


Joana Cruz Matos Calvão da Silva; André Castro Pinho; Ana Maria Carvalho Brinca; Ricardo José David Costa Vieira
Received on: 28/03/2020
Approved on: 29/05/2020
Financial support: None
Conflict of interest: None
Research performed at the Dermatology Service, Centro Hos- pitalar e Universitário de Coimbra, Coimbra, Portugal
Pincer nail is an acquired or hereditary nail deformity, which manifests as a transverse hypercurvature of the nail plate, especially in its distal portion, causing compression of the nail bed, which can provoke pain with functional disability, as well as secondary infections. Conservative treatment is associated with high recurrence rates, so surgical reconstruction is generally necessary. Four exemplary clinical cases of different corrective options of the pincer nail are described.
Keywords: Ambulatory surgical procedures; Nail diseases; Nails malformed
Pincer nail is characterized by a transverse over curvature of the nail plate, which causes compression of the nail bed, especially the distal portion, which can cause pain and secondary infection.1 It is more common in the toes, especially the hallux, but it can also occur in the fingers. The etiology can be hereditary (especially with an autosomal recessive transmission pattern and symmetric involvement of the nails) or acquired (more frequently with an asymmetric topography and secondary to various etiologies, such as tight footwear, osteoarthrosis of the distal interphalangeal joint, psoriasis, subungual exostosis, onychomycosis, tumors of the ungual system, and even some drugs, such as betablockers.2–4
Conservative treatment rarely corrects the deformity completely and is associated with a high recurrence rate. Surgery is thus more useful for better long-term control.5 Various surgical techniques have been described in the literature for correction of this nail deformity.
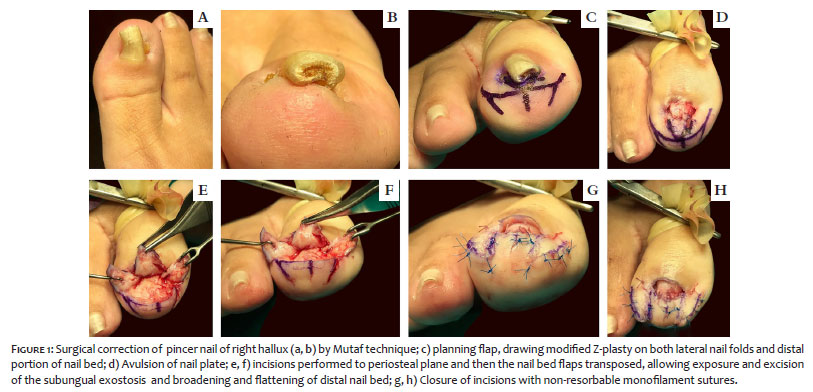
Case 1: Female patient, 45 years, with pincer nail of the right hallux, underwent corrective surgery with the Mutaf technique, consisting of avulsion of the nail plate, removal of the osteophyte on the dorsal surface of the phalanx and transverse broadening of the nail bed via modified Z-plasty applied to each of the lateral folds and the distal portion of the nail bed. Incisions performed up to the periosteal plane and posterior transposition of the nail bed flaps allow broadening and flattening of the distal nail bed (Figure 1).
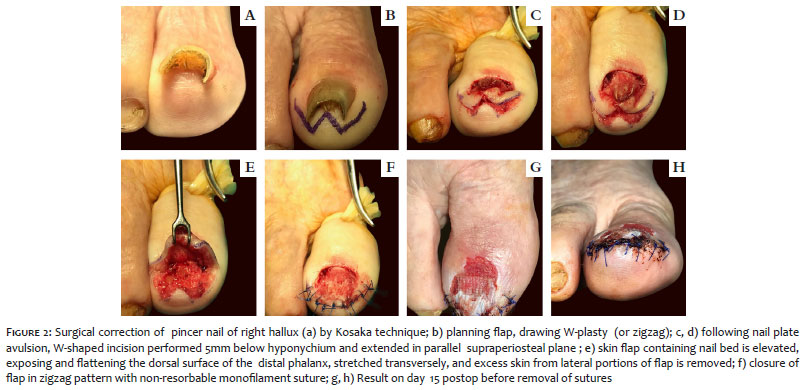
Case 2: Female patient, 84 years, with pincer nail of the right hallux, underwent surgical correction with the Kosaka technique (W or zigzag). In this technique, after avulsion of the nail plate, a W-shaped incision is performed, 5mm below the hyponychium, extending deeply under the nail bed in a supraperiosteal parallel plane. The skin flap containing the nail bed is elevated, stretched in the transverse direction, and the excess skin from the lateral portions of the flap is removed. The dorsal surface of the phalanx is flattened. The flap is then sutured in a zigzag pattern, similar to a classical W-plasty (Figure 2). In addition to the hallux, the technique was also performed on another patient with pincer tail of the second toe, also successfully, showing the technique’s versatility (Figure 3).
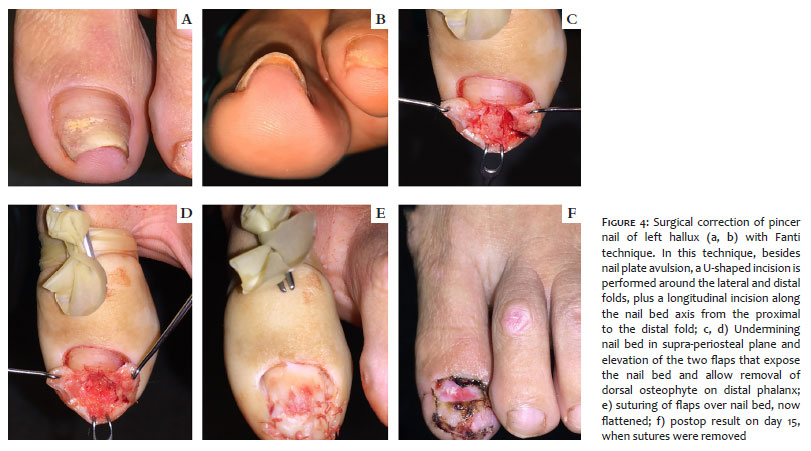
Case 3: Young female, 32 years, with pincer nail of left hallux, underwent Fanti surgical technique (Figure 4), consisting of nail plate avulsion and U-shaped incision around lateral and distal nail folds, plus longitudinal incision along the axis of the nail bed from the proximal to the distal fold. The nail bed is undermined in the supraperiosteal plane, elevating the two flaps to expose the nail bed, allowing removal of the dorsal osteophyte on the distal phalanx. The intervention is finalized by suturing the flaps over the new flattened nail bed.
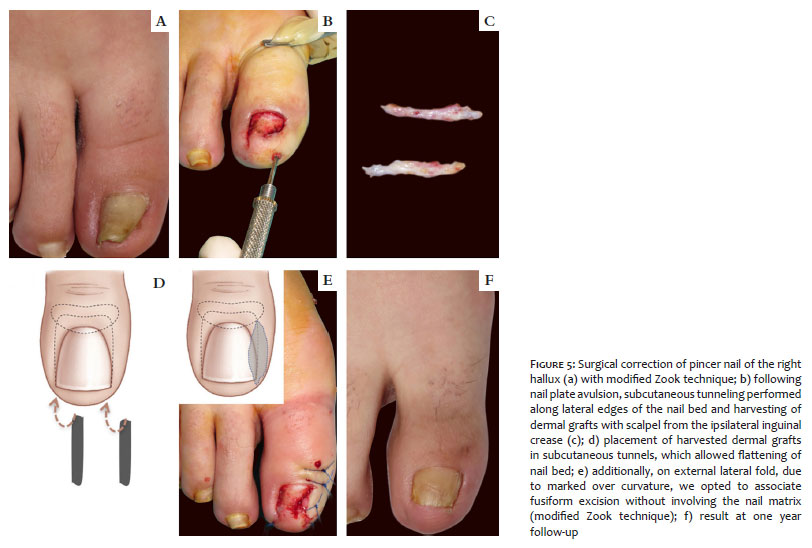
Case 4: Female patient, 30 years, with pincer nail of the right hallux, causing severe pain and functional disability, treated with modified Zook technique, consisting of removal of the nail plate and flattening of the nail bed via skin grafts (harvested with a scalpel from the ipsilateral inguinal crease) in subcutaneous tunnel created along both lateral edges of the nail bed. Additionally, on one of the lateral folds, since there was a marked over curvature, we opted to combine with a fusiform excision without involving the matrix (modified Zook technique) (Figure 5).
All the procedures were performed under distal digital anesthetic block, and there were no immediate or late complications. Antibiotic prophylaxis was performed with a first-generation cephalosporin in all the cases. Instructions to patients included rest and analgesia on the first days postop. The non-resorbable sutures were removed after seven to 15 days. The cosmetic and functional results were good in all the cases, with effective correction of the nail deformity.
Although conservative correction of pincer nail may be useful in mild cases, the high rates of treatment failure and relapse mean that surgical correction is the treatment of choice for this deformity, especially in serious cases with marked functional impact associated with inflammation and/or infection. Multiple corrective surgical techniques have been described, which can be classified as those that include destruction of the nail matrix and techniques that preserve it.
The main advantages of the techniques by Mutaf,6 Kosaka,7 and Fanti1 are preservation of the nail matrix, exposure and destruction of the subungual osteophyte when it exists, and flattening of the nail bed. Still, the technique’s performance involves partial or total avulsion of the nail plate, which increases the complete recovery time. The Zook technique8 does not require removal of the osteophyte, but it is technically more complex and requires the creation of secondary defects in the donor areas for dermal grafts.
I wish to thank my Service and the Director for the opportunity to work there and thus attend the surgeries such as the ones described here, as well as my coauthors, who are an example in dermatologic surgery and who have helped me with the drafting and revision of this article.
Joana Cruz Matos Calvão da Silva | 0000-0002-1161-269X
Approval of the final version of the manuscript; conception and planning of the study; elaboration and writing of the manuscript; data collection, analysis, and interpretation; effective participation in orientation of the research; intellectual participation in the propaedeutic and/or therapeutic conduct of the cases; critical review of the literature; critical revision of the manuscript.
André Castro Pinho | 0000-0001-6433-311X
Approval of the final version of the manuscript; effective participation in orientation of the research; critical revision of the manuscript.
Ana Maria Carvalho Brinca | 0000-0002-7539-9912
Approval of the final version of the manuscript; critical revision of the manuscript.
Ricardo José David Costa Vieira | 0000-0002-5914-9171
Approval of the final version of the manuscript; critical revision of the manuscript.
1. Maria J, Ballavenuto A, Antonio CR, Antonio JR. Tratamento de unha em pinça pela técnica de Fanti. Surg Cosmet Dermatol 2014;6(2):122-5.
2. Brinca A, Pereira N, Vieira R, Figueiredo A. Unha em pinça: correção cirúrgica pela técnica de Zook modificada. Rev Soc Port Dermatol Venereol. 2011;69(4):613-5.
3. Nam HM, Kim UK, Park SD, Kim JH, Park K. Correction of pincer nail deformity using dermal grafting. Ann Dermatol. 2011;23(Suppl. 3):299-302.
4. Baran R, Haneke E, Richert B. Pincer nails: definition and surgical treatment. Dermatologic Surg. 2001;27(3):261-6.
5. Shin WJ, Chang BK, Shim JW, Park JS, Kwon HJ, Kim GL. Nail plate and bed reconstruction for pincer nail deformity. Clin Orthop Surg. 2018;10(3):385-8.
6. Mutaf M, Sunay M, Isik D. A new surgical technique for the correction of pincer nail deformity. Ann Plast Surg. 2007;58(5):496-500.
7. Kosaka M, Asamura S, Wada Y, Kusada A, Nakagawa Y, Isogai N. Pincer nails treated using zigzag nail bed flap method: results of 71 toenails. Dermatologic Surg. 2010;36(4):506-11.
8. Zook EG, Chalekson CP, Brown RE, Neumeister MW. Correction of pincer-nail deformities with autograft or homograft dermis: modified surgical technique. J Hand Surg Am. 2005;30(2):400-3.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}