


Thiago da Silveira Manzione1; Sidney Roberto Nadal2; John Verrinder Veasey3
Received on: 29/10/2019
Approved on: 12/11/2020
Financial support: None
Conflict of interest: None
Study conducted at the Dermatology Clinic of Santa Casa de São Paulo, São Paulo (SP), Brazil
Buschke-Lowenstein tumor (BLT) is an extremely rare variant of condylomata acuminata that presents a benign biological behavior and histological characteristics despite being clinically presented by large lesions. Many therapeutic approaches are available, many of which rely on extensive and mutilating surgical procedures. We present two cases of patients with BLT treated with topical podophyllin whose therapeutic responses were extremely favorable in both cases.
Keywords: Podophyllin; Condylomata Acuminata; Carcinoma, Verrucous; Neoadjuvant Therapy
The Buschke-Lowenstein tumor (BLT), also known as giant condyloma acuminata, is a rare variant of condyloma acuminata, comprising about 0.1% of cases.1 It is caused by human papillomavirus (HPV) types 6 and 11.2 The risk factors described are immunosuppression, pregnancy, alcohol and tobacco consumption, poor local hygiene, and Herpes simplex virus infection.3
Clinically, the lesion reaches massive proportions, with aggressive local characteristics, invading and causing deformity in the adjacent tissues, but without lymphatic, vascular, or neuronal invasion.4 The risk of degeneration for squamous cell carcinoma (SCC) ranges from 30% to 56%. At the same time, condylomata acuminata has a risk of only 2%.5 Histologically, BLT is distinguished from condylomata acuminata by its proliferation and deep penetration into adjacent tissues, and from SCC, by the integrity of the basement membrane and inability to produce metastases.3
BLT has several therapeutic approaches, such as topical medications, cryosurgery, surgical excision, immunotherapy, chemotherapy, radiotherapy, and electrocoagulation. There is no consensus to guide the therapeutic decision, but the initial choice in many services is surgical excision.5
Surgery should be local resection, keeping margins free of residual disease. Surgical removal can cause extensive wounds, cicatricial strictures, and fecal incontinence. Abdominoperineal amputation is indicated when the sphincter apparatus is involved.6 Among the most used topical agents are podophyllin, which has an exfoliating, immunological, and antimitotic action,5,6 and imiquimod, an immunomodulatory substance capable of enhancing the immune response to HPV.5,6
A 25-year-old man with positive serology for HIV for eight months, using antiretroviral therapy (ART) with tenofovir, efavirenz, and lamivudine since his diagnosis, presenting CD4 cell count of 253/µL and undetected viral load.
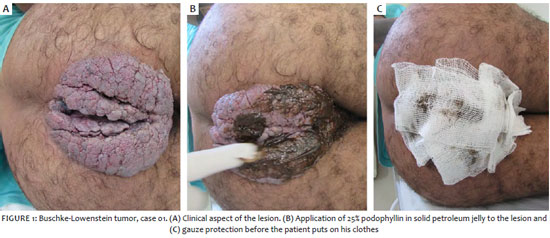
He complained of an anal tumor for nine months, evolving in the last month with an increase in the lesion, associated with a foul odor and difficulty in hygiene. Upon dermatological examination, he presented a large tumor with a verrucous aspect, 30 cm in diameter, occupying the buttocks, perineum, and intergluteal sulcus, making it impossible to identify the anus (figure 1).
The biopsy of the lesion ruled out SCC, which report concluded it was a condyloma acuminata. We prescribed sulfamethoxazole + trimethoprim, due to secondary infection, and topical treatment with podophyllin 25% in solid petroleum jelly started once a week, instructing the patient to remove the medication, washing it after six hours (figure 1).
After 23 applications for six months, we observed almost complete regression of the lesion (figure 2). After that, surgical resection and cauterization of the few remaining lesions were indicated. The histopathological evaluation of the resected piece did not present carcinoma, and the clinical evolution was favorable. The wounds healed after four weeks, with no signs of recurrence.
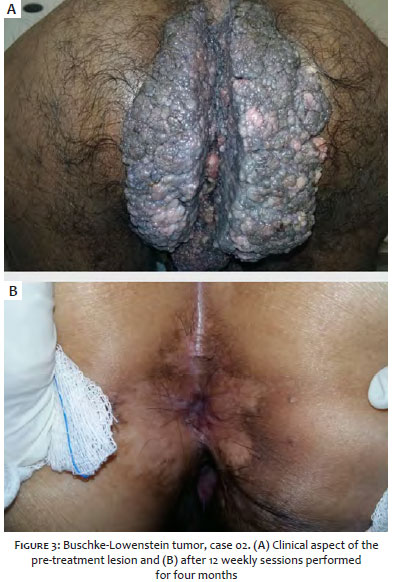
A 42-year-old woman, positive for HIV for six years, complaining of an anal tumor for 12 months. She withdrew ART after six months, with a significant increase in the lesion. The patient had 124/µL CD4 T lymphocytes and a viral load greater than 200,000/mL.
She was instructed to resume ART and started weekly treatment with podophyllin 25% in solid petroleum jelly. After the third application, the lesion showed a significant reduction. She received 12 applications over four months when the disappearance was complete (figure 3). The biopsy performed at the first consultation revealed condyloma acuminata, with no signs of malignancy. Anal colposcopy and cytology of the anal canal were normal at the end of treatment. There was no recurrence.
BLT involving the perianal region is rare. A meta-analysis evaluating publications from 1958 to 2000 found only 51 cases. It is more frequent in men (2.7:1) with an average age of 43.9 years.7
There appears to be a complex interaction between HIV, HPV, and local mucosa’s immunological mechanisms. HIV increases HPV transcription, and it causes a decrease in the number of macrophages, Langerhans cells, and CD4 T lymphocytes in the mucosa, with a consequent reduction in local immune control of HPV infection and increased proliferation of this virus.8
Although resection is the most commonly performed procedure, topical treatment was instituted to reduce the lesions’ size, thus facilitating resection and postoperative discomfort. Podophyllin 25% in solid petroleum jelly was used because it is easy to obtain and has low cost since the authors work in public hospitals and have experience with this medication in anogenital condyloma acuminata, including in children.1,5,6 This procedure causes remission of the lesions, avoids surgeries, and facilitates surgical procedures and postoperative recovery.
The patients are being followed up and periodically reassessed with dermatological and proctological examination. If there is no clinical lesion, cytology and anal colposcopy are performed. This follow-up strategy is necessary for surveillance of malignant lesions and early detection of clinical and subclinical recurrences.7,9
Treatment with topical substances can be instituted for BLT cases, with the possibility of reducing lesions, facilitating operative treatment, and avoiding complications caused by healing.
Thiago da Silveira Manzione | 0000-0003-1914-0129
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Sidney Roberto Nadal | 0000-0002-8238-4559
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
John Verrinder Veasey | 0000-0002-4256-5734
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Akhavizadegan H. Electrocautery resection, shaving with a scalpel, and podophyllin: a combination therapy for giant condyloma acuminatum. World J Mens Health. 2015;33(1):39-41.
2. Braga JC, Nadal SR, Stiepcich M, Framil VM, Muller H. Buschke Loewenstein tumor: identification of HPV type 6 and 11. An Bras Dermatol. 2012;87(1):131-4.
3. Trombetta LJ, Place RJ. Giant condyloma acuminatum of the anorectum: trends in epidemiology and management: report of a case and review of the literature. Dis Colon Rectum. 2001;44:1878-86.
4. Hull MT, Eble JN, Priest JB, Mulcahy JJ. Ultraestructure of Buschke-Lowenstein tumor. J Urol. 1981;126(4):485-9.
5. Nadal SR, Manzione CR. Proctologia na AIDS. 1st ed. São Paulo: Di Livros Editora; 2007.
6. Veasey JV, Dall'Antonia M, Miguel BAF, Mayor SAS, Campaner AB, Manzione TS. Anogenital condylomas in children: descriptive analysis of 20 cases. Surg Cosmet Dermatol. 2017;9(2):127-9.
7. Chu QD, Vezerifis MP, Libbery NP, Wanebo HJ. Giant condyloma acuminatum (Buschke and Lowenstein tumor) of the anorectal and perineal regions. Analysis of 42 cases. Dis Colon Rectum. 1994;37(9):950-7.
8. Mudrikova T. HPV-related anogenital disease and HIV infection: not always "ordinary" condilomata acuminate. Neth J Med. 2008;66:98-102.
9. Liszewski W, Ananth AT, Ploch LE, Rogers NE. Anal Pap smears and anal câncer: what dermatologists should know. J Am Acad Dermatol. 2014;71(5):985-92.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}