


Ary Santos Silva
Received on: 27/02/2018
Approved on: 08/12/201
Financial support: None
Conflict of interest: None
Study conducted at the Department of Plastic Surgery of the Hospital das Clínicas of the Faculdade de Medicina de Marília (HC FAMEMA), Marília (SP), Brazil
Pilomatricoma is an uncommon benign neoplasm of hair follicles, most commonly seen in children. The tumor appears as a solitary and firm nodule, covered with normal epidermis. We report the case of a 26-year-old woman with a lesion in the temporal region. In histological sections, there was an expansive proliferation of islets of epithelial cells configured irregularly, showing the shadow of lost nuclei (ghost cells) in the central area. Pilomatricoma should be considered in the differential diagnosis of skin nodules, especially those of the head, neck, and upper limbs.
Keywords: Hair Follicle; Neoplasms; Pilomatricoma
Pilomatricoma is an unusual benign neoplasm of hair follicles, first described by Malherbe and Chenantois in 1880. In 1961, Forbes and Helwig suggested the name pilomatricoma.1,2 Most of them appear in the first two decades of life, with a second peak occurring in older patients. A solitary and firm nodule, covered with normal epidermis, usually represents the tumor. The tumor can be solid or partially solid and cystic, with calcium deposits also observed, thus justifying the synonym “calcifying epithelioma of Malherbe”.1 The superficial coverage of the skin can turn violet and, in some cases, bleed. It is usually solitary, but literature also describes multiple tumors.3 Most are benign and, rarely, malignant changes are mentioned in the literature.4
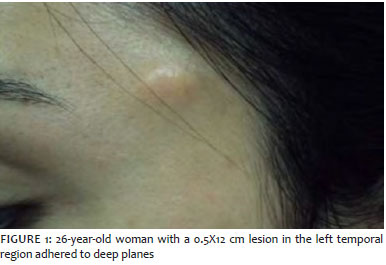
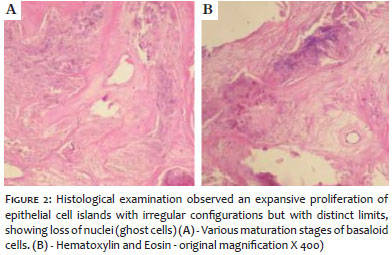
A 26-year-old woman presented a lesion in the left temporal region, with progressive growth and intermittent pain. The physical examination revealed a solid tumor lesion of approximately 0.5 x 1.2 cm in the left temporal region, adhered to the deep plane (Figure 1). The patient reported no previous illness or similar cases in the family. The clinical evaluation and preoperative laboratory tests did not change. Surgical resection of the lesion was performed with safety margins of 1 cm, under local anesthesia. The histological sections showed an expansive proliferation of islets of irregularly configured epithelial cells, which presented distinct boundaries, and a central stained area that showed a shadow of lost nuclei (ghost cells) (Figure 2). The examination demonstrated various stages of maturation of basaloid cells in shadow cells. Therefore, based on histopathological characteristics, the diagnosis of pilomatricoma was confirmed.
Pilomatricoma, or calcifying epithelioma of Malherbe, is a benign epithelial neoplasia. Malherbe and Chenantois described it in 1880 as a calcifying epithelioma derived from sebaceous glands.1,5 Forbis and Helwig later defined the origin of pilomatricoma as the hair follicle’s outer root sheath.2,6 These tumors are commonly present in the head and neck, but other parts of the body have also been reported. They are most common in the age group from 0 to 20 years.7,8 Pilomatricoma usually presents as a single asymptomatic nodule. The skin on the tumor is generally normal, but occasionally it may be reddish or bluish.9 It is generally well-circumscribed, with an oval or spherical shape, and can sometimes be encapsulated.9,10 Multiple tumors are associated with Gardner’s syndrome, Turner syndrome, myotonic dystrophy, sarcoidosis, and Steinert’s disease.11 Malignant transformation of pilomatricoma, although reported, is rare.8,12 The histopathological features of pilomatricoma are a well-circumscribed tumor, lined by a capsule of connective tissue. Pilomatricoma is usually located in the subcutaneous cell tissue, composed of islands of epithelial cells made up of varying amounts of basaloid matrix cells and some cystic changes.6,9 As the tumor matures, there is a central degeneration of the basaloid cells that constitute the ghost cells (anucleated shadows cells) of the uncolored central area, a histopathological characteristic of pilomatricoma.6,9 These basaloid cells tend to decrease in number, and the ghost cells start to predominate.11 The presence of an inflammatory reaction, central calcifications, giant foreign body cells, and keratin debris is also characteristic. With the use of von Kossa stain, 75% of calcium deposits are found in tumors.11 Trichilemmal cysts with loss of nuclei and calcification must be histopathologically differentiated from pilomatricoma. There is a palisade pattern of peripheral basophilic cells in trichilemmal cysts that is not found in pilomatricomas.6,9,12 The differential clinical diagnosis of these tumors should include sebaceous, dermoid, and epidermoid cysts, as well as metaplastic bone formation, foreign body reaction, trichoepithelioma, and basal cell carcinoma.8,12 Surgical excision is the treatment of choice. After adequate excision, tumor recurrence is rare, and long-term follow-up is mandatory.6
Pilomatricomas are benign tumors of skin appendages derived from primitive basal cells of the epidermis, which differ in cells of the hair matrix. They are a relatively rare condition and are more frequent in children.
The treatment of choice is complete surgical excision of the lesion, including the skin covering it in the sample. The recurrence is not frequent, nor the occurrence of the malignant variant of the lesion.
The relative rarity of the tumor justifies this report, and health professionals differentiate it from other tumors in soft tissues.
Ary Santos Silva | 0000-0002-4591-7547
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Malherbe A, Chenantais J. Note sur l' epitheliome calcifié des glandes sebacées. Prog Med. 1880;8:826-8.
2. Forbis R, Helwig EB. Pilomatrixoma (calcifying epithelioma). Arch Dermatol.1961;83:606-18.
3. Moehlenbeck FW. Pilomatrixoma (calcifying epithelioma). A statistical study. Arch Dermatol. 1973;108(4):532-4.
4. Hills RJ, Ive FA. Familial multiple pilomatrixomas. Br J Dermatol. 1992;127(2):194-5.
5. Knight PJ, Reiner CB. Superficial lumps in children: what, when, and why? Pediatr. 1983;72(2):147-53.
6. Birman MV, McHugh JB, Hayden RJ, Jebson PJ. Pilomatrixoma of the forearm: a case report. Iowa Orthop J. 2009;29:121-3.
7. Marrogi AJ, Wick MR, Dehner LP. Pilomatrical neoplasms in children and young adults. Am J Dermatopathol.1992;14(2):87-94.
8. Zaman S, Majeed S, Rehman F. Pilomatricoma-study on 27 cases and review of literature. D:/Biomedica 2009;25:69-72.
9. Kaddu S, Soyer HP, Cerroni L, Salmhofer W, Hödl S. Clinical and histopathologic spectrum of pilomatricomas in adults. Int J Dermatol. 1994;33: 705-8.
10. Schweitzer WJ, Goldin HM, Bronson DM, Brody PE. Solitary hard nodule on the forearm. Pilomatricoma. Arch Dermatol. 1989;125(6):828-9,832.
11. Peterson Wc, Hult AM. Calcifying epithelioma of malherbe. Arch Dermatol. 1964;90:404-10.
12. Chuang CC, Lin HC. Pilomatrixoma of the head and neck. J Chin Med Assoc. 2004;67:633-6.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}