


André Ricardo Adriano1; Juliano Borges1; Jordano Luiz da Costa2
Received on: 07/01/2020
Approved on: 03/11/2020
Financial support: None
Conflict of interest: None
Acknowledgement: We thank Professor Azulay for the encouragement to study, publish, and share knowledge
Study conducted at the Dermatology Institute Professor Rubem David Azulay, Santa Casa da Misericórdia do Rio de Janeiro, Rio de Janeiro (RJ), Brazil
The cuniculatum carcinoma is a rare, slow-growth, local aggressive subtype of the squamous cell carcinoma, presented as a verrucous lesion with a low metastasis capacity. Its histopathology shows keratin-filled crypts, and its etiology is linked with HPV, especially 11 and 16 subtypes. The treatment of choice is surgical excision, followed by regular monitoring due to the high risk of local recurrence. We report a case of a woman with Cuniculatum carcinoma treated with surgery with perioperative frozen section procedure, graft, and good evolution.
Keywords: Carcinoma; Carcinoma, Squamous Cell; Foot
Squamous cell carcinoma is the second most common type of skin cancer, behind only basal cell carcinoma.1 Carcinoma cuniculatum (CC) is a verrucous carcinoma (VC), a rare and indolent form of squamous cell carcinoma (SCC), well differentiated. Slow growth, local aggressiveness, and low capacity to cause metastasis characterize it. It penetrates the deep tissues, forming crypts filled with keratin.2,3
It was first described in 1954 by Aird et al.1, 5 It is more common in men than in women (5:1). Its pathogenesis has not been completely elucidated, but the association with human papillomavirus (HPV), especially subtypes 11 and 16, has been described.5,6
The treatment of choice is surgical excision with margin control, and the patient must be regularly monitored for the risk of recurrences, even when the surgical margins are free.6
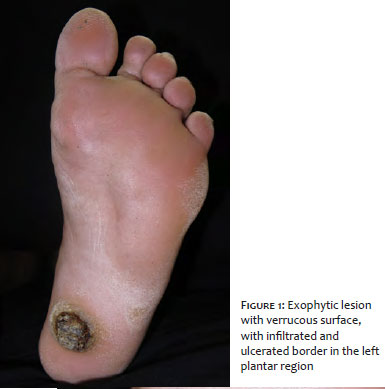
A 64-year-old woman, working as a sales clerk, sought medical care due to a lesion in the left plantar region two years ago, with a foul odor and associated local pain. The physical examination observed an exophytic lesion with a verrucous surface, 5 cm in diameter, with an infiltrated and ulcerated border (Figures 1 and 2). The image examination, X-ray of the left foot, showed a nodular image with a radiotransparent halo in soft tissues in the plantar region, without bone involvement (Figure 3).
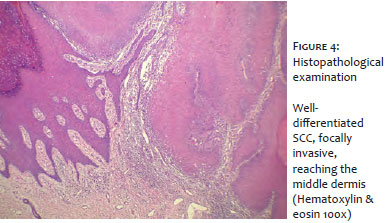
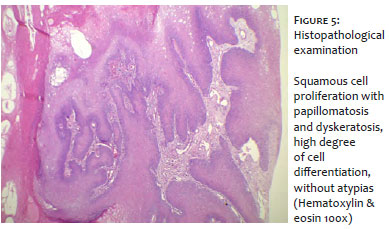
A biopsy was performed based on the suggested hypotheses of VC, keratoacanthoma, common wart, and amelanotic melanoma. The result favored the diagnosis of VC. Excisional surgery was then scheduled with histopathological evaluation by perioperative frozen section. The report indicated a well-differentiated SCC, focally invasive, reaching the middle dermis, with no perineural infiltration or angiolymphatic invasion, and free surgical margins (Figures 4 and 5).
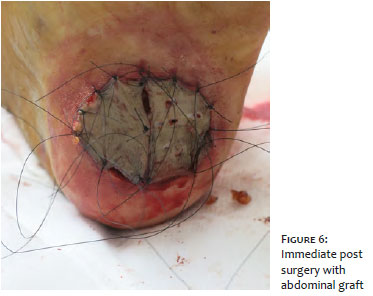
After the lesion’s complete excision, skin grafting was obtained from the abdominopelvic fold (Figura 6), and a fragment was sent for HPV research, with a positive result for type 16.
The patient evolved with good graft healing and subsequent return to daily activities. After 1.5 years of follow-up, we observed no lesion recurrence.
CC is a VC, a rare and indolent form of SCC. It usually has characteristics of a benign, verrucous tumor, with slow growth, more expansive than invasive evolutionary pattern, good cell differentiation, and low tendency to metastasis.2,7
Although its most common site is in the plantar region, it can occur in several other areas, such as the flank, legs, face, oral cavity, genital, and palmar region.4 It is called CC when it is located in the plantar area; Buschke-Lowenstein tumor, in the anogenital region; and Ackerman’s tumor, when in the oral region.3,8
It was first described in 1954 by Aird et al.1, 5 It is more common in men than in women (5:1)5 – what makes the report of this case even rarer because it is a female patient. Its pathogenesis is unknown, but the association with human papillomavirus (HPV), especially subtypes 11 and 16, has been described,6 as identified in the case above.
Diagnosis is based on dermatological and histopathological examination.5,6 This carcinoma should be suspected when the patient has a recurrent lesion on usual therapy. The differential diagnosis is made with common wart and keratoacanthoma.6,9
We observed scaly proliferation with papillomatosis and dyskeratosis in histopathology, a high degree of cell differentiation, without atypia. Keratin pseudocysts can be formed, sometimes with pus, generating a foul odor.3
The treatment of choice is surgical excision with margin control, and the patient must be regularly monitored for the risk of recurrences, even when free margins are obtained.6,7 In the case reported, we opted for surgery with a perioperative frozen section to control the margins and perform a graft on the patient’s abdomen, with Brown dressing. The patient has been in follow-up for more than two years without recurrence so far.
André Ricardo Adriano | 0000-0002-2986-959X Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Jordano Luiz da Costa | 0000-0003-1635-6944 Preparation and writing of the manuscript.
Juliano Borges | 0000-0001-8291-0806 Critical literature review; critical revision of the manuscript.
1. Feldmann R, Wruhs M, Peinhaupt T, Stella A, Breier F. Carcinoma cuniculatum of the right thenar region with bone involvement and lymph node metastases. Case Rep Dermatol. 2017;9:225-30.
2. Arisi M, Zane C, Edu I, Battocchio S, Petrilli G. Carcinoma cuniculatum of the foot invading the bone mimicking a pseudo-epitheliomatous reaction to an acute osteomyelitis. Dermatol Ther. 2016;6(1):95-9.
3. McArdle DJT, McArdle JP, Lee F, Mignanelli ED. Rare "inverted" verrucous carcinoma (Carcinoma Cuniculatum) of the sacrogluteal region: case report and literature review. International Journal Of Surgical Pathology 2017;25(5):438-42.
4. Kotwal M, Poflee S, Bobhate S. Carcinoma cuniculatum at various anatomical sites. Ind J Dermatol. 2005;50(4):216-220.
5. Chavez-Bolanos LJ, Días-Gómez CJ. Epitelioma cuniculatum plantar. Dermatol Peru. 2014;24(2):103-5.
6. McKay C, McBride P, Muir J. Plantar verrucous carcinoma masquerading as toe web intertigo. Australas J Dermatol. 2012;53(2):e20-2.
7. Zanini, M. Carcinoma Verrucoso. Med Cutan Iber Lat Am. 2011;39(1):26-9.
8. Kubik MJ, Rhatigan, RM. Carcinoma cuniculatum: not a verrucous carcinoma. J Cutan Pathol. 2012;39(12):1083-7.
9. Barreto, JE, Velazquez EP, Ayala E, Torres J, Cubilla AL. Carcinoma cuniculatum: a distinctive variant of penile squamous cell carcinoma: report of 7 cases. Am J Surg Pathol. 2007;31:71-5.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}