


Maria Laura Marconi França1; Hélio Amante Miot1; Juliano Vilaverde Schmitt1; Thales Vianna Coutinho2
Receipt date: 10/03/2020
Approval date: 12/05/2020
Financial support: FAPESP - Fundação de Amparo à Pesquisa do Estado de São Paulo
Conflict of interest: None
Acknowledgement: We thank FAPESP - Fundação de Amparo à Pesquisa do Estado de São Paulo
Study conducted at the Botucatu Medical School, Botucatu (SP), Brazil
INTRODUCTION: Melasma is frequent among women, and it is associated with a significant psychosocial impact. The facial expressions recognition is a cognitive process directly related to our emotional and psychosocial status.
OBJECTIVES: This study evaluates the melasma patients' ability and healthy controls in identifying facial expressions reflecting six main emotions.
METHODS: This is a cross-sectional study, including 24 melasma patients and 24 healthy controls, matched for age. We collected demographic data, dermatology life quality index (DLQI), Hospital Anxiety and Depression Scale (HADS), and Social Phobia Inventory (SPIN). Also, we conducted a computerized facial emotion recognition test using 56 images.
RESULTS: The participants had a mean age of 39.8 (sd: 8.1), and the melasma patients reported a median of 84 months (p25-p75: 48-144) duration of the dermatosis and a median DLQI of 6 (2-10). Patients with melasma presented higher anxiety scores (9.4 [4] x 6.7 [4.3]; p=0.03) and showed higher accuracy in identifying emotions due to their greater success in recognizing fear (35 [13-52] x 13 [3-25]; p=0.03). The non-biased right answers' difference remained significant after multivariate analysis adjusted for the anxiety scores (p<0.01).
CONCLUSIONS: Women with melasma presented a higher accuracy in recognizing facial expressions of fear, suggesting differentiated brain processing of emotions in this population.
Keywords: Anxiety; Emotions; Melanosis
Melasma is a frequent dyschromia among women and is associated with significant psychosocial impact on patients’ quality of life. It usually begins between the third and fourth decades of life in people with mixed color skin. Despite being associated with chronic sun exposure, genetic factors, and sex hormones, its etiopathogenesis is not fully understood. Changes such as solar elastosis, dermal inflammatory process, and basement membrane damage found in skin with melasma, suggest the role of inflammatory cells such as mast cells and photoaging in the disease’s etiopathogenesis.1–3
Among the psychological changes related to melasma, there has been a greater propensity to stress and anxiety, and emotional processing may be altered in this population. Also, quality of life, understood as a general perception of well-being involving different aspects of the individual’s life, seems to be significantly affected in melasma patients.4,5
Recognition of facial emotions is a cognitive process directly involved with our emotional and psychosocial status. Emotional changes may be related to accuracy in recognizing the different emotions expressed by others.6–8 Recognition and interpretation of emotional facial expressions play a crucial role in adapting to the environment and facilitating social interaction.9
Since 1990, visual affective stimuli have been used in research on emotions, since image visualization has privileged access to the semantic network where affective information is stored.10
In the present study, we assessed the melasma patients’ ability and healthy controls to identify facial expressions of the six main emotions (fear, anger, joy, sadness, surprise, and disgust). We sought to verify if there is any differentiation in this cognitive capacity between groups and some correlation with questionnaires already translated and validated in Brazilian Portuguese about quality of life (DLQI), symptoms of anxiety or depression through the Hospital Anxiety and Depression Score (HADS), and social phobia through the Social Phobia Inventory (SPIN). These characteristics can affect the facial recognition ability of emotions.
A cross-sectional study was conducted with 24 melasma patients and 24 previously age-matched controls without dermatological complaints. The study included women aged 18 to 60 years, recruited from the between January and October 2016, with no difficulties in understanding or communication, no decreased visual acuity, and no accompanying psychiatric comorbidities, according to the participant’s report, after signing the informed consent form.
The institution’s ethics committee approved the study.
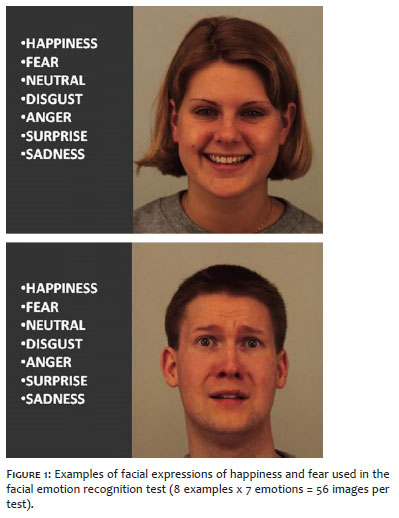
Demographic data were collected, and the Dermatology Life Quality Index (DLQI), Hospital Anxiety and Depression Scale (HADS), Social Phobia Inventory (SPIN) questionnaires, all validated in Portuguese, were applied. Also, we used an emotion recognition test through a computer-assisted facial image. The test randomly displayed, on a 16-inch monitor, eight copies of each illustrated emotion (anger, disgust, joy, neutral, sadness, surprise, and fear) totaling 56 images.11–16 Each image was preceded by a 3 seconds countdown and presented for 0.5 seconds before being hidden, in an adaptation of Calvo’s method (2008).17 The interviewee had free time to indicate which emotion she had recognized after each photo presented, and the image could not be shown again. (Figure 1) The 56 open access facial expression images were obtained from the Karolinska Institute (Solnavägen, Solna, Sweden).18
The HADS questionnaire was used because it is an open-access tool, often used in research on anxiety in medical studies, which reported higher anxiety levels in women with melasma. The report of interference of this feature with the ability to recognize emotions justifies the analysis of social phobia through SPIN, a tool validated for Portuguese.19
Continuous variables were analyzed between the case and control groups by the Student-parametric t-test or the Mann-Whitney non-parametric test according to the normality of the distributions assessed by the Shapiro-Wilk test.20 Categorical variables were compared by the chi-square or Fisher’s exact when the lowest expected value was less than 6. The ability to recognize emotions was assessed by the bias hit index adjusted by a mixed generalized linear model with gamma distribution and post-hoc significance adjusted by the Sidak sequential method.18,21,22
Table 1 compares the demographic and psychometric data between the groups, where there are higher HADS anxiety scores among melasma patients. Patients with melasma had a median of 84 (p25-p75: 48-144) months of disease duration and a median DLQI of 6 (2-10). There was no difference between the groups regarding marital status, income, education or social phobia scores and depression.
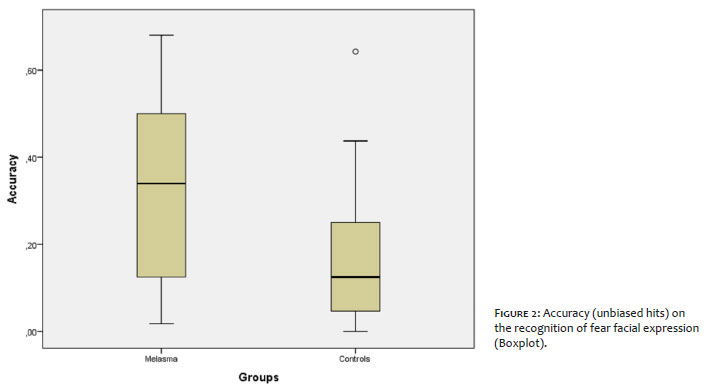
Women with melasma had a greater ability to identify emotions due to better recognition of fear expression (Figure 2). Multivariate analysis, adjusted for HADS anxiety values, confirmed this finding, with better performance only for fear expression (p <0.01). The difference between melasma patients and controls in fear recognition was significant for those with HADS anxiety above 7 (36 [13-50] x 8 [3-16]; p <0.01), but not for those with lower HADS anxiety levels (22 [4-33] x 13 [6-25]; p = 0.46).
There was no correlation between fear recognition scores and HADS anxiety (Rho = 0.08; p = 0.58) or DLQI (Rho = 0.23; p = 0.29) values.
Patients with melasma presented correct identification of facial expression of fear, as well as higher anxiety scores. The significance of the correctness in recognizing emotions was adjusted by Sidak’s sequential method to decrease the chance of such findings occurring at random due to multiple comparisons. Also, the groups were age-matched and had similar education, income, marital status, and depression and social phobia scores.
Previous studies have already identified a possible association between stress and anxiety with melasma, which may be related to facial recognition of emotions. In 2008, a study found that 26.3% of women reported melasma stress as an aggravating factor of the disease, and 28.6% had a previous psychiatric diagnosis between depression and anxiety. 5 Similarly, Bimal et al. (2017) identified high anxiety scores in 36.6% of melasma patients in northern India.23
Wolf et al. (1991) reported two melasma cases that manifested two to three months after acute stressful events (death of family members), with no other obvious risk factors.24 Finally, Handel et al. (2014) found higher levels of anxiety and increased consumption of anxiolytics or antidepressants in women with melasma.4
In addition to reports of the association between stress and anxiety with melasma, the symmetrical facial feature, regularly involving areas innervated by the trigeminal nerve, suggests that the nervous system may play a significant role in the pathophysiology of the disease. In this sense, Bak et al. (2009) identified increased expression of nerve growth factor (NGF) receptors and neural endopeptidase in melasma lesions compared to normal adjacent skin.25
Significant evidence indicates that stress-associated events in animal and human models are associated with changes in NGF production or action. Also, NGF may promote the remodeling of damaged tissues following acute or chronic stressful events.26
Peters et al. (2004) found in animal studies that NGF release is a major step in stress-induced capillary growth and fall, as well as the activation of mast cells and antigen-presenting cells in the skin.27
The present study’s findings indicate that melasma patients have a greater ability to recognize fear facial expressions. Furthermore, Surcinelli (2006) found that people with high anxiety levels have a greater ability to recognize fear in facial expressions.6 Thus, our findings corroborate the observation of a higher anxiety level in women with melasma according to Handel et al.4
Different psychosocial and socioeconomic factors may influence facial recognition of emotions. However, considering age matching and the absence of significant differences regarding marital status, income, and education level between the two groups in the present sample, the findings suggest the existence of a significant relationship between melasma, anxiety, and the ability to recognize facial emotions.
Recognition of fear facial expression is particularly associated with the amygdala’s function, with bilateral lesions in these parts of the brain leading to prominent impairment of this ability.28 Also, Stein et al. (2007) found that people prone to anxiety show greater activation of the amygdala and insula during brain processing of emotions.29
By analyzing subgroups according to HADS anxiety levels, we found that the difference in recognition of fear expression was significant only in participants with higher anxiety scores, suggesting that emotional processing of anxiety may differ between women with and without melasma, leading to different impacts on facial recognition of emotions.
The observed results suggest that melasma patients may present a greater amygdala activity and anxiety propensity; however, causal relationships between this observation and skin changes cannot be concluded in the present study. The trigeminal nerve may be the connection between skin and psychological changes. Effective treatment of persistent generalized anxiety through percutaneous trigeminal electrical stimulation has been reported, indicating the propagation of facial stimuli to nuclei involved in the processing of emotions, such as the amygdala and insula, through extensive connections to the trigeminal nuclei of the brain stem.30–32 Trigeminal stimuli related to amygdala activity could influence inflammatory and pigmentary changes observed in melasma.
The present study has limitations because it is monocentric and only includes patients from the public healthcare system, which may impair the results’ external validity. On the other hand, the results corroborate previous findings from the literature on the subject.
We can conclude that the women with melasma evaluated presented a better performance in recognizing the facial expression of fear, especially among those with higher anxiety levels, suggesting possible connections between the disease’s pathophysiology and characteristics of brain processing of emotions. Although consistent with the literature, this finding should be extended to different groups and centers to verify their external validity.
Maria Laura Marconi França | 0000-0003-0379-4558
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Hélio Amante Miot | 0000-0002-2596-9294
Statistical analysis; approval of the final version of the manuscript; active participation in research orientation; critical revision of the manuscript.
Juliano Vilaverde Schmitt | 0000-0002-7975-2429
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Thales Vianna Coutinho | 0000-0002-7968-0154
Study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. Handel AC, Lima PB, Tonolli VM, Miot LDB, Miot HA. Risk factors for facial melasma in women: a case-control study. Br J Dermatol. 2014;171(3):588-94.
2. Ikino JK, Nunes DH, Silva VPM, Fröde TS, Sens MM. Melasma and assessment of the quality of life in Brazilian women. An Bras Dermatol. 2015;90(2):196-200.
3. Pollo CF, Miot LDB, Meneguin S, Miot HA. Factors associated with quality of life in facial melasma: a crosssectional study. Int J Cosmet Sci. 2018;40(3):313-6.
4. Handel AC, Lima PB, Tonolli VM, Miot LDB, Miot HA. Risk factors for facial melasma in women: a case-control study. Br J Dermatol. 2014;171(3):588-94.
5. Freitag F, Cestari T, Leopoldo L, Paludo P, Boza J. Effect of melasma on quality of life in a sample of women living in southern Brazil. J Eur Acad Dermatology Venereol. 2008;22(6):655-62.
6. Surcinelli P, Codispoti M, Montebarocci O, Rossi N, Baldaro B. Facial emotion recognition in trait anxiety. J Anxiety Disord. 2006;20(1):110-7.
7. Legenbauer T, Vocks S, Rüddel H. Emotion recognition, emotional awareness and cognitive bias in individuals with bulimia nervosa fert. J Clin Psychol. 2008;64(6):687-702.
8. McClure EB, Pope K, Hoberman AJ, Pine DS, Leibenluft E. Facial expression recognition in adolescents with mood and anxiety disorders. Am J Psychiatry. 2003;160(6):1172-4.
9. Haxby JV, Hoffman EA, Gobbini MI. Human neural systems for face recognition and social communication. Biol Psychiatry. 2002;51(1):59-67.
10. Mayer JD, DiPaolo M, Salovey P. Perceiving affective content in ambiguous visual stimuli: a component of emotional intelligence. J Pers Assess. 1990;54(3-4):772-81.
11. Martins GA, Arruda L, Mugnaini ASB. Validação de questionários de avaliação da qualidade de vida em pacientes de psoríase. An Bras Dermatol. 2004;79(5):521-35.
12. Osório FL, Crippa JA, Loureiro SR. Evaluation of the psychometric properties of the Social Phobia Inventory in university students. Compr Psychiatry. 2010;51(6):630-40.
13. Marcolino JAM, Mathias LA da ST, Piccinini Filho L, Guaratini AA, Suzuki FM, Alli LAC. Hospital Anxiety and Depression Scale: a study on the validation of the criteria and reliability on preoperative patients. Rev Bras Anestesiol. 2007;57(1):52-62.
14. Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)--a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):210-6.
15. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361-70.
16. Connor KM, Davidson JR, Churchill LE, Sherwood A, Foa E, Weisler RH. Psychometric properties of the Social Phobia Inventory (SPIN). New self-rating scale. Br J Psychiatry. 2000;176(4):379-86.
17. Calvo MG, Lundqvist D. Facial expressions of emotion (KDEF): identification under different display-duration conditions. Behav Res Methods. 2008;40(1):109-15.
18. Goeleven E, De Raedt R, Leyman L, Verschuere B. The Karolinska Directed Emotional Faces: a validation study. Cogn Emot. 2008;22(6):1094-118.
19. Tseng HH, Huang YL, Chen JT, Liang KY, Lin CC, Chen SH. Facial and prosodic emotion recognition in social anxiety disorder. Cogn Neuropsychiatry. 2017;22(4):331-45.
20. Miot HA, Miot HA. Avaliação da normalidade dos dados em estudos clínicos e experimentais. J Vasc Bras. 2017;16(2):88-91.
21. Kleyn CE, McKie S, Ross AR, Montaldi D, Gregory LJ, Elliott R, et al. Diminished neural and cognitive responses to facial expressions of disgust in patients with psoriasis: a functional magnetic resonance imaging study. J Invest Dermatol. 2009;129(11):2613-9.
22. Wagner HL. On measuring performance in category judgment studies of nonverbal behavior J Nonverbal Behav. 1993;17:3-28.
23. Goyal SK, Thomas EA, Singla M, et al. Depression and Anxiety in Melasma: prevalence and correlates in North India. Ind J Clin Exp Dermatol. 2017;3(4):167-71.
24. Wolf R, Wolf D, Tamir A, Politi Y. Metasma: a mask of stress. Br J Dermatol. 1991;125(2):192.
25. Bak H, Lee HJ, Chang S-E, Choi J-H, Kim MN, Kim BJ. Increased Expression of nerve growth factor receptor and neural endopeptidase in the lesional skin of melasma. Dermatol Surg. 2009;35(8):1244-50.
26. Aloe L, Alleva E, Fiore M. Stress and nerve growth factor: findings in animal models and humans. Pharmacol Biochem Behav. 2002;73(1):159-66.
27. Peters EM, Handjiski B, Kuhlmei A. Neurogenic inflammation in stress-induced termination of murine hair growth is promoted by nerve growth factor. Am J Pathol. 2004;165(1):259-71.
28. Adolphs R, Baron-Cohen S, Tranel D. Impaired recognition of social emotions following amygdala damage. J Cogn Neurosci. 2002;14(8):1264-74.
29. Stein MB, Simmons AN, Feinstein JS, Paulus MP. Increased amygdala and insula activation during emotion processing in anxiety-prone subjects. Am J Psychiatry. 2007;164(2):318-27.
30. Trevizol AP, Shiozawa P, Sato IA, Calfat ELB, Alberto RL, Cook IA, et al. Trigeminal Nerve Stimulation (TNS) for generalized anxiety disorder: a case study. Brain Stimul. 2015;8(3):659-60.
31. Wang J, Li Z-H, Feng B, Zhang T, Zhang H, Li H, et al. Corticotrigeminal projections from the insular cortex to the trigeminal caudal subnucleus regulate orofacial pain after nerve injury via extracellular signal-regulated kinase activation in insular cortex neurons. Front Cell Neurosci. 2015;9:493.
32. Usunoff KG, Itzev DE, Rolfs A, Schmitt O, Wree A. Brain stem afferent connections of the amygdala in the rat with special references to a projection from the parabigeminal nucleus: a fluorescent retrograde tracing study. Anat Embryol (Berl). 2006;211(5):475-96.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}