


Daniela Alves Pereira Antelo; Jaqueline Barbeito de Vasconcellos; Rosane Orofino-Costa
Receipt date: 25/05/2020
Approval date: 30/05/2020
Financial Support: None
Conflict of Interest: None
Acknowledgements: The authors would like to thank Allergan, Dermatus and Dermage for donating the botulinum toxin, phenol solution 88%, and the photoprotector used in this study, and Andréa Reis de Souza Bernardes-Engemann for the guidance in making the figures, graphs, and tables.
Study conducted at the Universidade do Estado do Rio de Janeiro, Rio de Janeiro (RJ), Brazil.
INTRODUCTION: Patients often request anti-aging treatments of the perioral and periorbital regions. Most of the time, it is necessary to use a combination of procedures, so the result meets the patient’s expectations.
OBJECTIVE: This is a prospective, single-center, and comparative study assessing the rejuvenation of the perioral and periorbital regions after treatment with medium depth chemical peel using phenol 88% with or without the previous application of botulinum toxin.
METHODS: Sixteen patients underwent regional peel with phenol 88%; eight received botulinum toxin application two weeks before. The assessment was conducted using standard photographs and evaluation scales by doctors and patients.
RESULTS: The overall evaluation by doctors and patients on the 45th day was considered excellent or good for all patients, with little advantage for combined treatment in the periorbital region.
CONCLUSION: Combining these two relatively low-cost procedures, often overlooked by dermatologists, resulted in a significant improvement in the changes related to aging in these areas.
Keywords: Botulinum toxins type A; Chemexfoliation; Phenol; Rejuvenation
Perioral (POR) and periorbital (POB) aging is a frequent complaint of patients who seek to improve their facial appearance. It consists of static and/or dynamic wrinkles, flaccidity, and actinic changes in the skin, such as elastosis, caused by ultraviolet radiation, senescence, and smoking. These factors contribute to the change in texture and rhytids in areas where the skin is subject to frequent movement.1
It is necessary to combine procedures to obtain a satisfactory result, such as ablative lasers (Erbium or CO2), chemical peels, injections of botulinum toxin (BT) and hyaluronic acid, microfocused ultrasound, microneedling, and dermabrasion.1,2 Some of these procedures have high costs and results that do not always meet patients' expectations.
Unlike the deep peel obtained with the Baker-Gordon formula, phenol 88% is considered an average chemical peel. It affects the superior reticular dermis, promotes neocolagenesis, and attenuates static rhytids.3,4,5
BT injection causes a decrease in muscle contraction. Its application in small doses in the POR and POB regions improves dynamic rhytids and attenuates the static ones.6
This study aims to compare the POR and POB regions’ rejuvenation through the treatment with localized phenol (PP) 88% peeling with and without prior application of botulinum toxin (BT).
Prospective, single-center, and comparative study.
Sixteen healthy women with static and dynamic wrinkles in the POR and POB regions, classified into Fitzpatrick skin phototypes I to III and from the Dermatology Clinic of the State University of Rio de Janeiro, RJ, Brazil, participated in this project after signing the informed consent form. This study was conducted according to the rules issued by the Declaration of Helsinki, revised in 2013.
Electrocardiogram, blood count, and biochemical tests were performed with urea and creatinine levels before application. All patients used the triple combination at night (hydroquinone 4%, tretinoin 0.05%, and fluocinolone acetonide 0.01%) topically for two weeks before the procedure and sunscreen SPF 30, daily, in the morning. The patients were divided into two groups of eight individuals. Group I (GI) received only with PP, and group II (GII) received PP and BT.
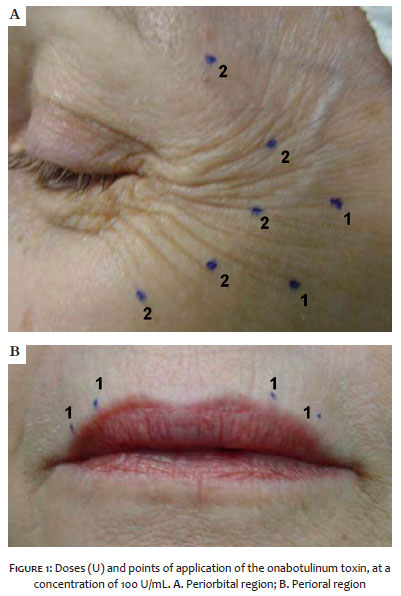
We diluted the onabotulinum toxin (onaBT) in 1 mL of sodium chloride 0.9% (final concentration of 100 U/mL) and applied it to eight patients (GII) two weeks before the peeling. Then, we injected 4 U BT in the POR region and 12 U on each side of the POB region (Figure 1).
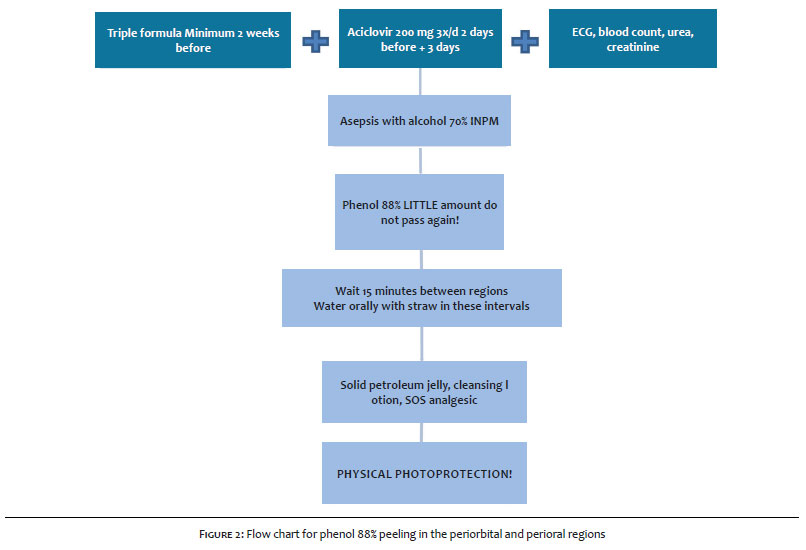
The 16 patients used oral acyclovir (200 mg 8/8h) for five days, starting two days before the PP. After demarcation of the target areas, PP was conducted, using an applicator made by wooden chopsticks wrapped with cotton, containing a small amount of the phenol solution, for application in just one pass.
Between the applications of phenol in the two regions, a time interval of approximately 15 minutes was waited, offering water intake (flowchart, Figure 2). Jessner's solution and trichloroacetic acid (TCA) 35% were applied to the rest of the face, with a layer of Jessner followed by a layer of TCA until homogeneous frosting was obtained.
After the PP, the patients were instructed to use solid vaseline on the whole face and gentamicin cream in the POB and POR areas for seven days, to maintain physical photoprotection during the protocol period and to take analgesics if necessary. The triple formula was reintroduced two weeks after the peels.
Face-to-face and photographic follow-up was performed one week (D7), two weeks (D14), and 45 days (D45) after the peel. The doctor subjectively classified the rhytids before and 45 days after the end of the treatment by their intensity in 1+, 2+ or 3+ (the most intense). The overall final result on D45 was classified as excellent, good, no change, or poor by the doctor and the patient, independently.
Patients’ age ranged between 41 and 78 years, with an average of 56 years (53 in GI and 58 in GII).
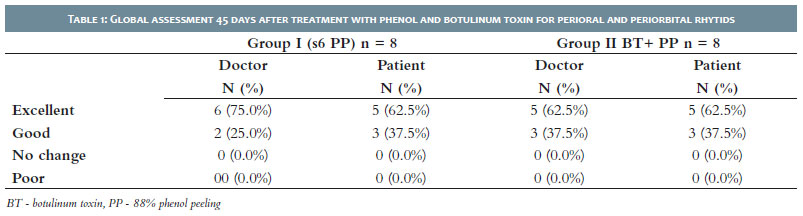
In the global assessment of GI and GII at D45, both physicians and patients considered the result as excellent, most of the time. There was no “no change” or “poor” results in any of the treated groups (Table 1).
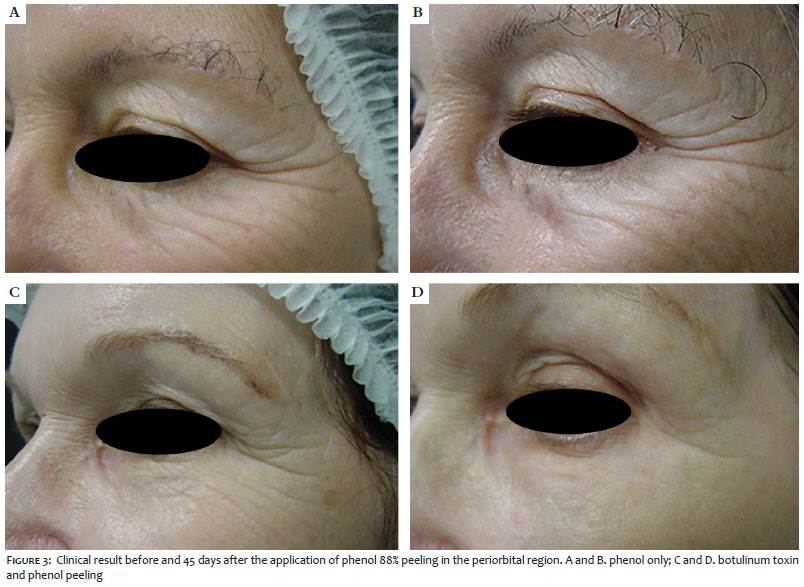
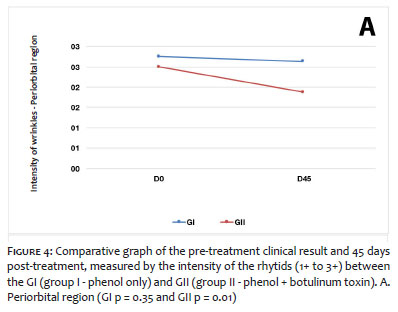
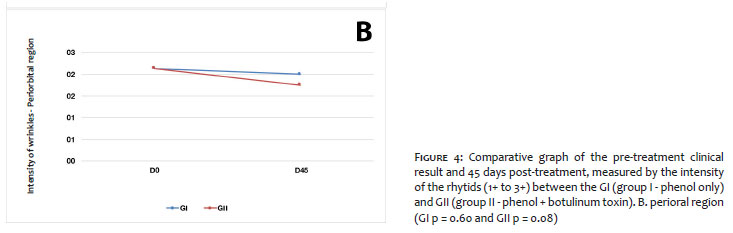
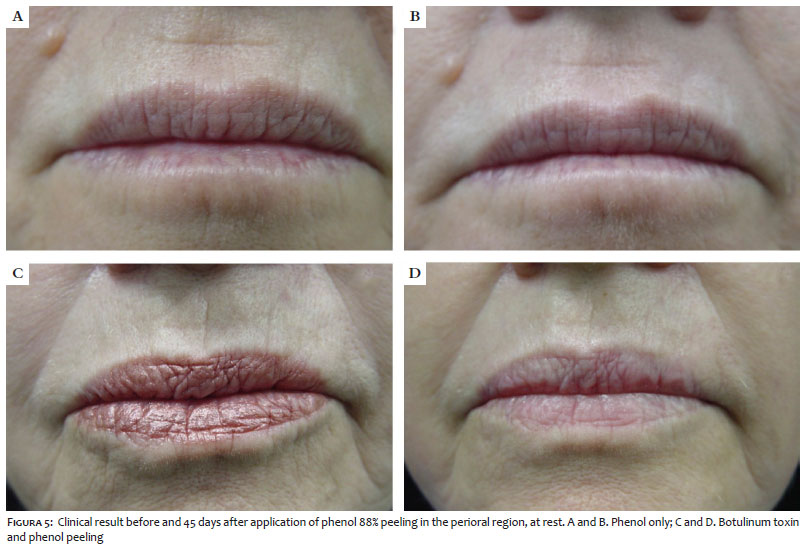
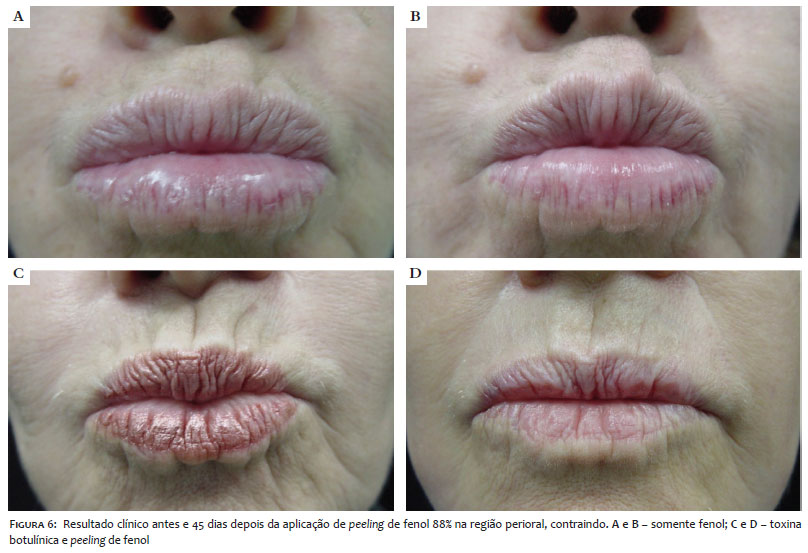
Regarding the intensity of wrinkles in the POB region, GII decreased the score in 5/8 (62.5%) patients, while in GI, only 1/8 (12.5%) patients presented a reduction in the score (Figures 3 and 4A). In the POR region, 3/8 (37.5%) patients in GII achieved the score reduction, while the other 5/8 (62.5%) remained unchanged. In GI, the score decreased in 2/8 (25.0%) patients, while 5/8 (62.5%) remained unchanged, and 1/8 (12, 5%) presented worsening of the score (Figures 4B, 5 and 6).
Regarding adverse events, post-inflammatory hyperchromia in the region treated with PP was observed in 2/8 (25%) patients, being resolved with the reintroduction of the triple formula and maintenance of sunscreen. There were no episodes of herpes simplex in the 16 patients treated.
The rhytids of the periorificial regions of the face are usually considered markers of aging.7 They are also difficult to approach by dermatologists and plastic surgeons due to the skin delicacy, in addition to the mouth and eyes movement and function. Blepharoplasty, dermabrasion, BT, fillers, peels, and ablative lasers are some of the procedures used.8,9
The POR and POB regions’ treatment with PP is a traditional technique, with significant results in static rhytids and low cost. However, some dermatologists restrict their use due to the publication of complications,10 mainly localized hypochromia. Limiting its use to skin phototypes I to III patients and associating Jessner's solution and TCA 35% in the adjacent area are useful measures. They increase safety since the face as a whole receives the skin renewal benefits. The post-inflammatory hyperchromia observed in two of our cases is relatively common in countries with a hot climate and a mixed population. It is usually easy to treat with depigmenting agents and adequate photoprotection.11 Phenol is nephrotoxic and arrhythmogenic, regardless of its concentration or application technique. Therefore, it is essential to conduct laboratory and electrocardiographic evaluations after the anamnesis and physical examination.12 It is advisable to take an interval between applying it in the different regions to accelerate the elimination of phenolic metabolites in the urine, thus reducing the possibility of systemic complications.13
BT mainly treats dynamic wrinkles, being indicated in the face’s periorificial areas, whose movement can leave lines marked permanently.
Combining a procedure to treat static rhytids associated with another for dynamic wrinkles has benefits, as its results will be more evident and more durable. Although the amount of BT used in these regions is small,
PP’s neocolagenesis will have a longer duration.14 For healthy and fair-skinned people, PP is an excellent therapeutic option, at an affordable cost compared to ablative lasers. BT injections before peels also act in the reepithelization and remodeling of collagen in a relatively adynamic environment.15
In this study, despite the small treatment groups and the subjective medical evaluation, a slight difference can be observed between monotherapy with PP and the combined treatment with BT and PP. This result is more evident in the POB region, given that most patients in the GII showed improvement in this area, in contrast to the improvement in only one patient in the GI. When globally assessing the POR and POB treatment, most patients considered the result excellent.
In this comparative study, the treatment of POR and POB rhytids with the association of botulinum toxin and PP was superior to monotherapy with PP and might be another safe and cost-effective option in managing these regions. The best results were obtained in the POB region.
Daniela Alves Pereira Antelo | 0000-0001-8203-1772
Aprovação da versão final do manuscrito; concepção e planejamento do estudo; elaboração e redação do manuscrito; obtenção, análise e interpretação dos dados; revisão crítica da literatura; revisão crítica do manuscrito.
Jaqueline Barbeito De Vasconcellos | 0000-0002-9726-0719
Aprovação da versão final do manuscrito; elaboração e redação do manuscrito; obtenção, análise e interpretação dos dados; revisão crítica da literatura; revisão crítica do manuscrito.
Rosane Orofino-Costa | 0000-0002-1603-418X
Contribuição no artigo: Aprovação da versão final do manuscrito; concepção e planejamento do estudo; elaboração e redação do manuscrito; obtenção, análise e interpretação dos dados; revisão crítica da literatura; revisão crítica do manuscrito.
1. Steiner D, Marçon CR. Terapêutica do envelhecimento cutâneo. In: Kadunc BV, Palermo E, Addor F, Metsavaht L, Rabello L, Mattos R, et al. Tratado de Cirurgia dermatológica, cosmiatria e laser da Sociedade Brazileira de Dermatologia. Rio de Janeiro: Elsevier; 2012. p.322-30.
2. Tamura BM. Avaliação de uma técnica simplificada para tratamento de rítides da região perioral e periorbicular com laser de CO2. Surg Cosmet Dermatol 2012;4(3):237-40.
3. Soleymani T, Lanoue J, Rahman Z. A. Practical approach to chemical peels: a review of fundamentals and step-by-step algorithmic protocol for treatment. J Clin Aesthet Dermatol. 2018;11(8):21-8.
4. Velasco MVR, Okubo FR, Ribeiro ME, Steiner D, Bedin V. Rejuvenescimento da pele por peeling químico: enfoque no peeling de fenol. An bras Dermatol. 2004;79(1):91-9.
5. Lee KC, Sterling JB, Wambier CG, Soon SL, Landau M, Rullan P, et al. Segmental phenol-Croton oil chemical peels for treatment of periorbital or perioral rhytides. J Am Acad Dermatol. 2019;81(6):e165-6.
6. Dorizas A, Krueger N, Sadick NS. Aesthetic uses of botulinum toxin. Dermatol Clin. 2014;32(1):23-36.
7. Honigman R, Castle DJ. Aging and cosmetic enhancement. Clin Interv Aging. 2006; 1(2):115-9.
8. Ozturk CN, Huettner F, Ozturk C, Bartz-Kurycki MA, Zins JE. Outcomes assessment of combination face lift and perioral phenol-croton oil peel. Plastic and Reconstructive Surgery. 2013;132(5):743-53.
9. Danhof RS, Cohen JL. A combination approach to perioral rejuvenation. J Drugs Dermatol. 2016;15(1):111-2.
10. Bagatin E, Hassun K, Talarico S. Revisão sistemática sobre peelings. Surg Cosmet Dermatol. 2009;1(1):37-46.
11. Davis EC, Callender VD. Postinflammatory hyperpigmentation: a review of the epidemiology, clinical features, and treatment options in skin of color. J Clin Aesthet Dermatol. 2010;3(7):20-31.
12. Kadunc BV, Vanti AA. Avaliação da toxicidade sistêmica do fenol em peelings faciais. Surg Cosmet Dermatol. 2009;1(1):10-4.
13. Starkman SJ, Mangat DS. Chemical Peel (Deep, Medium, Light). Facial Plast Surg Clin North Am. 2020;28(1):45-57
14. Gart MS, Gutowski KA. Overview of botulinum toxins for aesthetic uses. Clin Plastic Surg. 2016;43(3):459-71.
15. Zimbler MS, Holds JB, KokoskaMS, Glaser DA, Prendiville S, Hollenbeak CS, et al. Effect of botulinum toxin pretreatment on laser resurfacing results. Arch Facia Plast Surg. 2001;3(3):165-9.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}