


Rebecca Silveira; Tatiane Benini; André Cesar Antiori Freire Pessanha
Received on: 31/01/2020
Approved on: 13/11/2020
Financial support: None
Conflict of interest: None
Study conducted at the Universidade de Mogi das Cruzes, Mogi das Cruzes (SP), Brazil
Undifferentiated sarcomas are neoplasms of soft tissues derived from the mesoderm. We report a case of undifferentiated pleomorphic sarcoma, its dermoscopy, staging, and therapeutic approach.
Keywords: Dermoscopy; Sarcoma; Soft Tissue Neoplasms
Sarcomas are tumors derived from the mesoderm. They are divided into two types: bone and soft tissue sarcomas, which include skin tumors.1 Soft tissue sarcomas affect one to five individuals/ 100,000/ year, mainly over 55 years old.2 Its main subtypes are gastrointestinal, liposarcoma, and leiomyosarcoma.2 There are two types of soft tissue sarcomas that most commonly appear on the skin: undifferentiated pleomorphic sarcoma (previously called storiform-pleomorphic malignant fibrous histiocytoma) and myxofibrosarcoma (formerly called myxoid malignant fibrohistiocytoma).1 Cutaneous sarcomas usually present as skin-colored nodules or subcutaneous masses, with rapid growth, most commonly in the limbs.1
There is a histological grade (G) for soft tissue sarcomas (FNCLCC-France) in which three parameters receive a score: differentiation (1 to 3), mitotic index (1 to 3), and tumor necrosis (0 to 2). The sum of the numbers results in GX, G1 (2 to 3), G2 (4 to 5), and G3 (6 to 8). The American Cancer Society (ACS) has also established a TNM staging for this group of tumors depending on their topography: head and neck, trunk and extremities, thoracic and abdominal visceral organs, and retroperitoneum.3
Undifferentiated pleomorphic sarcoma (UPS) is the fourth most important soft tissue sarcoma. Regarding its epidemiology, it affects mostly men (two thirds) in relation to women, in the age group of 50 to 70 years (most affected age group).4 It is more frequent in the lower limbs, but 10% to 15% occur in the head and neck.1 Regarding its evolutionary trend, it presents a local recurrence of 19% to 31%, and a metastasis index of 31% to 35% (with a frequency of 90% in the lungs, 85% in the bones, and 1% in the liver). Its five-year survival rate is 65% to 70%. The recommended treatment is surgical with 2 cm margins and adjuvant radiotherapy in selected cases (however, it is difficult to obtain free margins through surgery). For metastatic disease, chemotherapy is indicated (albeit with poor results) with anthracyclines (16% to 27% response) associated or not with ifosfamide. Doxorubicin is palliative. New studies have shown greater benefit with eribulin mesylate.5
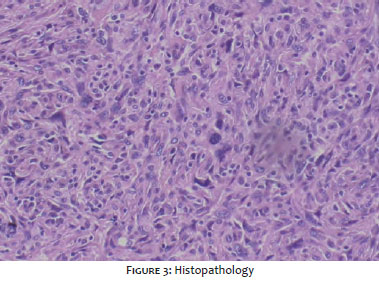
An 88-year-old woman presented a nodular lesion with progressive growth in the left clavicle region for three months. Dermatological examination showed a violet, ulcerated tumor, with friable necrosis, 11 cm in the longest axis, in the left infraclavicular area (Figure 1). Polymorphic vessels characterized the dermoscopy without other specificities (Figure 2). We performed the lesion’s incisional biopsy, whose anatomopathological examination revealed infiltration of the deep portion of the sample by large cell neoplasia, with a predominant fusiform shape, with cell nuclei of varying sizes and shapes, with irregular chromatin. Numerous mitosis figures, compatible with fusocellular and pleomorphic sarcoma, infiltrated the reticular dermis, histological grade 3 (Figure 3). The immunohistochemical panel showed a negative result for the expression of all the antigens surveyed (AE1/AE3, p63, 34BetaE12, protein S-100, SOX-100, melan-A, AML, desmin, CD3, and CD34), compatible with undifferentiated sarcoma. After anatomopathological examination, we opted for excision of the lesion with wide surgical margins and closure by primary intent of the surgical wound (Figure 4). We performed screening for lung, lymph node, and abdominal metastases with imaging tests, which was negative. The patient is being followed up, with no signs of local recurrence (Figure 5).
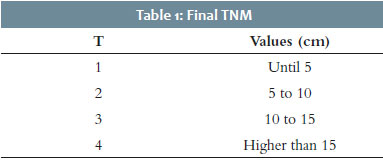
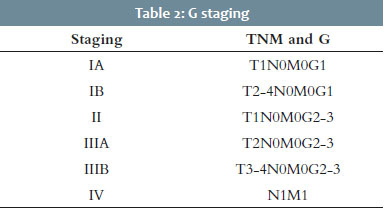
For TNM staging of this case, we adopted the American Joint Committee on Cancer (AJCC) 2018 reference for the trunk and extremities’ soft tissue sarcomas. Table 1 represents the T, and Table 2 shows the final staging (note that the G classification described in the introduction is considered). In both tables, the case reported is highlighted.
In the reported case, immunohistochemistry was essential since clinically, and even histopathologically undifferentiated pleomorphic sarcoma makes a differential diagnosis with:
- Melanoma (desmoplastic; frequent positivity for S100, HMW-MMA; rare positivity for SMA, desmin, factor XIIIA, laminin, and type IV collagen; and generally negative for HMB-45, Gp100, melan A/Mart1, tyrosinase, and transcription factor of microphthalmia).6
- Spindle cell squamous cell carcinoma (positive for AE1/AE3, vimentin, and CAM5.2, and vimentin).7
- Dermatofibrosarcoma protuberans (positivity for CD34 and vimentin; negativity for neuron-specific enolase, HMB-45, and S100 protein).8
- Atypical fibroxanthoma (exclusion diagnosis, negative for cytokeratins to exclude spindle cell carcinoma, spindle cells, S-100, and melanogenic markers such as melan-A and HMB-45 to exclude melanoma; desmin, actin, and H-caldesmon to exclude leiomyosarcoma; and p63 and p40 to exclude squamous cell carcinoma.9
- Leiomyosarcoma (positivity for smooth muscle actin, desmin, and S100).10
- Undifferentiated pleomorphic sarcoma (positive for vimentin, factor XIIIa, CD68, CD10, CD34, CD 99; and negative for keratin, muscle, and melanocytic markers).11
The case presented enriches the dermatologist’s memory regarding the possible differential diagnoses among the rare mesenchymal tumors. We emphasized how essential the role of histopathology and immunohistochemistry is, reviewing the game of markers with their diagnostic correlations in this mini-challenge and bringing the opportunity to review the staging and the conduct of soft tissue sarcomas.
Rebecca Silveira | 0000-0001-7164-4717 Critical literature review.
Tatiane Benini | 0000-0002-4084-7607 Preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
André Cesar Antiori Freire Pessanha | 0000-0001-9806-4245 Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Paiva A.C.G., Morgado A.M., Souza M.P. Undifferentiated pleomorphic sarcoma. An Bras Dermatol. 2018;93(1):154-5.
2. Staser K, Mount J, Solus C , Musiec A; Pleomorphic soft tissue sarcoma metastatic to the skin of the scalp and groin; JAAD case reports, march 2015.
3. Site da American Cancer Society : https://www.cancer.org/cancer/soft-tissue-sarcoma/detection-diagnosis-staging/staging.html
4. Salerni G ; Dermoscopic findings in an early malignant fibrous histiocytoma on the face ; Dermatology Practical and Conceptual; 2017; 7(3) : 9
5. De Vita A. ,Recine F., Mercatali L. , Miserocchi G., Spadazzi C., Liverani C. , Bongiovanni A. , Pieri F. , Casadei R. , Nada Riva N. , Fausti V , Amadori D, Ibrahim T; Primary Culture of Undifferentiated Pleomorphic Sarcoma: Molecular Characterization and Response to Anticancer AgentsInt. J. Mol. Sci. 2017, 18, 2662; doi:10.3390/ijms18122662
6. Paschoal FM, Yamada VL, Enokihara MMSS, Machado Filho CDS; Melanoma desmoplástico ;Surg Cosmet Dermatol 2012;4(1):59-63.
7. Mitsuhashi et al.; Basosquamous and spindle cell carcinoma of the skin; J Cutan Pathol 2006: 33: 246-252; Copyright # Blackwell Munksgaard 2006.
8. Morais PM, Schettini APM, Chirano CA, Nakamura G; Tumor de Bednar (dermatofibrossarcoma protuberante pigmentado): relato de um caso, An Bras Dermatol. 2005;80(3):273-6.
9. Koch et al : Atypical Fibroxanthoma - Histological Diagnosis, Immunohistochemical Markers and Concepts of Therapy; Anticancer Research 35: 5717-5736 (2015).
10. Salgado LMR, Caetano LVN, Paula GM, Cysneiros MAPC, Fleury Jr LFF ;Leiomiossarcoma cutâneo: Case report; Surg Cosmet Dermatol 2015;7(1):84-7.
11. Site de anatomia patológica da University of Washington : http://www.pathologyoutlines.com/topic/softtissuemfhpleo.html
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}