


Emanuella Stella Mikilita; Fernando Eibs Cafrune
Received on: 05/09/2019
Approved on: 10/08/2020
Financial support: None
Conflict of interest: None
Study conducted at the Santa Casa de Misericórdia de Porto Alegre, Porto Alegre (RS), Brazil
The trilobate flap can be used for the reconstruction of mid-size defects of the lower nasal portion. The third lobe determines the rotational arch’s increase, reducing the flap tension and improving the final aesthetics. We report the case of a patient submitted to the procedure with good aesthetic and functional results.
Keywords: Dermatologic Surgical Procedures; Mohs Surgery; Surgical Flaps
Nasal reconstruction is always challenging for the dermatological surgeon. Resection of skin neoplasms usually causes losses of nasal substance. There are many alternatives for skin coverage, and skin flaps are the best option. However, the choice of the best technique must be considered individually to achieve the best functional and aesthetic results, with minimal distortion of the anatomy. We report the case of a young patient with a significant nasal defect after tumor resection and rotation of a trilobed flap.
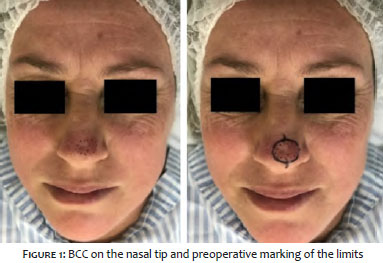
The patient was diagnosed with basal cell carcinoma at the transition from the nasal tip to the nasal dorsum. The incisional biopsy showed a tumor of approximately 1.2 cm (Figure 1). After undergoing tumor resection through Mohs micrographic surgery, the patient presented a defect of approximately 1.6 cm (Figure 2). After intraoperative analysis of the best surgical technique, we chose to perform a transposition flap with a variation of the bilobed flap technique (Figure 2). The immediate postoperative period showed little distortion of the anatomy (Figure 3). Reassessment was performed 90 days after surgery, with excellent aesthetic and functional results (Figure 4).
Partial-thickness nasal defects at the nasal tip present unique reconstructive challenges. The literature cites the bilobed flap and the extended glabellar flap as the first options for these types of defects for nose tip reconstruction.1,2
The dorsal nasal flap is a widely used reconstruction technique that preserves the distal nasal contour as a sliding flap, with rotation and advancement elements, accessing the reservoir of loose nasal skin and dorsal glabellar. The repair occurs using long suture lines, hidden along the nasofacial groove and the glabella, but always with an oblique distal nasal suture line at the standing cone repair site. 2,3
The trilobed flap recently described and detailed by Albertini and Hansen, is an elegant technique to address the nasal tip’s lower nasal defects. This flap further expanded the application of transpositional flaps for nasal repair that were previously repairable only by interpolation or grafts.3
This technique presents as a good option in case of small and medium defects in the distal region of the nose as it allows greater mobility with the use of tissue from the upper nasal portions.
This flap consists of the incorporation of the third lobe into the bilobed flap. The third lobe allows a total rotating arc of 135° to 150° with lobes separated by an external rotating angle of 45° to 50° oriented perpendicularly to the free margin, which determines an increase in the rotational arc, facilitating orientation and decreasing the tension perpendicular to the alar edge.3
The flap is projected around this pivot point, drawing arches and creating lobes of equal or almost equal size. The final flap design, including exact lobe size and length, is altered to a small degree on a case-by-case basis, based on various factors: swelling of the tissues at the time of reconstruction, elasticity, stiffness of the nasal skin, and surrounding scar.4,5
Due to the greater tissue mobility obtained with the multilobed flap, there is no need to extend the skin incisions superior to the glabella. The natural upper incisions (and the true reservoir) are found in the upper lateral wall and the medial nasal skin.4
This flap depends on the upper nasal portion. Therefore, patients with thin nasal skin, previous radiation, or previous nose surgery can benefit from other reconstructive options.3,5
Unsightly results with difficult healing, nasal asymmetry, especially alar, reduced airflow by anchoring in the ipsilateral internal nasal valve3,6 and tip elevation are possible complications. However, they are usually avoided with proper patient selection, flap design, and surgical execution.4
The trilobed flaps create a flap with predictable tissue movements and outcomes and can be used for defects in the nasal tip with excellent functional and aesthetic results. Selection of the type of flap for each defect remains crucial to the success of reconstruction.
Emanuella Stella Mikilita | 0000-0002-7659-4381
Preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
Fernando Eibs Cafrune | 0000-0002-6645-0122
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Laitano FF, Teixeira LF, Siqueira EJ, Alvarez GS, Martins PDE, Oliveira MP. Uso de retalho cutâneo para reconstrução nasal após ressecção neoplásica. Rev. Bras. Cir. Plást. 2012;27(2):217-22.
2. Collar RM, Ward PD, Baker SR. Reconstructive perspectives of cutaneous defects involving the nasal tip: a retrospective review. Arch Facial Plast Surg. 2011;13(2):91-6.
3. Wang CY, Armbrecht ES, Burkemper NM, Glaser DA, Maher IA. Bending the arc of the trilobed flap through external interlobe angle inequality. Dermatol Surg. 2018;44(5):621-9.
4. Albertini JG, Hansen JP. Trilobed flap reconstruction for distal nasal skin defects. Dermatol Surg. 2010;36(11):1726-35.
5. Jellinek NJ e Findley AB. Trilobed flaps: an alternative to dorsal nasal flaps. Glob Dermatol, 2016;3(3):302-4.
6. Hussain W, Mortimer N, Salmon P. Optimizing outcomes in trilobed flap reconstruction for nasal tip defects. Dermatol Surg. 2011;37(4):551.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}