


Welly Wijayanti; Khairuddin Djawad
Receipt date: 12/06/2020
Approval date: 07/09/2020
Financial Support: None
Conflict of Interest: None
Acknowledgments: The authors would like to thank Ivan Kurniadi, MD, for his technical support.
Study conducted at the Department of Dermatology and Venereology, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia.
INTRODUCTION: Basal cell carcinoma (BCC) is the most common cancer in the world. Although rarely metastasizes, BCC can cause high levels of morbidity due to its locally destructive nature. Local flaps provide reasonable option for reconstruction of facial defects with good result.
OBJECTIVE: Describe the clinical profile of BCC in South Sulawesi, Indonesia.
METHODS: A retrospective analysis was performed in all patients with BCC who had undergone surgical resection in our center. Patient charts were reviewed for demographic information, tumor size, anatomic location, clinical subtype, and surgical method.
RESULTS: There were 70 BCC cases consisting of 18 (25.7%) men and 52 (74.3%) women. The most frequent age group was 46 to 65-year-old group (49 patients, 70%). The most common aesthetic unit affected was the nasal unit (24 patients, 34.3%) with lesions measured 1 cm to 2 cm in diameter (45 patients, 64.29%). The most common clinical subtype was nodular type (37 patients, 52.86 %). Advancement flap was the most frequent technique used (32 patients, 45.71%).
CONCLUSIONS: BCC more frequently occurs in females, on the nose, and in the age range of 46 to 64 years old. Local flaps resulted in an excellent aesthetic result and are the first choice for reconstruction of the face.
Keywords: Basal cell; Carcinoma; Retrospective studies; Surgical flaps
Skin cancer is the most common type of cancer. It can be differentiated based on the type of cells found in each lesion into basal cell carcinoma (BCC) (77%), squamous cell carcinoma (SCC) (20%), malignant melanoma (3%), and rare tumors originating from the skin (<1%). Anatomical distribution mostly favors the head and neck region, where this location constitutes 85% of BCC and 75% of SCC.1
Among all skin cancers, BCC is the most common type. Although it rarely metastasizes or leads to death, BCC can cause high morbidity due to its locally destructive nature. The high prevalence of BCC allows us to understand better the disease characteristics, pathogenesis, clinical and histopathological features.2
The finding that BCC occurs mainly on sun-exposed sites and that sun protection can reduce its frequency provides indirect but crucial evidence for the role of ambient solar radiation.3 Intermittent intense episodes of UV exposure and sunburns at any age appear to increase the BCC risk. In contrast, cumulative long-term UV exposure and childhood sunburns increase the risk of developing SCC.4 Geographic location also has been implicated as a risk factor for BCC, and populations living in geographic regions with latitudes closer to the equator have reported higher rates of BCC than other populations.5
BCC generally occurs in individuals older than 50 years, but not much is known about its incidence in subjects younger than 40 years. To date, studies that aimed to investigated BCC in younger populations were unable to find any trends.6
Surgical excision may be the most effective treatment for primary BCC, and it has been traditionally the main treatment of choice. BCC is typically removed with a pre-set excision margin of 0.3-0.4 centimeter (cm). In BCC cases on the face, grafts and flaps are more recommended for wound closure than direct closure.7
In the past decade, several studies have examined the relationship between age, gender, and anatomical distribution regarding different BCC variants, including nodular, superficial, and morpheaform BCC. Recent literature suggests that the anatomical location of BCC may favor the development of particular subtypes.8 Yet further studies are needed to clarify these associations. This study aims is to describe the clinical profile of BCC in South Sulawesi, Indonesia.
We retrospectively analyzed data of all patients with facial BCC who presented to the Tumor and Skin Surgery Clinic of the Department of Dermatology and Venereology, at Makassar, from January 2015 to January 2020.
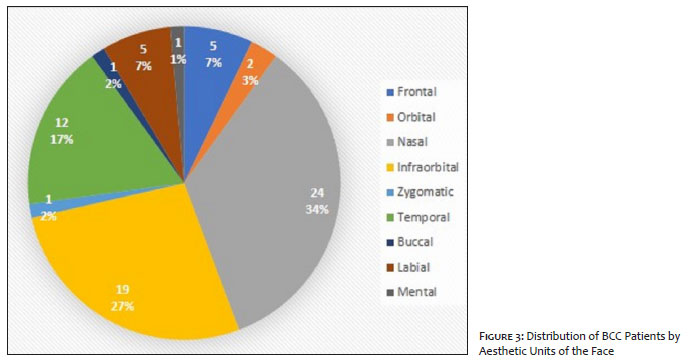
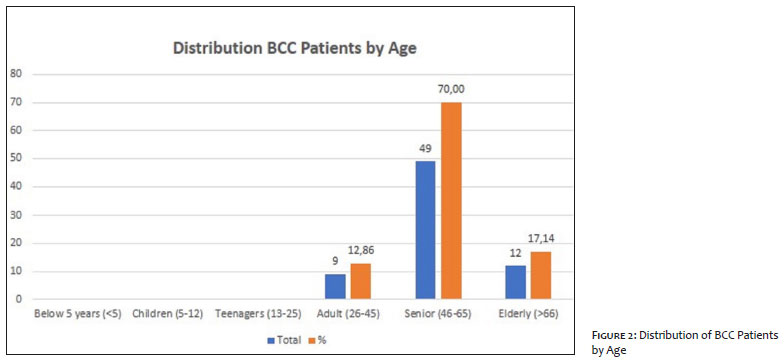
We reviewed patient charts for demographic information (age and sex), anatomical location, tumor size in diameter, clinical subtype, and surgical treatment method. Six age categories were established: (1) younger than 5 years of age, (2) 5 to 12 years of age, (3) 13 to 25 years of age, (4) 26 to 45 years of age, (5) 46 to 65 years of age, (6) older than 66 years of age. Anatomical location divided into 12 aesthetic units according to Gonzales-Ulloa, 1975: (1) frontal, (2) temporal, (3) auricular, (4) supraorbital, (5) orbital, (6) infraorbital, (7) zygomatic, (8) buccal, (9) nasal, (10) labial, (11) mental, and (12) parotid-mesenteric (Figure 3). Tumors were divided into four subtypes, according to Fitzpatrick et al. (2019): (1) nodular, (2) pigmented, (3) superficial, and (4) morpheaform. The method of surgical treatment by local flap was divided into five groups: (1) advancement flap, (2) rotation flap, (3) transposition flap, (4) combination of rotation and advancement flap, and (5) combination of transposition and advancement flap.
We were able to generate meaningful summary statistics, and we summarized the results, reporting them as mean or percentage, chart, and table. Mean and standard deviation was calculated for the age at presentation and size of the lesion. Frequency and percentages were calculated for all data. The data were analyzed using SPSS version 25.0 software (SPSS Inc., Chicago, IL, USA).
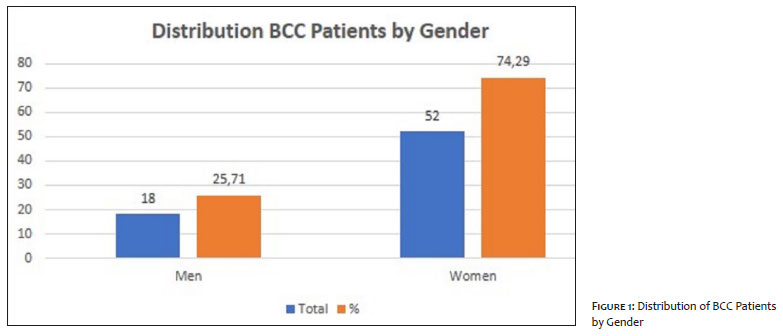
We retrieved a total of 70 facial BCC cases. Of these cases, 18 (25.72%) patients were men, and 52 (74,29%) were women with overall men to women ratio of 1:2.8 (Figure 1). The age distribution ranged from 30 to 80 years old. The most frequent age group was 46-65 years old (mean 60.06 ± 4.33 years), followed by 66 years old and above (Figure 2). Of these groups, the sixth decade was found to be the peak age of presentation.
Anatomic Distribution
We further analyzed the location of face tumors by reviewing the preoperative photographs and categorizing each tumor to 12 aesthetic units of the face, according to Gonzales-Ulloa, 1975.9 The most common site was the nose, where tumors occurred in 24 (34%) cases, followed by the infraorbital area, which was involved in 19 (27%) cases (Figure 3).
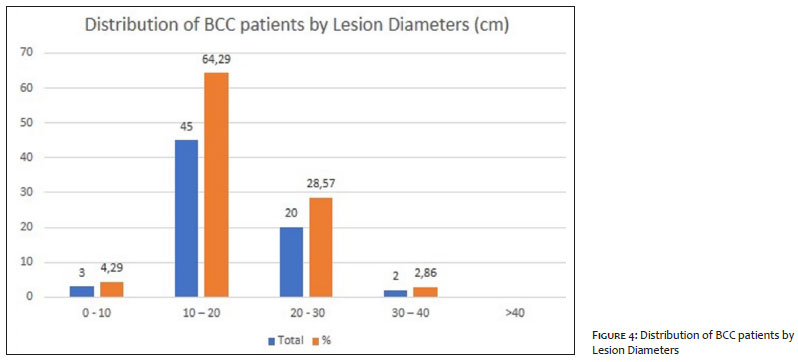
The smallest tumor was 0.5 cm in diameter, and the largest was 3.5 cm. The majority of tumors had a diameter between 1 cm and 2 cm in 45 (64,29%) cases, followed by 2 cm to 3 cm in 20 (28,57%) cases. The average tumor diameter was 1.8 cm (Figure 4).
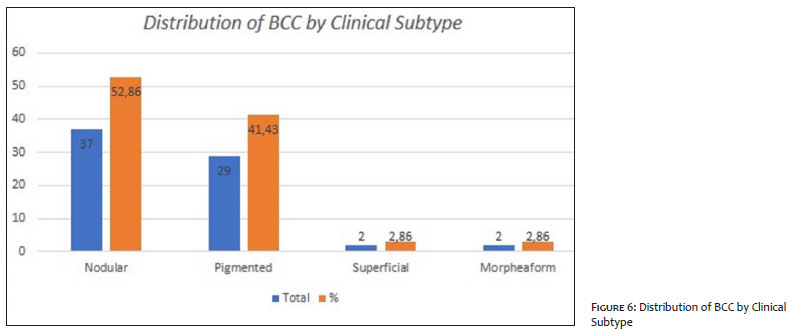
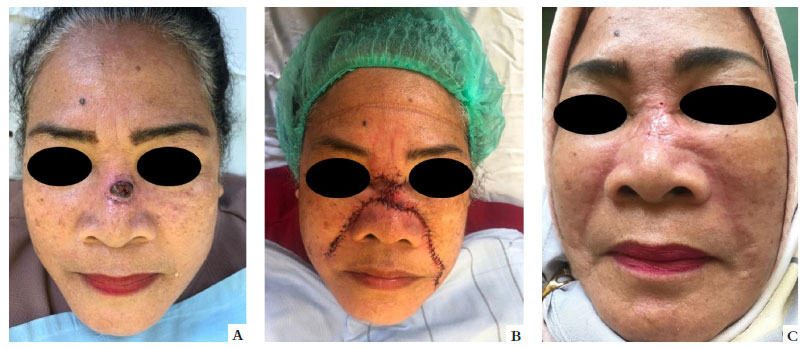
The BCC clinical subtype was divided into four types (nodular, pigmented, superficial, and morpheaform) using preoperative photographs (Figure 5). The most common clinical subtype was the nodular type, seen in 37 (52,86%) cases, followed by the pigmented type in 29 (41,43%) cases (Figure 6).
Surgical Treatment
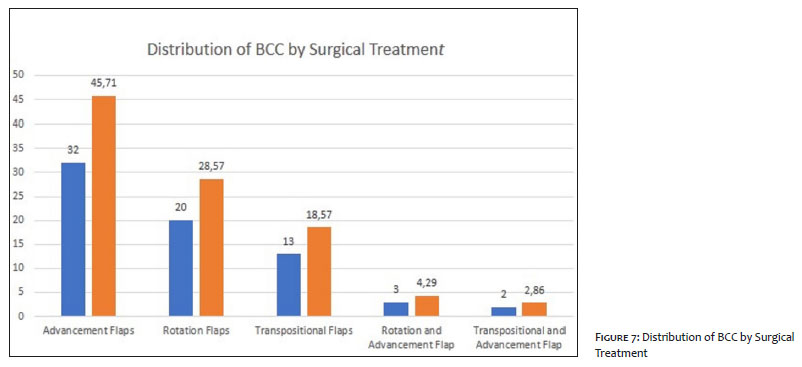
All 70 tumors were treated by excision with surgical margins of 0.4 cm to 0.5 cm. There was no recurrence in one to five years follow-up. The most commonly used method of wound closure was local flap. In all cases of local flaps, the most common technique was advancement flap (32 cases, 45.71%), followed by rotation flap (20 cases, 28.57%) (Figure 7).
We also analyzed the operative methods by aesthetic units. Among all advancement flaps cases, the most commonly treated area was the nose (9 cases, 28.12%) and the infraorbital unit (9 cases, 28.12%). Rotation flap was commonly used in the infraorbital unit (8 cases/40.00%), and transposition flap was frequently used in the nose (8 cases, 61.54%). The combination of rotation and advancement flap was commonly used in the nasal unit (2 cases, 66.67%), and the combination of transposition and advancement flap was mostly used in the nasal and infraorbital unit.
Skin cancer is the most frequent type of malignancy with a gradually increasing incidence throughout the world. Although it rarely metastasizes or leads to death, BCC can cause high morbidity due to its locally destructive nature.2
In the present study, the subjects’ age ranged from 30 to 80 years, with a mean age of 59.25 ± 10.11 years. The age group with the highest incidence of BCC was the 46-65 years (mean 60.06 ± 4.33 years). The mean age was similar to that reported by Matthew et al., 66.9 ± 15.1 years, and by Martha et al., of 60 years.(10,11) The most common variety of carcinoma is BCC, which accounts for 77% of all skin cancer cases and is more frequent in the elderly population, reflecting the connection between accumulative sun exposure and cancer development.1
BCC occurs mainly on sun-exposed sites. It suggests that cumulative lifetime sun exposure has a strong dose-response association with BCC.3 Chronic UV exposure is the highest risk factor for BCC, with a typical latency period of 15 to 20 years between the UV damage and the clinical onset. The UV dose, exposure duration and intensity all play a role in BCC development.12 UV exposure, particularly the UVB spectrum, is accepted as the most important causal factor for BCC development. UV light is believed to directly induce DNA mutations via covalent bonding between adjacent pyrimidines (UVB) and form reactive oxygen species (UVA).13 Geographic location has also been implicated as a risk factor for BCC, where populations living in geographic areas with latitudes closer to the equator have reported higher rates of BCC than other populations.5 Thus, the fact that Indonesia is located in the equator and has about 5000 km or 1/8 of the equatorial circumference in longitude played a significant role in the occurrence of BCC in our cohort.14
This study presented men to women ratio of 1 to 2.8. BCC is traditionally more commonly in men due to their more extensive exposure to sunlight. However, in a previous retrospective review assessing a period between 2005 and 2012, Choi et al. found BCC to be more common among women, with men to women ratio of 1:1,38.9 Nicolo et al. found that BCC is more common in women than men, with a ratio of 1:0.9. This greater incidence among women was believed to be due to female population’s the higher life expectancy.15 Mancuso et al. study showed that the development of skin cancer might be related to sex hormones such as estrogen, but such relationship has not been studied extensively in the clinical or epidemiologic setting. An animal study found that endogenous estrogen antagonized basal and squamous skin tumorigenesis induced by physical or chemical agents.16
In the current study, there were 70 BCC cases in the facial region. Neoplasm of the skin is more frequently found on the face because it is continuously exposed to UV radiation with no protection.17 Cosmetically, the face is the most significant anatomic space for many patients. Thus, malignant facial neoplasms pose a challenge in treatment: to have an oncologically accountable surgery and, at the same time, optimal cosmetic outcome.18 Analysis on the anatomical site for the occurrence of 70 cases BCC showed that the nose was the most common location, with 24 cases (34%), followed by the infraorbital area, with 19 (27%) cases. A study on 138 cases of BCC by Kang et al. showed a similar finding, where the nose was the most common site for BCC (44 of 138 cases, 31.9%).1 Omer et al. retrospectively reviewed 171 cases of BCC in the head and neck region and reported that BCC was more frequent in the nose (53 cases, 46,3%).19 Firas et al. showed in 335 cases of BCC that the face was the most commonly affected site in both men (77%) and women (83%). It reflects the importance of solar radiation as the main causative factor in the pathogenesis of this condition.20
BCC on the nose is expected, including on the nasal tip, because the nose is the most projected portion of the face and is more exposed to UVR.15 Larger tumors can infiltrate and eventually destroy the neighbor areas due to muscle infiltration in the distal half of the nasal area, and, subsequently, the cartilage. BCCs of the lateral sidewall may also extend to the nasolabial fold and infiltrate the muscles and the orbicularis oculi in advanced stages. Also, BCCs present on the nasal root, albeit rare, present a challenging defect closure due to its proximity with the medial canthus.21
In the present study, the mean tumor diameter was 1.8 cm. Most tumors measured between 1 cm and 2 cm in diameter (45 cases, 64.29%). In a previous retrospective review, Kang et al. found the most common tumor size was from 1 cm to 2 cm in 69 cases (50%), with a mean of 1.5 cm.1 Metastasis is expected to occur in tumors larger than 3 cm in diameter, with a risk of metastasis up to 1-2%. This risk increases to 20-25% and 50% in tumors with 5 cm and larger than 10 cm in diameter, respectively. A BCC larger than 10 cm in diameter is referred to as “giant” and poses a significant risk for morbidity and mortality.6
In our population, nodular BCC was the most frequently observed subtypes, and it was seen in 37 (52,86%) cases. This result is similar to that found by Codazzi et al., who observed the nodular subtype in 62.4% cases. This subtype more frequently develops on sun-exposed areas.22 It typically presents a shiny, pearly papule or nodule with a smooth surface, rolled borders, and arborizing telangiectasias. Moreover, slow-growing, advanced tumors can become large and ulcerate, classically referred to as a “rodent ulcer”. Advanced, infiltrative tumors can distort the structures they invade.23
All 70 tumors were treated by excision with surgical margins of 0.4-0.5 cm for complete clearance, and there was no recurrence in one to five years follow-up. The European Dermatology Forum (EDF) guidelines on surgical excision margin recommended the excision of BCC measuring less than 2 cm in diameter with 0.3 cm to 0.4 cm margin. In contrast, in cases of high-risk BCC, larger than 2 cm, the Forum recommended a margin of 0.5 cm to 1 cm. The EDF cited that previous studies showed complete clearance in 95% cases when such margins were used.24 Current guidelines suggest a range of peripheral margins between 0.2 cm and 0.5 cm in low-risk BCC and from 0.5 cm to 1.5 cm in high-risk lesions.25
All reconstructions in this study were successful without any significant aesthetic or functional deformity. The most commonly used method of wound closure was local flap. All flaps survived without complications; there were no reports of hematoma, seroma, or severe infection. Advancement flap was the most frequently used flap technique (32 cases, 45.71%). The local flap was also the method of choice in a previous study (102 cases, 74.4%) and consisted of advancement flap, rotation flap, forehead flap, and transposition flap.26
In the advancement flap (Figure 8), the movement goes in a straight line parallel to its major axis, from the donor site to the recipient. This maneuver is possible due to the skin donor’s elasticity, resulting in a gain directly proportional to the flap’s length. On the other hand, to prevent ischemic necrosis of the flap’s apex, it is essential to respect a ratio of at least 3:1 between the major and minor axis of the flap.27 The mobilization can be facilitated by the excision of two Burrow’s triangles (exhaustion method) on the flap base. Dual opposing (H-plasty) can be advantageously exploited in specific anatomic sites where it is necessary to keep aesthetic continuity (eyebrow, forehead, nose bridge, helix rhyme).28
The small number of subjects, and the inclusion of only one institution, limited our study. Future large-scale studies with additional data such as onset and recurrences will help better to delineate the BCC’s nature and corresponding optimal treatment.
Basal cell carcinoma is the most common type of malignant facial skin lesion. Our study showed that BCC more frequently occurs in women, on the nose, and in the group age of 46 to 64 years. The nodular subtype is the most common subtype with a 1-2 cm diameter, consistent with previously published reports. The advancement flap resulted in satisfactory facial reconstructive results, both cosmetically and functionally, following surgical excision.
Welly Wijayanti | 0000-0003-4862-8617
Análise estatística; aprovação da versão final do manuscrito; concepção e planejamento do estudo; elaboração e redação do manuscrito; obtenção, análise e interpretação dos dados; participação intelectual em conduta propedêutica e/ou terapêutica de casos estudados; revisão crítica da literatura; revisão crítica do manuscrito.
Khairuddin Djawad | 0000-0002-2316-1339
Aprovação da versão final do manuscrito; concepção e planejamento do estudo; elaboração e redação do manuscrito; revisão crítica do manuscrito.
1. Kang KW, Lee DL. A retrospective clinical view of basal cell carcinoma and squamous cell carcinoma in the head and neck region¿: a single institution's experience of 247 cases over 19 years. Arch Craniofac Surg. 2016;17(2):56-62.
2. Marzuka AG, Book SE. Basal cell carcinoma: pathogenesis, epidemiology, clinical features, diagnosis, histopathology, and management. Yale J Biol Med. 2015;88(2):167-79.
3. Madan V, Lear JT, Szeimies R. Non-melanoma skin cancer. Lancet [Internet]. 2010;375(9715):673-85.
4. Soyer HP, Rigel DS, McMeniman E. Actinic keratosis, basal cell carcinoma, and squamous cell carcinoma. In: Bolognia JL, Schaffer JV, Cerroni L, editors. Dermatology. 4th ed. UK: Elsevier; 2018. p. 1883.
5. Wu S, Han J, Vleugels RA, Puett R, Laden F, Hunter DJ, et al. Cumulative ultraviolet radiation flux in adulthood and risk of incident skin cancers in women. Br J Cancer. 2014;110(7):1855-61.
6. Hakverdi S, Balci DD, Dogramaci CA, Toprak S. Retrospective analysis of basal cell carcinoma. Indian J Dermatol Venereol Leprol. 2011;77(2):251.
7. Smith V, Walton S. Treatment of facial basal cell carcinoma¿: a review. J Skin Cancer. 2011;2011:380371. Epub 2011 Apr 27.
8. Rivers JK, Mistry BD, Hung T, Vostretsova K, Mistry N. A 13-Year retrospective study of basal cell carcinoma in a canadian dermatology practice¿: a comparison between anatomical location and histopathologic subtypes. J Cutan Med Surg 2016;20(3):233-40.
9. Choi JH, Kim YJ, Kim H, Nam SH, Choi YW. Distribution of basal cell carcinoma and squamous cell carcinoma by facial esthetic unit. Arch Plast Surg. 2013;40(4):387-91.
10. Cho M, Lee J, James CL, Marshman G, Huilgol SC. Scalp basal cell carcinoma: review of 2,202 cases. Dermatol Surg. 2016;42(7):834-41.
11. Vaca-Aguilera MR, Guevara-Gutiérrez E, Barrientos-García JG, Tlacuilo-Parra A. Giant basal cell carcinoma: clinical-histological characteristics of 115 cases. Int J Dermatol. 2019;58(12):1430-1434.
12. Kauvar ANB, Cronin T, Roenigk R, Hruza G, Bennett R. Consensus for nonmelanoma skin cancer treatment: basal cell carcinoma, including a cost analysis of treatment methods. Dermatol Surg. 2015;41(5):550-71.
13. Tsatsou F, Trakatelli M, Patsatsi A, Kalokasidis K, Sotiriadis D. UV-mediated skin carcinogenesis extrinsic aging. Dermatoendocrinol. 2012;4(3):285-97.
14. Yamanaka MD. Physical climatology of Indonesian maritime continent¿: an outline to comprehend observational studies. Atmos Res. 2016;178-179:231-59.
15. Bertozzi N, Simonacci F, Grieco MP, Grignaffini E. Single center evidence for the treatment of basal cell carcinoma of the head and neck. Acta Biomed. 2019;90(1):77-82.
16. Mancuso M, Gallo D, Leonardi S, Pierdomenico M, Pasquali E, Stefano I De, et al. Modulation of basal and squamous cell carcinoma by endogenous estrogen in mouse models of skin cancer. Carcinogenesis. 2009;30(2):340-7.
17. Nakayama M, Tabuchi K, Nakamura Y, Hara A. Basal cell carcinoma of the head and neck. J Skin Cancer 2011:496910.
18. Rao JK, Shende KS. Overview of local flaps of the face for reconstruction of cutaneous malignancies: single institutional experience of seventy cases. J Cutan Aesthet Surg. 2016;9(4):220-5.
19. Janjua OS, Qureshi SM. Basal cell carcinoma of the head and neck region: an analysis of 171 cases. J Skin Cancer. 2012;2012:943472. Epub 2012 Dec 19.
20. Al-qarqaz F, Marji M, Bodoor K, Almomani R, Gargaz W Al, Alshiyab D, et al. Clinical and demographic features of basal cell carcinoma in North Jordan. 2018;2018:2624054. Epub 2018 Oct 4.
21. Wollina U, Bennewitz A, Langner D. Basal cell carcinoma of the outer nose: overview on surgical techniques and analysis of 312 patients. J Cutan Aesthet Surg. 2014;7(3):143-50.
22. Tang JY, Epstein EH, Oro AE. Basal cell carcinoma and basal cell nevus syndrome. In: Kang S, Amagai M, Bruckner AL, Enk AH, Margolis D, McMichael AJ, et al., editors. Fitzpatrick's dermatology. 9th ed. New York: Mc Graw Hill; 2019. p. 1884-97.
23. Cordova M, Nehal KS, Rossi AM. Basal cell carcinoma: epidemiology; pathophysiology; clinical and histological subtypes; and disease associations. J Am Dermatology. 2019;80(2):303-17.
24. Nahhas AF, Scarbrough CA, Trotter S. A review of the global guidelines on surgical margins for nonmelanoma skin cancers. J Clin Aesthet Dermatol. 2017;10(4):37-46.
25. Peris K, Concetta M, Garbe C, Kaufmann R, Bastholt L, Basset N, et al. Diagnosis and treatment of basal cell carcinoma: european consensus e based interdisciplinary guidelines. Eur J Cancer. 2019;118:10-34.
26. Lee BM, Shim JS, Kim TS, Han DG, Park DH. Clinical consideration of 137 cases of basal cell carcinoma in face. Arch Craniofacial Surg. 2013;14(2):107-10.
27. Haimovic A, Sheehan JM, Rohrer TE. Excisional surgery and repair, flaps, and grafts. In: Kang S, Amagai M, Bruckner AL, Enk AH, Margolis DJ, McMichael AJ, et al., editors. Fitzaptrick's dermatology. 9th ed. New York: Mc Graw Hill; 2019. p. 3726-59.
28. Gualdi G, Monari P, Apalla Z, Lallas A. Surgical treatment of basal cell carcinoma and squamous cell carcinoma. G Ital Dermatol Venereol. 2015;150(4):435-47.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}