


Thais Furtat Marques; Manoella Freitas Santos; Isadora da Luz Silva; Fabiane Kumagai Lorenzini; Ana Paula Dornelles da Silva Manzoni
Receipt date: 13/04/2020
Approval date: 05/05/2020
Financial Support: None
Conflict of Interest: None
Acknowledgments: The authors thank the resident colleagues and tutors who helped indirectly in this project.
Study conducted at the Dermatology service of the Santa Casa de Miseri- córdia de Porto Alegre, Porto Alegre (RS), Brazil.
INTRODUCTION: Keloids are known to impact the quality of life of their patients. Intralesional corticosteroid injection (ICI) is still the most widely used therapeutic option, although with variable results and limitations. Numerous other strategies have been studied, including the association of lasers with drug delivery (DD).
OBJECTIVES: To compare the therapeutic response between ICI with isolated triamcinolone acetonide and the association of ablative fractional laser (AFL) and DD of the same drug, and assess quality of life.
METHODS: We followed-up eight keloid patients who underwent three sessions with a one-month interval between them. ICI was performed in the right half of the scar and AFL and DD on the left. In assessing the results studied statistically, we used measurement and clinical and photographic comparison of the lesions, the Vancouver clinical and analog pain scales, and the Dermatology Life Quality Index questionnaire.
RESULTS: We observed a statistically significant improvement in keloids with both techniques. In comparison, ICI was significantly higher than the AFL with DD. On the other hand, the latter technique was statistically less painful. As for patients' quality of life, a significant improvement was observed after treatment in both cases.
CONCLUSIONS: Both methods were significantly effective in improving keloids; however, ICI showed to be superior. AFL with DD was better tolerated than ICI and is an interesting option for patients with extensive lesions or low pain tolerance.
Keywords: Drug delivery systems; Injections, Intralesional; Keloid; Lasers; Triamcinolone acetonide
Skin healing is a physiological process in response to tissue damage.1 However, when there is an imbalance between the destruction and deposition of fibroblasts, the appearance of unsightly lesions known as keloid or keloid scars can occur.1 Keloids are elevated, shiny scars that can exceed the limits of the original skin damage. Usually, they are accompanied by itching and/or pain and do not spontaneously involute.2 Its incidence varies between 6-16% in the scientific literature, being more frequent in patients with high skin phototypes and regions such as ear lobe, arms, shoulders, back, and chest.2 Due to its unsightly appearance and symptoms, publications describe a significant impact on these patients’ quality of life (QoL).3
Intralesional corticosteroid injection (ICI) is the most commonly used therapeutic option.6 However, it cannot always be used due to technical limitations such as extensive lesions and pain.9 According to the literature, its effectiveness varies between 50% and 100% of treated cases, and the recurrence rate ranges from 9% to 50%.4 Also, complications may accompany its use, such as the appearance of atrophy, telangiectasias, enlargement of the lesion, and perilesional hypochromia.5
To date, there is no report of a therapeutic method universally accepted as the gold standard for keloids’ treatment.6 Numerous therapeutic strategies have been studied, some of them very promising.2,5 Ablative fractional lasers (AFL) are an option used since the publication of the study by Manstein et al.
5 It can be associated with the topical application of corticosteroids on the micro-perforations resulting from AFL use, a technique known as drug delivery (DD), proposed by Waibel et al. as an alternative of combining treatments to optimize results.9
This study aims to compare the effectiveness between the therapeutic response to keloids from ICI and the association of AFL with corticosteroid DD. The degree of discomfort caused by each treatment modality will also be comparatively analyzed, as well as the impact on the quality of life of patients with keloids.
This study is a quasi-experimental, self-controlled clinical trial, in which the patient is in control of himself. Patients from the outpatient clinics of the Dermatology Service of the Federal University of Health Sciences of Porto Alegre with a clinical diagnosis of keloid were selected.
The sample consisted of individuals over 18 years old with keloids diagnosed clinically by dermatologists and without previous treatments. The patients could not have a previous history of allergy to the components used in the formulation of triamcinolone acetonide, be pregnant, or use medications that reduced tissue healing during the study or in a period less than six months ago (e.g., immunosuppressants and isotretinoin).
All patients agreed to participate in the study by signing the Informed Consent Form. The Declaration of Helsinki’s ethical guidelines were included in this research. A total of eight patients were treated and evaluated with loss to follow-up of one of them during the study.
Procedures
Three sessions were held at monthly intervals. Before completing each treatment session and 30 days after its conclusion, the researcher measured the total extent of the lesions (centimeters), marking a central point that divided them into two equal portions. The lesions were photographed in a standardized way.
ICI and DD were performed with triamcinolone acetonide at a concentration of 5 mg/ml (Kenalog 50% 10 mg/ml suspension - Bristol-Myers Squibb Montréal, Canada – plus saline 50%), using the same volume (1 ml/cm3) for both techniques, in all sessions.
We applied the ICI on the right half of the lesion, and AFL + DD on the left half. The AFL 2940 nm of the Solon® platform (LMG lasers, Guaxupé, MG, Brazil) was used in the ablative fractional mode with 17 J of energy. Immediately after the AFL, triamcinolone acetonide was massaged for 30 seconds over the microperforations, restricted to the keloid’s left half-side. The ICI was distributed homogeneously in the right half-side of the lesion using a 1 ml syringe and 27 G needle.
After applying each of the therapeutic modalities, patients were asked to rate the pain felt using the pain analog scale (zero = no pain to 10 = unbearably painful). At each session, the order in which ICI and AFL + DD were applied was reversed, so it did not influence the pain assessment.
Before starting the treatment and 30 days after its conclusion, the Vancouver clinical scale was adapted to classify keloids in vascularity, pigmentation, texture, and thickness.7 Patients also answered the quality of life questionnaire known as the Dermatology Life Quality Index (DLQI).3
One month after the last session, patients evaluated the improvement on each side of the keloid, according to their perception, giving scores between 0 (no clinical improvement) and 10 (total improvement of the keloid). We invited a dermatologist who was not part of the study and was blinded about the treatments used to evaluate from 0 to 10 each side of the keloid. The grades were given through the pre-treatment analysis one month after therapy’s conclusion photographs, paired in a standardized way in the Windows® Power-Point program. The cutoff point for considering clinical improvement was scores equal to or greater than 5.
The sample size calculation was performed based on a reduction of 55% (6.8 ± 1.96 to 3.05 ± 1.70) on the Vancouver scale (d = 2.03) and considering a significance level of 5% and a power of 90%.
The minimum sample size was estimated at six patients. Statistical treatment was performed using descriptive statistics to characterize categorical variables (absolute and relative distribution), and quantitative variables (measures of central tendency and variability). The Shapiro Wilk nonparametric normality test was applied to the latter. For symmetric variables, the mean and standard deviation were used; and for asymmetric, median, interquartile range, maximum and minimum values were used. For the inference analysis in the comparison before and after the intervention, the t-Student or Wilcoxon tests were used for continuous variables, and the McNemar and Friedman test for categorical variables. The data received statistical treatment using the software SPSS 25.0 (Statistical Package to Social Sciences for Windows) in which, for decision criteria, the significance level (<) of 5% was adopted.
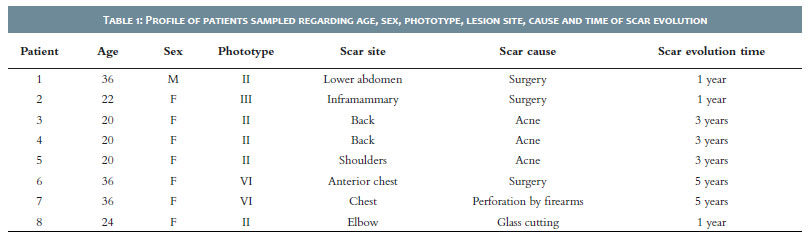
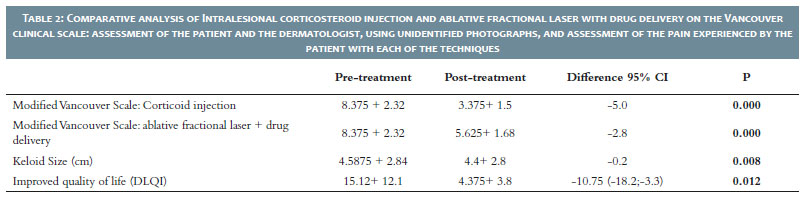
Table 1 shows the patients’ profile regarding age, sex, skin phototype, location, cause and time of evolution of the scar. The clinical analysis before and after treatment using the modified Vancouver clinical scale demonstrated statistically significant improvement of the keloid both on the side treated with ICI (p=0.000) and on the side treated with AFL + corticosteroids DD (p=0.005) (Table 2). When comparing which of the therapeutic options showed the most significant clinical improvement using the modified Vancouver scale, the ICI was significantly higher than the AFL + DD (p=0.003) (Table 3). The score given by the patient regarding the clinical improvement of each half-side of their lesion demonstrated that both the side that received ICI (p=0.014) and the side treated with AFL + DD (p=0.008) improved significantly (Table 4).
Regarding the analysis of the patients' quality of life using the DLQI scale, we found that the subjects obtained a statistically significant improvement in their QoL after the treatment (p=0.012) (Table 2). There was also a significant total scar size reduction after the treatment (p=0.008) (Table 2). Regarding the patient's assessment of the degree of discomfort with each therapeutic modalities using the pain analog scale, the subjects classified the ICI as significantly more painful than the AFL + DD (p = 0.006) (Table 3).
During the five-month follow-up of the sampled patients, complications with any of the treatment modalities were not evidenced.
Dermatologists already use ICI widely to treat keloids, and scientific publications already documented its ability to improve these lesions.6 AFL has its main scientific knowledge based on the facial rejuvenation’s treatment through its ability to remodel collagen in the applied region.8 Similarly, it was postulated that it could assist in the treatment of scars, in addition to inducing a correction of abnormal lymphoproliferative growth, localized tissue hypoxia, and reduced cell growth factors.6,8,10 Also, the microchannels created in tissue ablation can be used to deliver the corticosteroid intralesionally using the DD technique. Thus it’s possible to associate more than one therapeutic option in the same treatment session.6 One of the few consensuses that exist in the current literature on keloids is that we should combine treatments, leading to better outcomes.4,5,6
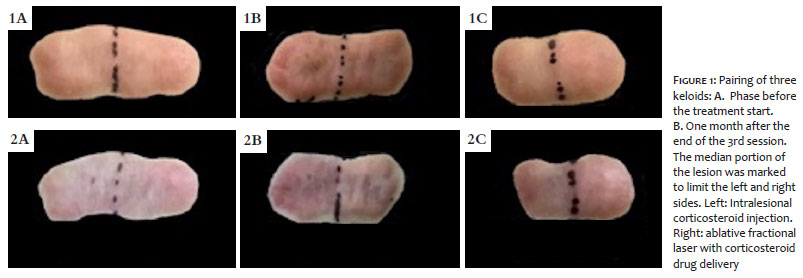
In this study, we found that three sessions with monthly intervals of the association of the AFL with the triamcinolone acetone DD were significantly effective in obtaining a keloid’s clinical improvement (Figure 1) according to the criteria of the modified Vancouver clinical scale (p=0.005) and to the patient's self-assessment (p=0.008). There are few publications in the scientific literature on the treatment of keloids using AFL + DD, and, among them, our study is the one that demonstrated a significant improvement in keloids with the least number of sessions. The improvement in the side treated with ICI is also statistically significant (p=0.000), corroborating previous scientific findings.
Comparing the two techniques studied with each other, using the modified Vancouver scale score, found that the ICI was statistically superior to the AFL + DD in terms of clinical improvement (p=0.003). This result was different from the study by Alexander et al., the scientific publication that most resembles our study regarding the use of AFL + DD.
They demonstrated a superiority of the AFL + DD over the ICI that we believe is due to the more significant number of sessions held, in a total of five sessions with monthly intervals, compared to our work, which totaled three sessions.6
AFL + DD was significantly less painful than ICI (p=0.006) when assessing pain experienced with each therapeutic modalities. We believe that in this finding lies the main highlight for the use of AFL + DD over ICI, as patients with extensive keloid areas tend not to tolerate pain caused by ICI in large extensions.9,10
Regarding the assessment of patients' quality of life before and after the treatment, the results showed a significant improvement after the therapy, corroborating the scientific literature’s findings.4,6 The holistic approach to keloid patients is essential to promote global health status. These patients deal with unsightly lesions, often symptomatic, and with psychosocial discomfort secondary to the condition. Thus, we should not underestimate the suffering that even small keloid lesions can cause to the patient.3
It is noteworthy that no secondary effects were observed with the two treatment modalities during the study period. It demonstrates that both are safe when performed with the correct technique in up to three sessions.
The present study's main limitation is the small sample of patients and the reduced number of sessions. Thus, we aim to expand both the number of patients and the number of total sessions performed. We will also increase the follow-up time to assess the risk of keloid recurrence and analyze whether collagen remodeling continues after the sessions. It was seen in Figure 2 patient who, two months after the final evaluation, demonstrated that the side that received the AFL + DD continued to improve even without further intervention.
We know that when using the same lesion to assess both therapeutic modalities, we face the risk that both procedures would influence the keloid's middle portion. However, we believe that the benefits were more significant than if we used two different keloid lesions. This perception was because we did not observe any difficulty in applying the modified Vancouver clinical scale to each keloid half-side or in the patient's self-assessment of the lesion.
The compared techniques were significantly effective in improving keloids, and the ICI is superior. AFL + DD was better tolerated than ICI, and it is an interesting option for patients with extensive lesions or with low pain tolerance.
Thais Furtat Marques | 0000000166765872
Study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Manoella Freitas Santos | 0000000250245976
Data collection, analysis, and interpretation
Isadora Da Luz Silva | 0000000190848723
Preparation and writing of the manuscript.
Fabiane Kumagai Lorenzini | 0000000163658705
Critical revision of the manuscript.
Ana Paula Dornelles Da Silva Manzoni | 0000000161844440
Approval of the final version of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Arno AI, Gauglitz GG, Barret JP, Jeschke MG. Up-to-date approach to manage keloids and hypertrophic scars: a useful guide. Burns. 2014;40(7):1255-66.
2. Gauglitz GG, Korting HC, Pavicic T, Ruzicka T, Jeschke MG. Hypertrophic scarring and keloids: pathomechanisms and current and emerging treatment strategies. Mol Med. 2011;17(1-2):113-25.
3. Furtado F, Hochman B, Ferrara SF, Dini GM, Nunes JM, Juliano Y, et al. What factors affect the quality of life of patients with keloids? Rev Assoc Med Bras. 2009;55(6):700-4.
4. Erlendsson AM, Anderson RR, Manstein D, Waibel JS. Developing technology: ablative fractional lasers enhance topical drug delivery. Dermatol Surg. 2014;40(Suppl 12):S142-6
5. Lanoue J, Goldenberg G. Acne scarring: a review of cosmetic therapies. Cutis. 2015;95(5):276-81.
6. Alexander S, Girisha BS, Sripathi H, Noronha TM, Alva AC. Efficacy of fractional CO2 laser with intralesional steroid compared with intralesional steroid alone in the treatment of keloids and hypertrophic scars. J Cosmet Dermatol. 2019;18(6):1648-1656.
7. Lee YI, Kim J, Yang CE, Hong JW, Lee WJ, Lee JH. Combined therapeutic strategies for keloid treatment. Dermatol Surg. 2019;45(6):802-810.
8. Waibel JS, Rudnick A, Shagalov DR, Nicolazzo DM. Update of ablative fractionated lasers to enhance cutaneous topical drug delivery. Adv Ther. 2017;34(8):1840-9.
9. Waibel JS, Wulkan AJ, Shumaker PR. Treatment of hypertrophic scars using laser and laser assisted corticosteroid delivery. Lasers Surg Med. 2013;45(3):135-40.
10. Behrangi E, Jalilifar M, Lajevardi V, Razavi V, Azizian Z. Comparative e¿ect of ablative fractional CO2 laser plus triamcinolone acetonide cream versus intralesional injection of triamcinolone acetonide in keloid and hypertrophic scars: a randomized clinical trial. J Skin Stem Cell. In Press(In Press):e69394. Epub 2018 Sept 1.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}