


Laís Lopes Almeida Gomes1; Raquel Nardelli de Araujo1; Vando Barbosa de Souza1; Solange Cardoso Maciel Costa Silva1; Igor Eli Balassiano2
Received on: 31/05/2019
Approved on: 26/05/2020
Financial support: None
Conflict of interest: None
Acknowledgement: We thank the Dermatology Service of the
Study conducted at the Universidade do Estado do Rio de Janeiro, Rio de Janeiro (RJ), Brazil
INTRODUCTION: Dermatofibrosarcoma protuberans (DFSP) is a local aggressive sarcoma that presents 60% of recurrences. Rarely it presents lung metastasis too.
METHODS: 41 years old man presented a soft tumor in his right hallux for two years. Histopathology has shown spindle-shaped cells arranged in a storiform manner, and immunohistochemistry was CD34 positive.
DISCUSSION: The literature describes some clinical types of DFSP. The most common are: confluent nodules forming a plaque, sometimes similar to keloids, tumoral lesions, and atrophic plaques.
CONCLUSION: DFSP cases simulating a subcutaneous cyst have been described in the literature; nevertheless, it is an unusual presentation of this tumor.
Keywords: Dermatofibrosarcoma; Sarcoma; Surgical Procedures, Minor
Described previously by Taylor in 1890, dermatofibrosarcoma protuberans (DFSP) is a locally aggressive sarcoma that presents local recurrence in 60% of the cases besides rare metastases, which are also available to lymph nodes.1,2,3
DFSP is a rare and infiltrating connective tissue tumor that represents 1-2% of all sarcomas. DFSP has a prevalence of 0.8 to 5.0 cases per million population per year1 and occurs primarily among youth in the third and fifth decades of life age, although it may occur to people at any age.3,4 Due to the slow and asymptomatic growth of DFSP, the cases diagnosed in adulthood begin in childhood and approximately 20% occurred in children. A study observed that the occurrence of DFSP in black-skinned patients happens two times more in relation to white-skinned ones, while a gender distribution among them is the same.4,5
The trunk is the most affected site (50-60% of the cases), mainly the thorax and shoulders, followed by the proximal region of the limbs (20-30%), being more common in the upper limbs.4,6 Approximately 10 to 15% of cases occur in the head and neck, mainly in the scalp and malar. In children, a tendency to acral presentation of the tumor has been described.7 Hands and feet are affected in about 1% of the cases.8,9
Approximately 85-90% are low-grade lesions whose behavior is an indolent tumor with an average evolution of about 6.4 years at the time of diagnosis.1,3 Occasionally, some areas of differentiation for high-grade sarcoma within the DFSP are found. These cases present a more aggressive behavior and have high rates of recurrence and metastases.3,10
Metastasis are rare and occur in 2-5% of cases. Therefore, CT scans and laboratory tests are not routinely performed. Metastasis can spread hematogenously, usually in more advanced lesions or recurrent lesions, and chest X-rays should be requested for all patients and chest tomography only for those with pulmonary metastasis.4,8,9
The mean size of the DFSP varies from 2 to 5 cm. In cases with late treatment, some lesions may reach 20cm in diameter and present multiple satellite nodules. It is usually restricted to the skin. However, recurrent or old lesions may invade other structures, such as fascia, striated muscle, periosteum, and bones.4
Some reports associate the emergence of DFSP with the HIV virus infection, renal transplantation and antibody deficiency.11 A previous history of trauma is described in about 10-20% of cases, being considered a possible etiologic agent.9
In 1993, the immunoreactivity of this tumor was described for CD34 that today continues as its main immunohistochemical marker, especially if associated with negativity for XIIIa factor.12
Even after extensive resections, there may be local recurrences due to the presence of unexpectedly positive margins, secondary to the microscopic infiltrative pattern of tumor growth. In these cases, a new excision accompanied by a careful histopathological analysis is indicated.3,8,9 The mean time to recurrence is about 2-3 years after excision.3,13,14 We report hitherto the case of a patient with DFSP of unusual location and atypical clinical presentation.
A 41-year-old male presented a softened tumor in the right hallux with growth for two years (Figures 1 e 2). Pain, dyspnea or other symptoms were reported. Chest radiography without alterations.
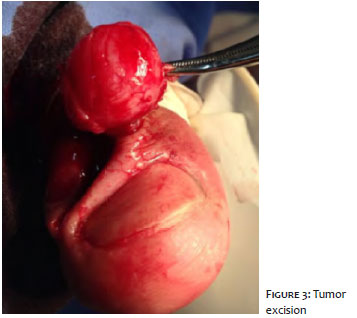
A right-sided CT scan revealed a nodular formation with a density of soft tissues and contrast medium of 1.8 x 1.5cm in the subcutaneous tissue near the interphalangeal joint of the first pododactyl. It also presented discrete erosion of the cortical bone in the epiphysis of the proximal phalanx in contiguity to injury. The patient was referred to the dermatologic surgery for lesion excision. It was performed the hallux garrotrum and fusiform incision above the lesion (Figure 3), with tumor removal and approach of the borders by simple suture with 4-0 wire (Figure 4).
During the surgical procedure, a softened lesion was confirmed, simulating cystic lesions. The histopathological appearance revealed spindle cells in a stent-like arrangement which, upon infiltration of the subcutaneous tissue, shows a honeycomb appearance and a focally positive immunohistochemistry for CD34 (Figure 5). In light of the data presented, the diagnosis of DFSP with positive surgical margins was confirmed. Margin enlargement with freezing was performed and the patient was sent for a radiotherapy procedure.
The progression of DFSP is slowly over a long period of time until it enters a rapidly growing phase.15 Initially, DFSP appears as a hardened, purplish or brownish plaque, attached to the skin, but not to the subcutaneous. After a period that may vary from years to decades, it occurs the proliferation of multiple nodules on the plaque, justifying such a name as protuberans. The DFSP can also appear as a single cutaneous nodule, but it is an unusual clinical presentation.4,8 In the course for the tumor phase or when it already appears in this phase, some differential diagnoses must be remembered, such as epidermal cysts, lipomas or dermatofibromas.4
Some clinical variants are described in the literature, as long as the main ones are: a) confluent nodular lesions forming a plaque, often similar to the keloid one b) tumor lesion c) atrophic plaque. In addition, simulating subcutaneous cyst cases were found in the literature, with similar clinical characteristics to those presented by the current patient.7,16,17
Cystic presentation is unusual.18,19 Gielli et al. presented a series of 27 cases of cystic DFSP observed in a hospital in Italy during a period of 14 years.18 Shivartsbeyn et al. showed by molecular methods that the cell line that formed the pseudocystic part of the DFSP was the same as the main tumor line, allowing the confirmation of the diagnosis and emphasizing that the cyst region was of neoplastic origin and did not represent a secondary reactional proliferation.19
The treatment pillar is performed with complete surgical removal with free margins under light microscope. Two centimeters margins have been suggested in the literature and margins of 5 cm may reach less than 5% recurrence. However, morbidity is proportional to tumor size, which can lead to an increase in complications resulting from the procedure, such as bleeding and surgical wound infections.4,8,20 Furthemore, the surgical procedure may require complex reconstructive techniques and cause functional or cosmetic loss.
After surgery, patients should be followed up every six months for the first three years and annually after that period. Inspection and palpation of the surgical scar are essential.21 Adjuvant radiotherapy is indicated in cases with positive margin when further surgery is not possible. Imatinib (PDGF receptor inhibitor) has been used as the first safe and effective drug in DFSP systemic therapy. Lesions initially assessed as unresectable tumors with metastasis in initial presentation or indication of mutilating surgeries are examples in which the use of such a drug assists in the reduction and subsequent excision of the tumor.3
The cystic aspect is more common in larger tumors. The cause of this cystic transformation is unknown and represent a degenerative phenomenon rather than a histopathological variant.19 However, in the aforementioned patient, the tumor presented reduced size.
Cystic recurrence is rarely observed in sarcomas in general and should be considered as a pseudocystic modification, taking into account that sarcomas, because they are originated from the mesenchymal lineage, would not have true epithelial tissue to form the wall of a cyst. Other sarcomas that may present with formation are endometrial stromal sarcoma, pulmonary synovial sarcoma, and fibroblast sarcoma of the small intestine.19
In high-grade tumors, the cystic portion can be related to degeneration, due to areas of ischemia or necrosis. However, in the aforementioned presented case, the tumor did not have these characteristics as justification of its morphology. In light of that, it is vitally important to emphasize the recognition of this form of DFSP to avoid its misinterpretation as a benign cystic lesion.
Laís Lopes Almeida Gomes | 0000-0001-5396-4362
Preparation and writing of the manuscript; active participation in research orientation; critical literature review; critical revision of the manuscript.
Raquel Nardelli de Araujo | 0000-0003-1443-1621
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; critical literature review; critical revision of the manuscript.
Igor Eli Balassiano | 0000-0001-6229-097X
Study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Vando Barbosa de Souza | 0000-0002-9067-5153
Study design and planning; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Solange Cardoso Maciel Costa Silva | 0000-0003-0812-908X
Approval of the final version of the manuscript; study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Zheng Z, Piao J, Lee JH, Kim SE, Kim SC, Chung KY, et al. Dermatofibrosarcoma Protuberans. A Study of Clinical, Pathologic, Genetic, and Therapeutic Features in Korean Patients, Yonsei Med J. 2015;56(2):440-6.
2. Joucdar S, Kismoune H, Boudjemia F, Bacha D, Abed L, Les dermatofibrosarcomesde Darier et Ferrand e analyse retrospective de 81 cas sur dix ans (1983e1994). [Darrier and Ferrand dermatofibrosarcomas e retrospective analysis of 81 cases over ten years (1983e1994)]. Ann Chir Plast Esthet. 2001;46(2):134-40.
3. Glazer ES, Prieto-Granada C, Zager JS. Current approaches to cutaneous sarcomas: dermatofibrosarcoma protuberans and cutaneous leiomyosarcoma. Curr Probl Cancer. 2015;39(4):248-57.
4. Llombart B, Serra-Guillén C, Monteagudo C, López Guerrero JA, Sanmartín O. Dermatofibrosarcoma protuberans: a comprehensive review and update on diagnosis and management. Semin Diagn Pathol. 2013;30:13-28.
5. Criscione VD, Weinstock MA. Descriptive epidemiology of dermatofibrosarcoma protuberans in the United States, 1973 to 2002. J Am Acad Dermatol. 2007;56(6):968-73.
6. Tarakji MH, Toro A, Carlo ID, Junejo K. Unusual presentation of dermatofibrosarcoma protuberans in a male patient's breast: a case report and review of the literature. World J Surg Oncol. 2015,13(1):158.
7. Gregory JK, Schanbacher CF, Kelly AP, Bennett RG. Dermatofibrosarcoma protuberans growing around plantar aponeurosis: excision by mohs micrographic surgery. Dermatol Surg. 2000;26(10):941-5.
8. Gloster HM. Dermatofibrosarcoma protuberans. J Am Acad Dermatol. 1996;35(3Pt1):355-74, quis 375-6.
9. Sanmartín O, Llombart B, López-Guerrero JA, Serra C, Requena C, Guillén C. [Dermatofibrosarcoma protuberans]. Actas Dermosifiliogr. 2007;98(2):77-87..
10. Lemm D, Mugge LO, Mentzel T, Höffken K. Current treatment options in dermatofibrosarcoma protuberans. J Cancer Res Clin Oncol 2009;135(5):653-65.
11. Lindner NJ, Scarborough MT, Powell GJ, Spanier S, Enneking WS. Revision surgery in dermatofibrosarcoma protuberans of the trunk and extremities. Eur J Surg Oncol. 1999;25(4):392-7.
12. Altman DA, Nickoloff BJ, Fivenson DP. Differential expression of factor XIIIa and CD34 in cutaneous mesenchymal tumors. J Cutan Pathol. 1993;20(2):154-8.
13. Bowne WB, Antonescu CR, Leung DH, Katz SC, Hawkins WG, Woodruff JM, et al. Dermatofibrosarcoma protuberans. A clinicopathological analysis of patients treated and followed at a single institution. Cancer 2000;88(12):2711-20.
14. Liang CA, Jambusaria-Pahlajani A, Karia PS, Elenitsas R, Zhang PD, Schmults CD. A systematic review of outcome data for dermatofibrosarcoma protuberans with and without fibrosarcomatous change. J Am Acad Dermatol 2014;71(4):781-6.
15. Laskin WB. Dermatofibrosarcoma protuberans. CA Cancer J Clin. 1992;42(2):116-25.
16. Maeda D, Minami K, Osaki Y, Miwa H, Hosokawa K, Kubo T. A malignant neoplasm imitating a subcutaneous cyst. Eplasty 2012. Epub 2012 Jul 20.
17. Bathelier E, Ly A, Kanitakis J, Ranchere-Vince D, Chouvet B, Allombert C, et al. Subcutaneous dermatofibrosarcoma protuberans masquerading as a cyst. J Eur Acad Dermatol Venereol. 2007,21(8):1127-8.
18. Gelli R, Urso C, Reali UM. An unusual case of dermatofibrosarcoma protuberans. G Ital Dermatol Venereol. 1990;125(6):263-5.
19. Shvartsbeyn, M, Lazar AJF, Lopez-Terrada D, Meehan SA. Pseudocystic dermatofibrosarcoma protuberans: report of two cases and demonstration of COL1A1-PDGFB rearrangement. J Cutan Pathol. 2012;39(3):356-60.
20. Llombart B, Monteagudo C, Sanmartín O, López-Guerrero JA, Serra-Guillén C, Poveda A, et al. Dermatofibrosarcoma protuberans: a clinicopathological, immunohistochemical, genetic (COL1A1-PDGFB), and therapeutic study of low-grade versus high-grade (fibrosarcomatous) tumors. J Am Acad Dermatol. 2011;65(3):564-75.
21. McPeak CJ, Cruz T, Nicastri AD. Dermatofibrosarcoma protuberans: an analysis of 86 cases-five with metastasis. Ann Surg. 1967;166(5):803-16.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}