, retired farmer, presented an erythematous papule infiltrated with a central crust in the right malar region. He was monitored for multiple previous non-melanocytic skin neoplasms and had no evidence of immunosuppression or other comorbidities. The patient was referred for biopsy under the diagnostic hypothesis of keratoacanthoma or SCC. Histopathology showed actinic damage and sebaceous hyperplasia, not presenting neoplastic cells. The patient returned after three months for follow-up, showing exacerbated growth of the lesion, exulcerated tumor, local pain, and loss of ipsilateral vision (Figure 1). The new histopathological exam evidenced moderately differentiated squamous cell carcinoma (Figure 2). Computed tomography (CT) of the face showed a large expansive, infiltrative lesion, with regional involvement of the skin and subcutaneous tissue, superficial irregularities and ulcerations, orbit’s impairment, zygomatic process, orbital floor, and projection to the maxillary sinus. There was also evidence of proptosis of the eyeball, surrounded by the lesion. We observed no swollen lymph node enlargement in the cervical region. The patient was staged as T4aN0M0 and urgently referred to the institution’s Head and Neck Surgery Service and briefly submitted to a surgical procedure. We performed an orbital exenteration with total maxillectomy and partial parotidectomy, with reconstruction using a microsurgical flap of the rectus abdominis muscle, with good postoperative evolution (Figure 3) and anatomopathological exam indicating lesion-free margins.
SCC originates from the atypical proliferation of cells in the spinous layer of the epidermis. It may present clinically as a papule, nodule, or plaque lesion and may also present associated hyperkeratosis and ulceration. Professionals should consider actinic keratoses, basal cell carcinomas, attachment tumors, amelanotic melanomas, and keratoacanthoma as differential diagnosis, as in our case.2 Well-differentiated SCC can be clinically and histopathologically similar to keratoacanthoma, and, therefore, it is crucial to rule out this possibility in contexts of rapid tumor growth. In the present case, histopathology and invasiveness of deep structures confirmed that it was SCC.
Epidemiologically, SCC occurs predominantly in men over 50 years old, with a low skin phototype and sun exposure history. It is the most frequent tumor in transplanted individuals, being two to three times more common than basal cell carcinoma. The natural history of squamous cell carcinomas varies from slow to fast, with accelerated growth being observed more frequently in immunosuppressed patients. In the context of immunosuppression, SCC is often multiple and tends to be more aggressive.6
Among the most common causes of systemic immunosuppression, in addition to organ transplants (58%), there are systemic inflammatory diseases (16%).4 In kidney transplant patients, treatment with immunosuppressants combined with ultraviolet radiation causes a deficiency in the systemic and local immune response. These patients have a numerical decrease in lymphocyte subtypes (CD4 and CD8), lymphocytes that express the interleukin-2 receptor on the skin, and Langerhans cells. Thus, there is less expression of MHC-II, compromising local immunological competence, and favoring the appearance of pre-neoplastic and neoplastic lesions.5
As in other types of malignant neoplasms, local leukocyte populations are protective against cancer development and also play a role in the “sculpture” of the high-intensity tumor, leading to many causes of immunogenicity and tumor progression. UV radiation and chronic viral transport may represent unique risk factors for SCC development, and the local immune system plays a key role in modulating the response to both.6
The staging of squamous cell carcinomas considers the tumor volume measured by diameter and depth. It also considers lymph node metastases and distant metastases. High-risk characteristics for metastatic SCC include impairment greater than 2 mm in thickness, Clark’s level greater than or equal to IV, perineural invasion, anatomical location (ear, lips, and mucous membranes are at higher risk), origin in scarring, immunosuppression, and differentiation degree (worse prognosis is associated with poorly differentiated and undifferentiated).2 Our case presents a patient with negative staging for lympho-hematogenous dissemination, but with extreme local aggressiveness, ultimately affecting one of the ocular devices.
The first-line therapy for SCC is complete surgical excision with histopathological control of the margins.3 The literature recommends margins of 4 mm to 10 mm, depending on the clinical characteristics suggestive of high risk of recurrence or not – although there is no consensus. In low-risk tumors, professionals may choose curettage with electrocoagulation and cryosurgery. Adjuvant radiotherapy is recommended in patients with negative margins after surgery in case of perineural involvement, and few drugs have been used successfully in adjuvant or neoadjuvant therapy for metastatic SCC.3
This case presented an uncommon rapid growth, aggressiveness, and tumor volume of the moderately differentiated SCC, mainly due to the absence of a factor that compromises his systemic immune status, highlighting the potential local immunomodulation by UVR.
Surgical management proved to be complicated and followed the principle of Oncodermatology therapy, with the neoplasia’s wide excision.
Renan Rangel Bonamigo | 0000-0003-4792-8466 Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Laura Luzzatto 0000-0002-4193-6943 Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Sindy Natália Balconi | 0000-0002-6369-5474 Study design and planning; preparation and writing of the manuscript; critical literature review.
Isadora da Luz Silva | 0000-0001-9084-8723 Study design and planning; preparation and writing of the manuscript; critical literature review.
Ana Cláudia Dal Magro | 0000-0001-5472-4539 Study design and planning; preparation and writing of the manuscript; critical literature review.
1. Kabir S, Schmults CD, Ruiz ES. A review of cutaneous squamous cell carcinoma epidemiology, diagnosis and management. Int J Cancer Manag. 2018;11(1):e60846.
2. Bolognia JL, Jorizzo JL, Schaffer JV. Dermatologia. 3th ed. Rio de Janeiro: Elsevier; 2015. p. 2816-2820.
3. NCCN Guidelines for patients. Squamous cell skin cancer. 2020. Available from: https://www.nccn.org/patients/guidelines/content/PDF/squamous_cell-patient.pdf
4. Gonzalez JL, Reddy ND, Cunningham K, Silverman R, Madan E, Nguyen BM. Multiple cutaneous squamous cell carcinoma in immunosuppressed vs immunocompetent patients. JAMA Dermatol. 2019;155(5):625-
5. Almeida APN, Almeida LM, Franco KP, Peçanha MAP. Lesões cutâneas malignas e pré-malignas pós transplante renal: Case report e revisão da literatura. Rev Cient FMC. 2014;9(1):30-4.
6. Bottomley MJ, Thomson J, Harwood C, Leigh I. The role of the immune system in cutaneous squamous cell carcinoma. Int J Mol Sci. 2019;20(8):2009.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}