


Juliana Chaves Fabrini1; Michelle dos Santos Diniz1; Mônica Maria de Faria Pimenta1; Maria Silvia Laborne Alves de Sousa2; Ralph Brito Damaceno1; Cassio Ferreira Guimarães2;
Received on: 11/11/2019
Approved on: 25/02/2020
Financial support: None
Conflict of interest: None
Acknowledgment: I thank the dedication of the preceptors Michelle dos Santos Diniz, Maria Silvia Laborne, and Cassio Ferreira Guimarães
Study conducted at the Dermatology Service of Santa Casa de Misericórdia in Belo Horizonte, Belo Horizonte (MG), Brazil
Dermatofibrosarcoma protuberans is a locally aggressive sarcoma of intermediate malignancy that predominates in the range of young adults to middle age. Congenital or childhood lesions are rare but have been reported. It can be misdiagnosed and incompletely excised in the early stages, which increases the risk of recurrence. The present article reports the case of a 24-year-old male patient presenting a hyperchromic macula in the abdominal region from birth that evolved into a tumor after several surgical approaches. Biopsy and immunohistochemistry confirmed the diagnosis of dermatofibrosarcoma protuberans, and the lesion was excised with a 3 cm margin.
Keywords: Dermatofibrosarcoma; Neoplasms, Fibrous Tissue; Sarcoma
Dermatofibrosarcoma protuberans (DFSP) is a fibrohistiocytic tumor of intermediate malignancy, which, although rare, represents the majority of cutaneous sarcomas. It is locally aggressive, with high rates of recurrence but low metastatic potential. DFSP occurs more in the age group of 20 to 50 years and has a slight predominance in males.1,2,6
The most frequent location is the trunk (40-60%), followed by the limbs (20-30%) and the head and neck (10-15%).3 It is exceptionally described on the abdominal wall, as it represents the soft tissue tumor, less frequent in this region.4
In its initial phase, DFSP presents as a hardened plaque, asymptomatic, skin color, violet, reddish-brown, or hyperchromic, similar to keloid. Eventually, DFSP develops reddish-brown nodules up to several centimeters in diameter. In palpation, the lesion is solid and adhered to the subcutaneous tissue. There are reports of lesions that develop after trauma or in previous surgical scar.1,3,7
In histopathological examination, DFSP presents a uniform, dense collection of spindle cells arranged as short fascicles in a “storiform” or mat-like arrangement with low nuclear pleomorphism and low mitotic activity. The cells infiltrate the subcutaneous tissue forming a “honeycomb” pattern. Deep cellular projections toward the fascia and muscle hinder delimitation and surgical removal of the DFSP.3,5,6
The immunohistochemistry test of DFSP shows fusiform cells positive for CD34 and factor XIIIa negative, which helps in the differential diagnosis with dermatofibroma, in which cells are CD34 negative and factor XIIIa positive.2,7,8
Complete surgical excision, including Mohs micrographic surgery, is the standard treatment for DFSP. Imatinib mesylate has been tried in patients with unresectable, recurrent, and/or metastatic DFSP.2
The aim of this study is to highlight the importance of early diagnosis of DFSP, which, although rare, can clinically simulate various cutaneous lesions, such as keloids. The first surgical approach with broad margins has a greater curative chance, reducing risk for local recurrences and high morbidity.
A 24-year-old male patient from Belo Horizonte, Brazil, with lesion in the abdominal epigastric region from birth, which began as a hyperchromic macula accompanied by pain at the site.
A biopsy was performed at 12 years of age, suggestive of keloid according to the patient, who did not present the anatomopathological result at the medical appointment. The patient underwent the surgical approach at 12 and 16 years of age, with posterior recurrence and lesion growth, which progressed to nodules and skin color plaques. He also did not have the histological results of these surgeries.
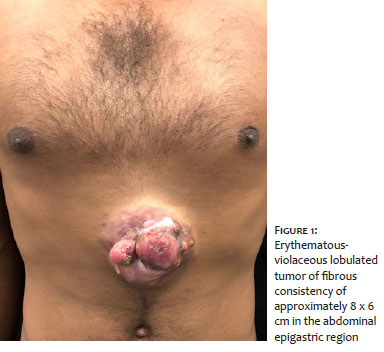
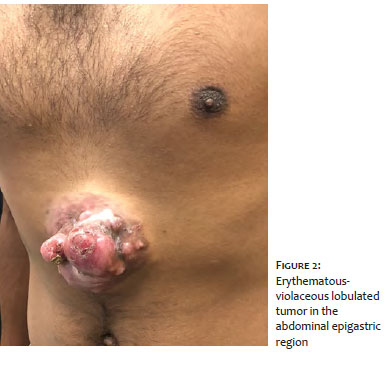
At age 24, he was submitted to a new biopsy requested by a dermatologist, which was suggestive of fibromixoma without signs of malignancy. The patient was referred to the Dermatology service of the Santa Casa de Belo Horizonte for propaedeutic extension. Physical examination showed a lobate erythematous-violet tumor with fibrous consistency of approximately 8 x 6 cm in the abdominal epigastric region (Images 1 and 2).
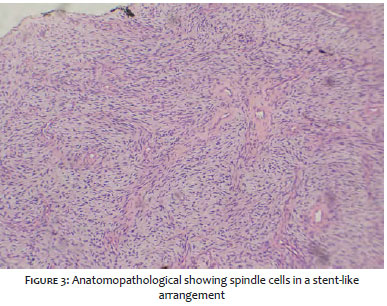
According to the clinical presentation, the main suspicion was DFSP and, therefore, a revision of the anatomopathological slide was performed. The review revealed spindle cells in a storiform arrangement and the material was submitted to immunohistochemical evaluation (Image 3 ). Immunohistochemistry revealed positivity for the CD34 antibody, being conclusive of DFSP, corroborating with the main clinical diagnostic hypothesis.
In addition, the patient was submitted to a nuclear magnetic resonance, to evaluate the extent of the lesion and local invasion. The examination showed multiloculated expansive lesions in the skin and subcutaneous and a hepatic nodule and may correspond to secondary neoplastic involvement. However, the nodule propaedeutics did not show, until now, any relation with the cutaneous neoplasia.
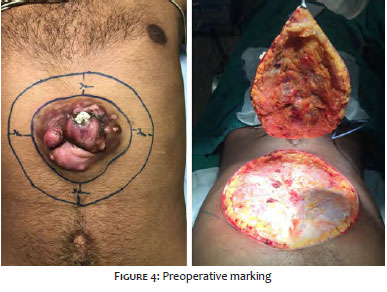
The lesion was excised by the plastic surgery team, with a margin of three centimeters, with removal of the fascia of the rectus abdominis muscle and wall closure by reverse abdominoplasty, with good aesthetic results (Images 4 and 5). As discussed with a pathologist, the anatomopathological of the surgical specimen was compatible with DFSP with fragments of muscle fascia free from neoplasia and the possibility of more aggressive transformation in the part analyzed was excluded.
No adjuvant treatment was given. At the moment, one year after the surgical procedure, the patient has no evidence of local or distant recurrences.
The DFSP is a neoplasm of spindle cells with intermediate malignancy and low risk of metastasis. However, the indolent behavior of the tumor and its inaccurate characteristics often lead to delays in its perception by patients and physicians, leading to delays in diagnosis. Moreover, due to the higher prevalence of cases of basal cell carcinomas, squamous cell carcinomas and cutaneous melanomas, dermatologists are more familiar with the diagnosis, prognosis and treatment of these neoplasms.1,3
The early stage of DFSP can be misdiagnosed as a benign tumor and incompletely excised because it is a nonspecific and asymptomatic lesion. The clinical differential diagnosis includes keloid, dermatofibroma, dermatomyofibroma and morphea.2,7
Proper collection of material for anatomopathological (AP) is extremely important because superficial samples of material for AP may not produce diagnostic material.2
The first intervention is of extreme importance, since tumor spread after the first inadequate resection may lead to uncontrolled local growth or metastasis.1
The high rates of local recurrence accompanied by the high morbidity of DFSP justify the effort in the early diagnosis and the need for initial treatment, which allows a higher rate of cure.3,7,9
Lesions with multiple recurrences after initial treatment appear to be more likely to differentiate into high-grade malignancies with increased risk of metastases.3
The main prognostic factors are inadequate surgical removal with compromised margins, large tumors located in the head and presence of fibrosarcoma areas in histology.3
The treatment with greater curative chances is surgical resection with wide local excision. The microscopic spread of the tumor by projections of tumor cells, similar to tentacles, under clinically normal skin, makes complete surgical removal of the lesion difficult. When possible, Mohs micrographic surgery has the highest cure rates for this tumor.1,3 In this case, we opted for conventional surgery with wide surgical margins made by plastic surgery due to the large extent of the lesion. l
Juliana Chaves Fabrini | 0000-0001-7182-0530
Study design and planning; preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Michelle dos Santos Diniz | 0000-0002-9259-0807
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Mônica Maria de Faria Pimenta | 0000-0002-9075-5903
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript.
Maria Silvia Laborne Alves de Sousa | 0000-0002-2441-2187
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Ralph Brito Damaceno | 0000-0002-2879-6552
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Cassio Ferreira Guimarães | 0000-0002-4328-8994
Approval of the final version of the manuscript; study design and planning; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Fleury LFF, Sanches JS. Sarcomas cutâneos primários. An Bras Dermatol. 2006;81(3):207-21.
2. Bolognia JL, Jorizzo JL, Rapini RP. Dermatology. 4th ed. Elsevier; 2018.
3. Diniz MS, Ramos DG, Nunes MB. Dermatofibrossarcomaprotuberans: localização não usual e a importância da cirurgia micrográfica de Mohs. Surg Cosmet Dermatol. 2013;5(2):173-6.
4. Stojadinovic A, Hoos A, Karpoff HM, Leung DH, Antonescu CR, Brennan MF, et al. Soft tissue tumors of the abdominal wall: analysis of disease patterns and treatment. Arch Surg. 2001;136(1):70-9.
5. Belda Junior W, Chiacchio Di N, Criado PR. Tratado de Dermatologia. 2nd ed. São Paulo: Atheneu; 2014.
6. Rapini RP. Dermatopatologia Prática. 2nd ed. Elsevier; 2012.
7. Llombart B, Serra-Guillén C, Monteagudo C, López Guerrero, JA, Sanmartín O. Dermatofibrossarcoma protuberante: uma revisão abrangente e atualização sobre diagnóstico e manejo. Semin Diagnost Pathol. 2013;30(1):13-28.
8. Diwan AH, Skelton HG, Horenstein MG, Kelly DR, Barrett TL, Bussian AH, et al. Dermatofibrosarcoma protuberans and giant cell fibroblastoma exhibit CD99 positivity. J Cutan Pathol. 2008;35(7):647-50.
9. Cai H, Wang Y, Wu J, Shi Y. Dermatofibrosarcoma protuberans: clinical diagnoses and treatment results of 260 cases in China. J Surg Oncol, 2011;105(2):142-8.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}